Airway anatomy Adult vs Pediatric airway Difficult airway assessment, predictors , cart and management MD Anaesthesia pg exam 50 marks major answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
AIRWAY ANATOMY, ADULT vs. PEDIATRIC AIRWAY, DIFFICULT AIRWAY ASSESSMENT, PREDICTORS, CART AND MANAGEMENT
MD Anaesthesia PG Exam - 50 Marks Major Answer
SECTION 1: AIRWAY ANATOMY
Overview
The airway is divided into:
- Upper airway: Nasal cavity, oral cavity, pharynx, larynx
- Lower airway: Trachea, tracheobronchial tree
A detailed understanding of airway anatomy is essential for the anaesthesiologist - it underpins airway assessment, preparation for awake intubation, and the proper use of airway devices. (Miller's Anesthesia, 10e)
1.1 Nasal Cavity
- The airway begins functionally at the naris (external opening).
- Divided into right and left passages by the nasal septum (septal cartilage anteriorly; ethmoid superiorly, vomer inferiorly posteriorly).
- The lateral walls bear three turbinates (conchae) creating three meatuses. The inferior meatus is the preferred pathway for nasal airway devices.
- The roof is formed by the cribriform plate (ethmoid bone) - if fractured, creates a nasocrancial communication with CSF leak; avoid nasopharyngeal airways and NGTs.
- The posterior openings (choanae) lead into the nasopharynx.
- The mucosa is highly vascular; vasoconstrictor must be applied before nasal instrumentation to minimise epistaxis.
- Nasal septal deviation is common - always assess the more patent side.
1.2 Oral Cavity
- The mouth is the preferred conduit for most airway devices.
- Adequate mouth opening requires rotation and protrusion (subluxation) of the mandibular condyles within the temporomandibular joint (TMJ).
- The genioglossus (connects tongue to mandible) is the most clinically relevant extrinsic muscle - jaw thrust moves it anteriorly, relieving obstruction.
- The mylohyoid divides the floor of the mouth into sublingual and submental spaces; infection or haematoma here causes tongue elevation and obstruction (Ludwig's angina).
1.3 Pharynx
A muscular tube extending from the base of skull to the level of the cricoid (C6), connecting nasal/oral cavities with the larynx and esophagus.
| Division | Boundaries | Key Structures |
|---|---|---|
| Nasopharynx | Base of skull to soft palate | Adenoid tonsils, choanae |
| Oropharynx | Soft palate to epiglottis tip | Palatine tonsils, tonsillar pillars, base of tongue, vallecula |
| Hypopharynx (Laryngopharynx) | Epiglottis to cricoid | Piriform fossae, posterior pharyngeal wall |
- The velopharynx (soft palate junction) is a common site of airway obstruction in both awake and anesthetized patients.
- Loss of pharyngeal muscle tone under anaesthesia is a primary cause of upper airway obstruction.
1.4 Larynx
The larynx is a sphincteric organ at the junction of the alimentary and respiratory tracts. It is composed of nine cartilages (3 paired + 3 unpaired):
Unpaired: Thyroid, Cricoid, Epiglottis
Paired: Arytenoids, Corniculate, Cuneiform
Key Cartilages
- Thyroid cartilage: Shield-shaped; the largest cartilage; forms the anterior "protective housing" of the vocal folds. The laryngeal prominence (Adam's apple) marks the midline.
- Cricoid cartilage: The only complete ring in the airway; signet ring-shaped (~1 cm height anteriorly, ~2 cm posteriorly). Basis of cricoid pressure (Sellick's manoeuvre).
- Epiglottis: Leaf-shaped; protects the laryngeal inlet during swallowing.
- Arytenoid cartilages: Paired; move on the cricoid to control vocal cord tension and abduction/adduction.
Cricothyroid Membrane (CTM)
- Joins the inferior edge of thyroid cartilage to the superior surface of the cricoid.
- Dimensions: 8-12 mm wide, 10.4-13.7 mm high.
- Located 1 to 1.5 fingerbreadths below the thyroid notch.
- The central portion is the conus elasticus.
- The site for emergency cricothyrotomy; incisions should be made in the inferior third directed posteriorly (to avoid vocal cords above and cricoid vasculature).
- Ultrasound facilitates identification, especially in obese patients.
Vocal Cords
- Extend from the thyroid cartilage (anteriorly) to the arytenoid cartilages (posteriorly).
