Hypoalbuminemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypoalbuminemia" AND "clinical outcomes"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to write a thorough response. Let me compile everything:
Hypoalbuminemia
Definition
Hypoalbuminemia is defined as a serum albumin below 3.5 g/dL (35 g/L). Severe hypoalbuminemia is generally taken as < 2.5 g/dL (25 g/L). Normal albumin production by the liver is 12-14 g/day (130-200 mg/kg/day).
Causes
Hypoalbuminemia arises from one or more of four main mechanisms:
1. Decreased Hepatic Synthesis
- Liver disease (cirrhosis, hepatitis, hepatic failure) - most common chronic cause
- Malnutrition / protein-energy undernutrition - inadequate amino acid substrate
- Acute-phase response / inflammation - IL-6 and TNF suppress albumin mRNA transcription (albumin is a negative acute-phase reactant)
- Malabsorption syndromes - celiac disease, Crohn's disease, short bowel syndrome
2. Increased Losses
- Nephrotic syndrome - urinary albumin loss > 3.5 g/day; albumin accounts for > 80% of excreted proteins
- Protein-losing enteropathy - IBD, intestinal lymphangiectasia, Menetrier's disease
- Burns / exfoliative skin disease - transdermal protein losses
- Large-volume hemorrhage or drainage (ascitic tap, pleural drainage)
3. Increased Catabolism / Distribution
- Sepsis / critical illness - capillary leak moves albumin into the interstitial space (third-spacing); increased catabolism
- Post-surgical state - rapid post-operative falls are almost always due to redistribution/capillary leak, not decreased synthesis
- Hyperthyroidism
4. Dilutional
- Fluid overload / aggressive IV hydration
- SIADH
- Pregnancy (physiological, due to expanded plasma volume)
Pathogenesis in Nephrotic Syndrome (Best Studied Model)
Hypoalbuminemia in nephrotic syndrome results from multiple simultaneous alterations:
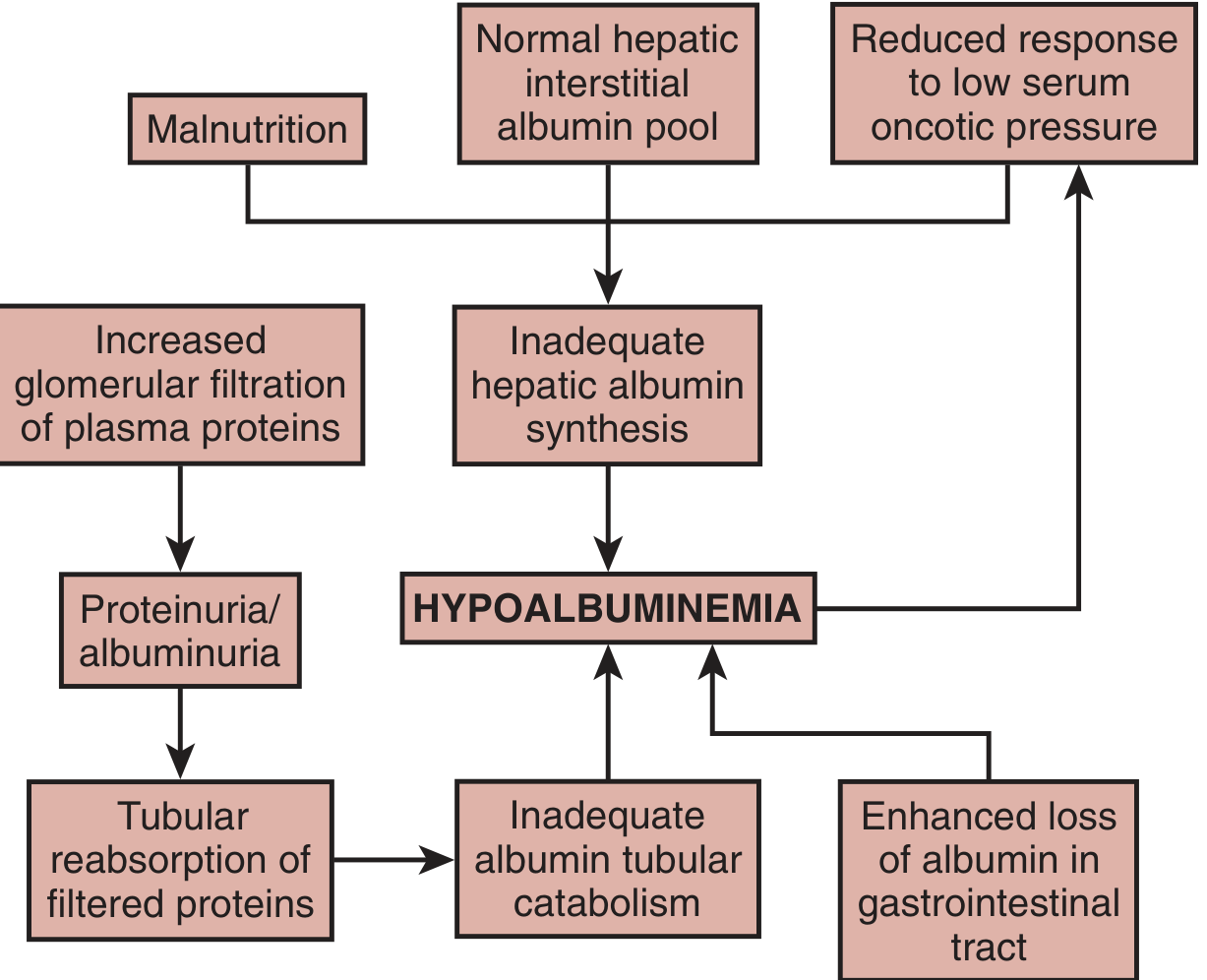
Fig. 30.10 - Brenner and Rector's The Kidney: Schematic representation of mechanisms leading to nephrotic hypoalbuminemia. Compensatory mechanisms are insufficient to correct the hypoalbuminemia.
- Urinary albumin loss - the direct driver, but not sufficient alone
- Inadequate hepatic synthetic response - though the liver CAN increase albumin synthesis up to 300%, in nephrotic patients this response is blunted; the hepatic interstitial albumin pool remains relatively normal, so the liver does not "sense" the degree of systemic depletion
- Increased tubular catabolism - a high-capacity, low-affinity tubular transport system allows increased reabsorption and catabolism of filtered albumin as the filtered load rises
- Malnutrition - low dietary protein further impairs hepatic albumin mRNA expression and synthesis
- Brenner and Rector's The Kidney, p. 1313-1315
- Comprehensive Clinical Nephrology 7e, p. 240
Consequences and Clinical Effects
Edema Formation
Hypoalbuminemia lowers plasma oncotic pressure, shifting the Starling forces in favor of fluid transudation into the interstitium. Two mechanisms operate in nephrotic syndrome:
- Underfill: Low oncotic pressure → decreased circulating volume → RAAS activation → aldosterone-driven sodium retention → worsening edema
- Overfill (more common): Primary ENaC activation in the distal nephron by proteolytic enzymes → sodium/water retention → increased blood volume + low oncotic pressure → transudation
Renal Function
- Impaired sodium and fluid homeostasis
- Reduced GFR: in minimal change and membranous nephropathy, this is due to lowered glomerular hydraulic permeability from podocyte foot process effacement; the fall in GFR is partially offset by elevated net ultrafiltration pressure from reduced intraglomerular oncotic pressure
Hypocalcemia
- Total calcium is low because ~50% is protein-bound; ionized calcium is usually normal
- However, some nephrotic patients have true hypocalcemia due to urinary loss of vitamin D-binding protein → vitamin D deficiency → secondary hyperparathyroidism
- Formula: corrected Ca²⁺ = measured Ca + 0.8 × (4.0 - albumin in g/dL)
Hypercoagulability
- Loss of anticoagulant proteins (antithrombin III, protein C, protein S) in urine
- Elevated fibrinogen and clotting factors (large molecules retained) → net prothrombotic state
- Increased risk of DVT, PE, renal vein thrombosis
Hyperlipidemia
- Reduced oncotic pressure stimulates non-discriminatory hepatic protein synthesis → increased VLDL and LDL production
- Reduced lipoprotein lipase activity (loss of enzyme cofactors in urine)
Drug Pharmacokinetics
Albumin is the major carrier protein for many drugs. In hypoalbuminemia:
- Fewer binding sites → increased free drug fraction → enhanced pharmacological (and toxic) effects at standard doses
- Especially affects highly protein-bound drugs: phenytoin, warfarin, valproate, furosemide, NSAIDs, salicylates
- At steady state, faster drug metabolism partially compensates, but caution is still required
- Etomidate: decreased protein binding in hypoalbuminemia enhances its pharmacological effects
- Goldman-Cecil Medicine, p. 1071; Morgan & Mikhail's Clinical Anesthesiology 7e
Negative Nitrogen Balance / Muscle Wasting
- Heavy proteinuria causes marked negative nitrogen balance
- Loss of 10-20% lean body mass can occur in nephrotic syndrome, often masked by edema
- Albumin turnover is increased due to tubular catabolism of filtered protein
Impaired Immune Function
- Loss of immunoglobulins and complement factors in urine (in nephrotic syndrome)
- Increased susceptibility to infections, especially encapsulated organisms (Streptococcus pneumoniae)
Wound Healing / Surgical Risk
- Post-surgical hypoalbuminemia is an ominous prognostic finding
- Associated with poor wound healing, pressure ulcers, and increased morbidity
- Albumin infusions do not improve survival; the priority is nutritional support, skin integrity, minimizing diuretics
Clinical Signs
| Sign | Detail |
|---|---|
| Pitting edema | Peripheral, periorbital, ascites, pleural effusions |
| Muehrcke lines | Paired white transverse bands on nails - characteristic sign of hypoalbuminemia; the white bands grew during the period of low albumin |
| Muscle wasting | May be masked by edema |