- Innervated by the recurrent laryngeal nerve (all intrinsic muscles) except the cricothyroid (external branch of superior laryngeal nerve).
- Unilateral RLN injury: Hoarseness
- Bilateral RLN injury: Complete airway obstruction due to unopposed cord adduction
Laryngeal Innervation
| Nerve | Branch | Supplies |
|---|---|---|
| Superior Laryngeal Nerve (SLN) | Internal branch | Sensory: laryngeal mucosa above vocal cords |
| SLN | External branch | Motor: Cricothyroid muscle |
| Recurrent Laryngeal Nerve (RLN) | - | All other intrinsic muscles + sensory below cords |
1.5 Trachea
- Approximately 15 cm long in adults; 17-18 C-shaped cartilages.
- First tracheal ring is anterior to C6 vertebra in adults.
- Posterior wall is membranous (overlies the esophagus).
- Bifurcates at the carina (level of T5/T6 or sternal angle of Louis) into right and left principal bronchi.
- The right principal bronchus is shorter, wider, and deviates at a less acute angle - aspirated material and deeply inserted ETTs preferentially enter the right side.
SECTION 2: ADULT vs. PEDIATRIC AIRWAY - COMPARATIVE ANATOMY
This is one of the most frequently examined topics in MD Anaesthesia. The following differences are both anatomical and physiological.
Key Comparative Table
| Feature | Adult | Pediatric/Infant/Neonate |
|---|---|---|
| Head size | Proportionate | Large occiput - causes flexion in supine position; shoulder roll needed |
| Tongue | Proportionate to oral cavity | Relatively larger tongue occupies more oropharyngeal space |
| Nose | Nasal breathing optional | Obligate/preferential nasal breather (especially neonates/infants) |
| Laryngeal position (glottis) | C4-C6 (C5-C6 in adults) | C3-C4 in infant; C3 in premature - appears "anterior" = actually cephalad |
| Narrowest point of airway | Glottis (vocal cords) | Subglottis (cricoid ring) - circular, functionally narrowest |
| Epiglottis shape | Flat, broad | Omega/tubular-shaped, longer, narrower, stiffer, difficult to elevate |
| Vocal cord angle | Perpendicular/horizontal | Anteriorly slanted - causes ETT hangup at anterior commissure |
| Aryepiglottic folds | Normal width | Closer to midline - contributes to difficulty in visualisation |
| Tracheal length | ~15 cm | ~4 cm (neonate) - short, right main bronchus intubation more likely |
| Tracheal diameter | 1.5-2 cm | Narrower; small amounts of subglottic oedema cause significant obstruction |
| Airway cartilage | Firm/calcified | Pliable/soft - can collapse |
| FRC/oxygen reserve | Large; allows prolonged apnoea | Low FRC, high metabolic rate - rapid desaturation |
| Compliance | High | Low chest wall compliance, high lung compliance in neonates |
| ETT selection | Cuffed | Traditionally uncuffed (now cuffed acceptable with low cuff pressures) |
Laryngeal Level - Detail
- Normal adult: Glottis at C5-C6
- Full-term infant: C4
- Premature infant: C3
The combination of large tongue + cephalad larynx makes the laryngoscopic line of vision more difficult in infants. The larynx appears anterior but is more accurately described as cephalad.
The "Cone-Shaped vs. Cylindrical" Concept
- Traditional teaching (Eckenhoff): Infant airway is cone-shaped, narrowest at the subglottic cricoid ring - hence uncuffed tubes were preferred.
- Modern evidence (Litman, 2003): The infant larynx is actually cylindrical (not cone-shaped), and the vocal cords are the narrowest point - similar to adults but proportionally smaller. This has supported the use of cuffed ETTs in children with proper cuff pressure monitoring.
Why Infants Desaturate Faster
- High oxygen consumption (~6 mL/kg/min vs ~3 mL/kg/min in adults)
- Low functional residual capacity (FRC)
- High closing capacity (CC can exceed FRC even in awake state)
- Small absolute airway diameter - minor oedema has significant effect
Hagen-Poiseuille Law: Resistance ∝ 1/r⁴. A 1 mm reduction in radius in a 4 mm diameter airway increases resistance by 16-fold vs. only 3-fold in an 8 mm diameter adult airway.
ETT Size in Children
- Uncuffed (traditional formula): Age/4 + 4 (in mm internal diameter)
- Cuffed: Age/4 + 3.5
- Depth of insertion: Age/2 + 12 cm (oral), Age/2 + 15 cm (nasal)
- A leak at 20-25 cm H₂O confirms appropriate uncuffed tube fit.
SECTION 3: DIFFICULT AIRWAY
3.1 Definitions
- Difficult airway (ASA 2022): A clinical situation in which a conventionally trained anaesthesiologist experiences difficulty with face mask ventilation, difficulty with supraglottic airway placement, difficulty with laryngoscopy, difficulty with tracheal intubation, or difficulty with surgical airway access.
- Difficult mask ventilation: Inability to maintain SpO₂ >90% with face mask ventilation in a patient with normal preoperative SpO₂.
- Difficult intubation (DI): Requires >3 attempts or >10 minutes with conventional laryngoscope. Cormack-Lehane (C-L) grade 3 or 4.
- Failed intubation: Inability to place ETT after multiple attempts.
- Cannot Intubate Cannot Oxygenate (CICO): The most life-threatening scenario.
3.2 ASA Difficult Airway Assessment - Step 1
The ASA guidelines recommend assessing for:
- Difficulty with patient cooperation or consent
- Difficult mask ventilation (MOANS)
- Difficult supraglottic airway placement
- Difficult laryngoscopy
- Difficult intubation
- Difficult surgical airway access
SECTION 4: PREDICTORS OF DIFFICULT AIRWAY
4.1 Bedside Screening Tests
A. Modified Mallampati Classification (Samson & Young, 1987)
Patient is seated upright, head neutral, mouth wide open, tongue protruded, no phonation.
| Class | Structures Visible | Predicted Difficulty |
|---|---|---|
| I | Soft palate, fauces, uvula, tonsillar pillars | Easy |
| II | Soft palate, fauces, uvula | Easy-Moderate |
| III | Soft palate + base of uvula only | Moderate-Difficult |
| IV | Hard palate only (soft palate NOT visible) | Difficult |
| 0 | Epiglottis visible | Usually easy (but may be difficult with floppy epiglottis) |
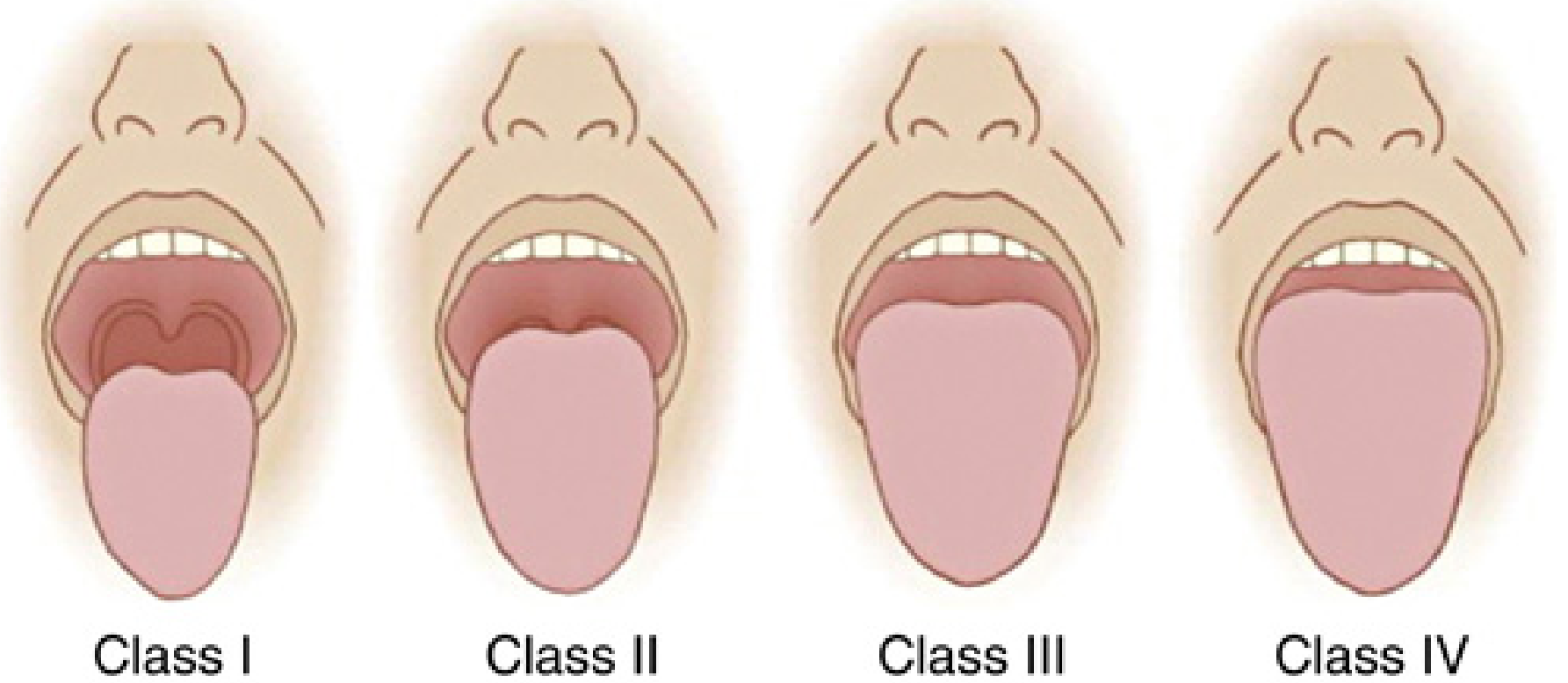
Class III/IV predict difficult direct laryngoscopy. As a standalone test, sensitivity is ~50%, specificity ~80%. Best used in combination.