| Signs of underlying cause | Jaundice (liver disease), ascites, cachexia (malignancy), diarrhea (enteropathy) |
Investigations
- Serum albumin (direct measurement)
- 24-hour urine protein or spot urine protein:creatinine ratio (nephrotic syndrome)
- LFTs / synthetic function (PT, INR, bilirubin) - liver disease
- Stool alpha-1 antitrypsin - protein-losing enteropathy
- CRP / ESR - inflammatory/acute-phase state
- Lipid profile, coagulation studies (antithrombin III)
- Serum calcium (corrected), vitamin D levels
- CBC, albumin-to-creatinine ratio
Management
Management is directed at the underlying cause:
| Cause | Treatment |
|---|---|
| Nephrotic syndrome | Immunosuppression (steroids, etc.), ACE inhibitors/ARBs to reduce proteinuria, diuretics for edema |
| Liver disease | Treat underlying hepatic pathology; salt restriction; diuretics for ascites |
| Malnutrition | Nutritional supplementation (enteral > parenteral); adequate protein intake (1.0-1.5 g/kg/day) |
| Sepsis/critical illness | Treat infection; nutritional support |
| Protein-losing enteropathy | Treat underlying GI disease |
Albumin infusion:
- Adult: 25 g IV over 30-120 min; repeat every 1-2 days PRN (max 2 g/kg/24h)
- Child: 0.5-1 g/kg/dose IV over 30-120 min; repeat every 1-2 days PRN
- Hypovolemia: 0.5-1 g/kg IV rapid infusion; may repeat after 15-30 min
- Contraindicated in CHF or severe anemia; can cause fluid overload
- Important caveat: albumin infusions do not correct the underlying metabolic abnormality and have NOT been shown to improve survival in surgical/critically ill patients; they are best used for specific indications (spontaneous bacterial peritonitis, large-volume paracentesis, hepatorenal syndrome)
- Harriet Lane Handbook 23e, p. 1001
Drug dosing adjustments: Review all highly protein-bound medications and consider dose reduction; monitor for toxicity especially with narrow therapeutic index drugs (phenytoin - use free phenytoin levels; warfarin - close INR monitoring).
Recent Evidence
A 2026 systematic review (PMID: 41945558) found that preoperative hypoalbuminemia is significantly associated with worse clinical outcomes after total hip or knee arthroplasty, reinforcing its role as a key surgical risk marker. A 2025 systematic review (PMID: 39645428) addressed perioperative albumin administration in liver transplantation, noting benefit in specific high-risk contexts.
Sources: Brenner and Rector's The Kidney (2-Vol Set) | Comprehensive Clinical Nephrology 7e | Goldman-Cecil Medicine | Morgan & Mikhail's Clinical Anesthesiology 7e | Harriet Lane Handbook 23e | Mulholland & Greenfield's Surgery 7e | Robbins & Cotran Pathologic Basis of Disease
Abruptdopamine signelling
Reading File
Finding Sources
Finding Sources
Searching the Web
abrupt dopamine signalling neuroscience meaning
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a thorough answer. Note that "abrupt dopamine signalling" almost certainly refers to phasic (abrupt/burst) dopamine signaling - the term used in neuroscience for the sudden, brief bursts of dopamine release as opposed to the slow, baseline tonic mode.