B. Thyromental Distance (Patil's Test)
- Measured from the thyroid notch to the lower border of chin with head in full extension.
- <6.5 cm (or <3 fingerbreadths) = reduced mandibular (submandibular) space = difficulty displacing tongue during laryngoscopy = anticipated difficult intubation.
C. Sternomental Distance
- From sternal notch to the chin with head fully extended and mouth closed.
- <12.5 cm = predicted difficult intubation.
D. Interincisor Distance (Mouth Opening)
- <3 cm (2 fingerbreadths) = difficult intubation.
- Some studies use <4 cm as the cutoff.
E. Atlantooccipital Extension
- Reduced neck extension is associated with difficult intubation.
- Overall neck ROM <80° is predictive.
- Sniffing position (cervical flexion + atlantooccipital extension) is the ideal for direct laryngoscopy.
F. Upper Lip Bite Test (ULBT)
| Class | Ability | Prediction |
|---|---|---|
| I | Lower incisors bite upper lip above vermilion border | Easy |
| II | Lower incisors bite upper lip below vermilion border | Moderate |
| III | Cannot bite upper lip at all | Difficult |
Higher specificity and lower interobserver variability than Mallampati alone.
G. Neck Circumference
- >43 cm (17 inches) is associated with difficult intubation.
- Neck circumference is a stronger predictor than BMI alone.
4.2 LEMON Assessment (Emergency Medicine / RSI)
A rapid bedside tool for emergency airway assessment:
| Letter | Parameter | Abnormal Finding |
|---|---|---|
| L - Look externally | Facial/neck pathology | Trauma, burns, tumour, beard, large neck |
| E - Evaluate 3-3-2 rule | 3 fingers mouth opening; 3 fingers hyoid to chin; 2 fingers hyoid to thyroid notch | Any <3/3/2 fingers |
| M - Mallampati | Oropharyngeal view | Class III/IV |
| O - Obstruction | Signs of obstruction | Stridor, mass, foreign body, haematoma |
| N - Neck mobility | Ability to flex/extend | Cervical spine disease, collar, burns |
4.3 MOANS - Predictors of Difficult Mask Ventilation
| Letter | Feature |
|---|---|
| M - Mask seal | Beard, facial trauma, craniofacial abnormality |
| O - Obese/Obstruction | BMI >26, obstructing mass |
| A - Age | >55 years |
| N - No teeth | Edentulous (poor seal) |
| S - Snores/Stiff | OSA, stiff lungs (ARDS) |
4.4 RODS - Predictors of Difficult SGA Placement
R - Restricted mouth opening; O - Obstruction; D - Distorted airway; S - Stiff lungs
4.5 SHORT - Predictors of Difficult Surgical/Front-of-Neck Airway
S - Surgery/radiation to neck; H - Haematoma; O - Obesity; R - Radiation changes; T - Tumour/mass
4.6 Cormack-Lehane Grading (Direct Laryngoscopy View)
| Grade | View | Intubation Difficulty |
|---|---|---|
| 1 | Full glottic opening visible | Easy |
| 2a | Posterior portion of glottis visible | Easy-moderate |
| 2b | Only arytenoids visible | Moderate |
| 3 | Only epiglottis visible | Difficult |
| 4 | Neither epiglottis nor glottis visible | Very difficult/impossible |
4.7 Wilson Risk Sum Score
A multivariate scoring system (max 10 points) evaluating: weight, head-neck movement, jaw movement, receding mandible, buck teeth.
- Score ≥2: Predicts 75% of difficult intubations; combined with Mallampati improves predictive power.
4.8 El-Ganzouri Risk Index
Multivariable score including 7 parameters (mouth opening, thyromental distance, Mallampati, neck movement, ability to protrude jaw, weight, history of difficult intubation).
SECTION 5: DIFFICULT AIRWAY CART
The difficult airway cart (trolley) centralises specialised airway equipment in one location for rapid deployment. Equipment should be customised to institutional needs and patient population.
Standard Contents of a Difficult Airway Cart
1. Basic Airway Equipment
- Face masks (all sizes), oral and nasal airways (all sizes)
- Self-inflating (Ambu) bag
- Oxygen source with tubing
2. Supraglottic Airways (SGAs)
- Classic LMA (sizes 1-5)
- Proseal/Supreme/i-gel LMA
- Intubating LMA (ILMA - Fastrach) - allows blind or FOB-guided ETT insertion
- Laryngeal tube / King airway
3. Laryngoscopes and Blades
- Macintosh blades (sizes 2, 3, 4)
- Miller blades (straight, sizes 1, 2, 3)
- McCoy blade (hinged tip)
- Spare batteries and bulbs
4. Video Laryngoscopes (VL)
- GlideScope (hyperangulated)
- C-MAC (Storz)
- McGrath
- Airtraq (optical + camera)
- Storz DCI video laryngoscope
5. Flexible Fiberoptic Bronchoscope (FOB)
- Size 4.0 and 5.0 mm - gold standard for awake difficult intubation
- Light source, camera, screen/monitor
- Anti-fog solution, suction
6. Intubating Aids / Bougies / Stylets
- Eschmann bougie (gum elastic bougie - GEB)
- Cook airway exchange catheter
- Intubating stylet (Frova, Parker)
- Magill forceps
7. Endotracheal Tubes (ETTs)
- Range of cuffed and uncuffed tubes (ID 3.0 - 9.0 mm)
- Reinforced/flexometallic ETTs (for head/neck/airway surgery)
- Microlaryngoscopy tube (MLT)
- Nasal RAE tubes
8. Surgical / Front-of-Neck Access (FONA) Equipment
- Scalpel (#10 or #20 blade)
- 6.0 ETT / tracheostomy tube
- Cricothyrotomy kit (e.g., Melker percutaneous set - both surgical and Seldinger-based)
- Bougie
- Tracheal dilator
- 14G IV catheter (needle cricothyrotomy / transtracheal jet ventilation)
- Jet ventilator / Manujet III
9. Retrograde Intubation Set
- Cook retrograde intubation kit (18G epidural needle, guidewire, catheter)
10. Topicalization Supplies
- Lidocaine 4% (nebulization, mucosal atomization)
- Lidocaine 10% spray
- Mucosal Atomization Device (MAD)
- Cricothyroid membrane puncture kit for transtracheal block
- Cocaine 4% spray (for nasal topicalization - both vasoconstrictor and local anaesthetic)
11. Drugs
- Sedatives: Midazolam, Dexmedetomidine, Ketamine
- Muscle relaxants: Succinylcholine, Rocuronium
- Reversal: Sugammadex (for rocuronium reversal)
- Vasoconstrictors: Ephedrine, Phenylephrine
- Anticholinergics: Glycopyrrolate (drying agent for awake FOB)
12. Monitoring and Confirmation
- Waveform capnography (ETCo₂)
- Colorimetric CO₂ detector
- Pulse oximetry
13. Cognitive Aids
- Laminated ASA/DAS difficult airway algorithm
- VORTEX approach card
- Airway checklist
SECTION 6: MANAGEMENT OF THE DIFFICULT AIRWAY
6.1 Core Principles (ASA 2022 / DAS 2015)
- Assess the likelihood of all difficulties (ventilation, SGA, laryngoscopy, intubation, surgical airway).
- Supplement oxygen throughout the entire process (apnoeic oxygenation via high-flow nasal oxygen - HFNO, e.g., 15 L/min via nasal cannula).
- Consider awake intubation vs. intubation after induction.
- Consider video-assisted laryngoscopy as the primary initial approach.
- Never make more than 3 attempts with the same technique.
- Develop primary and alternative strategies before starting.
- Call for help early.
6.2 The Fundamental Decision: Awake vs. Asleep
| Factor | Awake Intubation Favoured | Asleep Intubation Feasible |
|---|---|---|
| Airway predictors | Multiple predictors positive | Few/no predictors |
| Mask ventilation | Likely difficult | Likely easy |
| Full stomach/aspiration risk | Yes | No |
| Cervical spine instability | Yes | No |
| Cooperative patient | Yes | - |
| Critical anatomy | Yes (airway tumour, abscess) | - |
6.3 Awake Intubation (Gold Standard for Anticipated Difficult Airway)
Indication: Any anticipated difficult airway where mask ventilation is also expected to be difficult.
Technique Steps:
- Pre-oxygenation - 3-5 minutes high-flow O₂ or 8 vital capacity breaths.
- Antisialogogue - Glycopyrrolate 0.2 mg IV (10 minutes before) to reduce secretions and improve topicalization.
- Sedation - Dexmedetomidine infusion (0.7-1 mcg/kg over 10 min) OR Midazolam 1-2 mg + Fentanyl 25-50 mcg; keep patient awake and cooperative. Ketamine also used.
- Topical anaesthesia:
- Mouth/tongue: Lidocaine 4% nebulization (4 mL over 15 min) or benzocaine spray
- SLN block: Lidocaine 2% injection lateral to hyoid cornua bilaterally
- Transtracheal block: 3-4 mL lidocaine 2% injected through CTM, patient coughs to spread
- Nasal: Lidocaine + oxymetazoline (vasoconstrictor) applied with pledgets
- Fiberoptic intubation (FOB): Advance scope through vocal cords under vision, railroad ETT over scope.
- Alternative techniques: Awake video laryngoscopy (if anatomy permits), awake blind nasal intubation (less preferred).
6.4 ASA Difficult Airway Algorithm
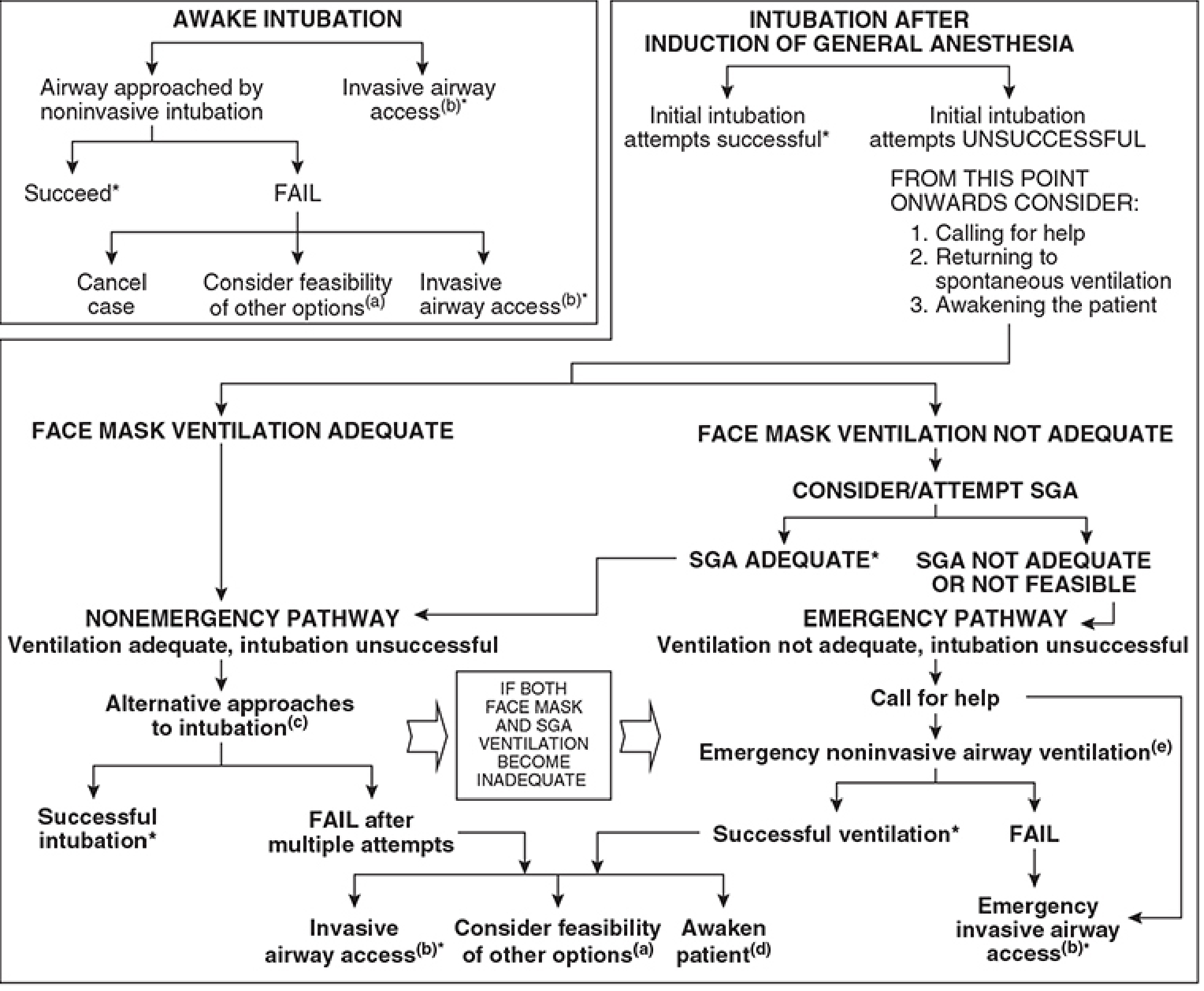
The algorithm has two main pathways after induction:
Non-Emergency Pathway (Ventilation adequate, intubation unsuccessful):
- Alternative approaches to intubation:
- Video laryngoscopy
- Alternative blades (Miller, McCoy, Bullard)
- Fiberoptic intubation
- SGA as intubating conduit (ILMA + FOB)
- Intubating bougie/stylet
- Blind oral/nasal intubation
- Cancel surgery, awaken patient, reattempt awake
- Invasive airway access if alternatives fail
Emergency Pathway (Cannot Intubate, Cannot Oxygenate - CICO):
- Call for help immediately
- Emergency SGA (LMA) as temporising measure
- If SGA fails → Emergency Front-of-Neck Access (eFONA)/Cricothyrotomy
6.5 VORTEX Approach (Chrimes, 2016)
A structured cognitive tool for high-acuity airway management. Visual "vortex cone" representing escalating urgency:
The three "lifelines" (best attempt at each):
- Face mask ventilation (Best attempt: optimal head position, 2-person, airway adjuncts, jaw thrust)
- SGA (Best attempt: optimal size/type, jaw thrust, head position)
- Endotracheal tube (Best attempt: VL, optimal positioning, bougie, BURP)
If all three lifelines fail → Green Zone = CICO = Immediate eFONA
6.6 DAS (Difficult Airway Society) Algorithm - Unanticipated Difficult Intubation
Plan A: Optimise direct laryngoscopy (sniffing position, McCoy blade, BURP)
- Max 3 attempts per plan
- One attempt may be by a more experienced colleague
Plan B: Supraglottic airway device (Proseal/Supreme LMA)
- If successful → maintain oxygenation; decide to proceed with LMA/awaken
Plan C: Revert to face mask, awaken patient
- Awaken if SpO₂ maintained; reattempt with different strategy
Plan D: Emergency Front-of-Neck Access (eFONA)
- Scalpel-bougie-tube technique (preferred):
- Horizontal stab incision through CTM with #10 scalpel
- Dilate with bougie with curved end directed caudally
- Railload 6.0 mm cuffed ETT over bougie
- Inflate cuff, confirm with capnography
- Needle cricothyrotomy (temporary, children/bridge):
- 14G cannula-over-needle into CTM
- Jet ventilation at 50 psi (beware barotrauma, hypercapnia)
- Maximum 30-45 minutes bridge only
6.7 Front-of-Neck Access (FONA) - Details
| Technique | Approach | Rate | Notes |
|---|---|---|---|
| Surgical (scalpel-bougie-tube) | Horizontal CTM incision | Fastest | DAS preferred; gold standard eFONA |
| Percutaneous Seldinger (Melker) | Needle → guidewire → dilator → tube | Moderate | Lower urgency situations |
| Needle (cannula-over-needle) | 14G IV catheter | Fastest temporary | Jet ventilation only; CO₂ retention risk |
| Surgical tracheostomy | Formal | Slowest | Elective; by surgeon |
6.8 Management of Specific Difficult Airway Scenarios
Obese Patient
- Ramped position (ear-to-sternal-notch alignment) instead of sniffing position
- High FiO₂ preoxygenation + CPAP/PEEP
- Rapid desaturation - HFNO apnoeic oxygenation
- Video laryngoscope as first choice
Known Difficult Airway (Elective)
- Awake FOB intubation is the gold standard
- Multidisciplinary planning
- Tracheostomy under LA if intubation expected to be impossible
- Post-operative monitoring in PACU/ICU
Obstetric Difficult Airway
- RSI mandatory (full stomach risk)
- Failed intubation rate 1:300 (vs. 1:2000 in general population) in obstetrics
- If failed intubation: oxygenate via SGA (Proseal LMA), proceed with surgery if mother/fetus in danger; awaken if time permits
Cervical Spine Injury
- In-line stabilisation (MILS) - do not extend neck
- Awake video laryngoscopy or awake FOB preferred
- Manual in-line stabilisation reduces movement during direct laryngoscopy
Paediatric Difficult Airway
- Ask for help before starting
- Use supplemental O₂ during and between attempts
- Use video laryngoscopy for the first attempt
- Do NOT persist with failing techniques
- Complications highest in children <10 kg and with short thyromental distance
- Emergency front-of-neck access in children: surgical tracheotomy preferred over cricothyrotomy (CTM small/non-palpable in <8 years)
SECTION 7: EXTUBATION AFTER DIFFICULT INTUBATION
Extubation carries equal or greater risk than intubation in the difficult airway patient.
Strategy
- Plan extubation before it occurs - document plan.
- Ensure patient is awake, cooperative, following commands, has adequate neuromuscular function (TOF ratio >0.9).
- Consider airway exchange catheter (AEC) placement before extubation - allows reintubation if needed.
- Extubate over AEC and leave in place for 60-90 minutes.
- Have all equipment ready at bedside (video laryngoscope, bougie, emergency drugs).
- Consider delayed extubation in ICU if anatomy is distorted (post-op oedema, haematoma).
- Heliox (helium/oxygen mixture) can reduce work of breathing in post-extubation stridor.
DAS Extubation Guidelines
- Low risk: Standard extubation technique with precautions
- At-risk: Extubation over AEC; awake extubation
- High risk / CICO recurrence risk: Tracheostomy, planned delayed decannulation
SUMMARY TABLE: DIFFICULT AIRWAY MNEMONICS AT A GLANCE
| Mnemonic | Purpose |
|---|---|
| LEMON | Rapid difficult intubation assessment (Look, Evaluate 3-3-2, Mallampati, Obstruction, Neck) |
| MOANS | Difficult mask ventilation (Mask seal, Obese, Age >55, No teeth, Snores) |
| RODS | Difficult SGA (Restricted opening, Obstruction, Distorted, Stiff) |
| SHORT | Difficult surgical airway (Surgery, Haematoma, Obese, Radiation, Tumour) |
| VORTEX | High-acuity emergency management algorithm |
| HEAVEN | Difficult video laryngoscopy (Hypoxaemia, Extremes of size, Anatomical challenge, Vomit/blood, Exsanguination, Neck mobility) |
KEY POINTS FOR EXAM
- The cricoid cartilage is the only complete ring in the airway - it is the narrowest point in the adult airway but the subglottis (around the cricoid level) is the functionally narrowest in neonates.
- Mallampati classification requires: seated upright, neutral head, maximum mouth opening, tongue protruded, no phonation.
- Predictors of difficult intubation: Thyromental distance <6.5 cm, interincisor distance <3 cm, sternomental distance <12.5 cm, neck circumference >43 cm, Mallampati III/IV.
- Awake FOB intubation is the gold standard for the anticipated difficult airway.
- Scalpel-bougie-tube technique through the CTM is the DAS-preferred eFONA in adults.
- In CICO: Call for help → SGA → if failed → immediate cricothyrotomy.
- 3 attempts maximum with any single technique before moving to the next plan.
- Post-difficult intubation: document, label, communicate to patient (difficult airway alert bracelet + medical record).
- Infant larynx is at C3-C4; appears anterior but is actually cephalad.
- Infants have high O₂ consumption + low FRC = rapid desaturation; pre-oxygenation is critical and time-limited.
Sources: Miller's Anesthesia 10e (Hagberg, Chapter 40); Barash Clinical Anesthesia 9e (Chapter 28); Morgan & Mikhail's Clinical Anesthesiology 7e (Chapter 19); Fishman's Pulmonary Diseases and Disorders; Barash Pediatric Anaesthesia Chapters.
This is a shared conversation. Sign in to Orris to start your own chat.