Dopamine Signalling - Phasic ("Abrupt") vs Tonic Modes
Note on terminology: "Abrupt dopamine signalling" is not a standard single term in neuroscience. Based on the context, this most likely refers to phasic dopamine signalling - the abrupt, burst-mode firing of dopamine neurons that encodes reward, salience, and prediction error. The full picture of dopamine signalling is covered below, with phasic signalling as the central focus.
1. Dopamine - Overview
Dopamine (DA) is a catecholamine neurotransmitter acting primarily on G protein-coupled receptors. The highest concentrations are in the brain, but DA also exists peripherally in the adrenal medulla, GI plexuses, and the enteric nervous system. There are 5 DA receptor subtypes (D1-D5), grouped into two families:
| Family | Receptors | G-protein | Effect on cAMP | Key locations |
|---|---|---|---|---|
| D1-like | D1, D5 | Gs | ↑ cAMP (adenylyl cyclase activation) | Striatum, prefrontal cortex, limbic system |
| D2-like | D2, D3, D4 | Gi | ↓ cAMP (adenylyl cyclase inhibition) | Striatum, mesolimbic, tuberoinfundibular |
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
2. Synthesis and Life Cycle of Dopamine
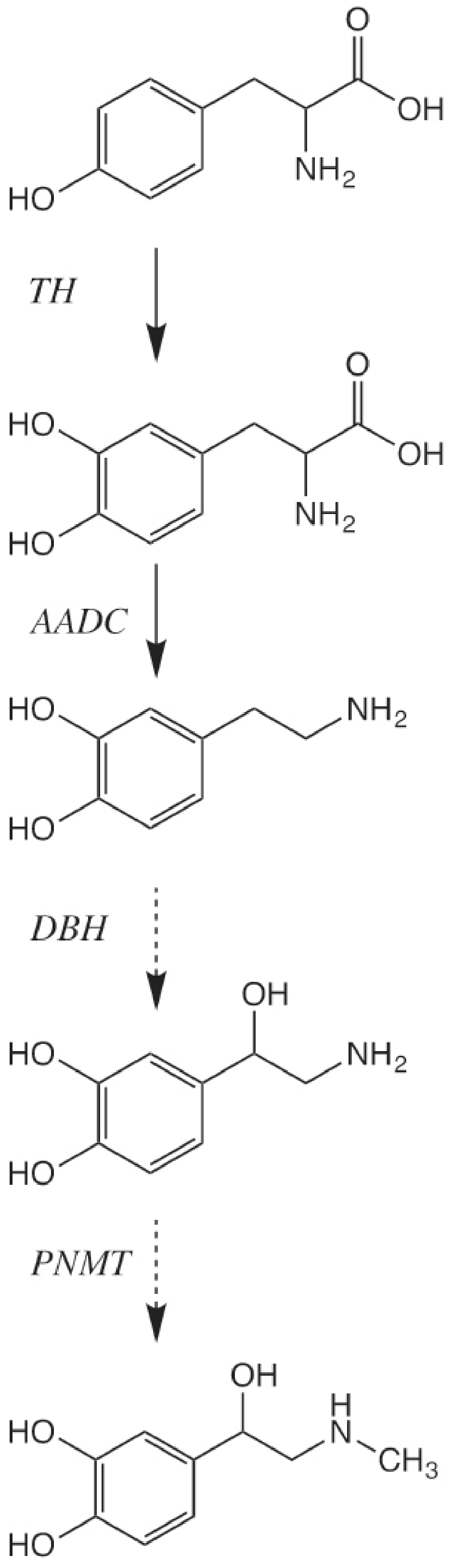
Fig. 1.7-1 - Kaplan & Sadock: Biosynthesis of dopamine, norepinephrine, and epinephrine.
Step-by-step synthesis:
- Tyrosine (from dietary protein/phenylalanine) enters neurons via LNAA transporter
- Tyrosine → L-DOPA via tyrosine hydroxylase (TH) - the rate-limiting step; requires tetrahydrobiopterin cofactor
- L-DOPA → Dopamine via aromatic amino acid decarboxylase (AADC) in the cytosol
- Dopamine is packaged into vesicles by VMAT-2 (vesicular monoamine transporter-2), protecting it from cytoplasmic MAO degradation
Termination of dopamine action:
- Reuptake via the dopamine transporter (DAT) - the primary mechanism
- MAO (monoamine oxidase) degrades cytoplasmic dopamine → DOPAC
- COMT (catechol-O-methyltransferase) in the synapse/postsynaptic cell → HVA (homovanillic acid)
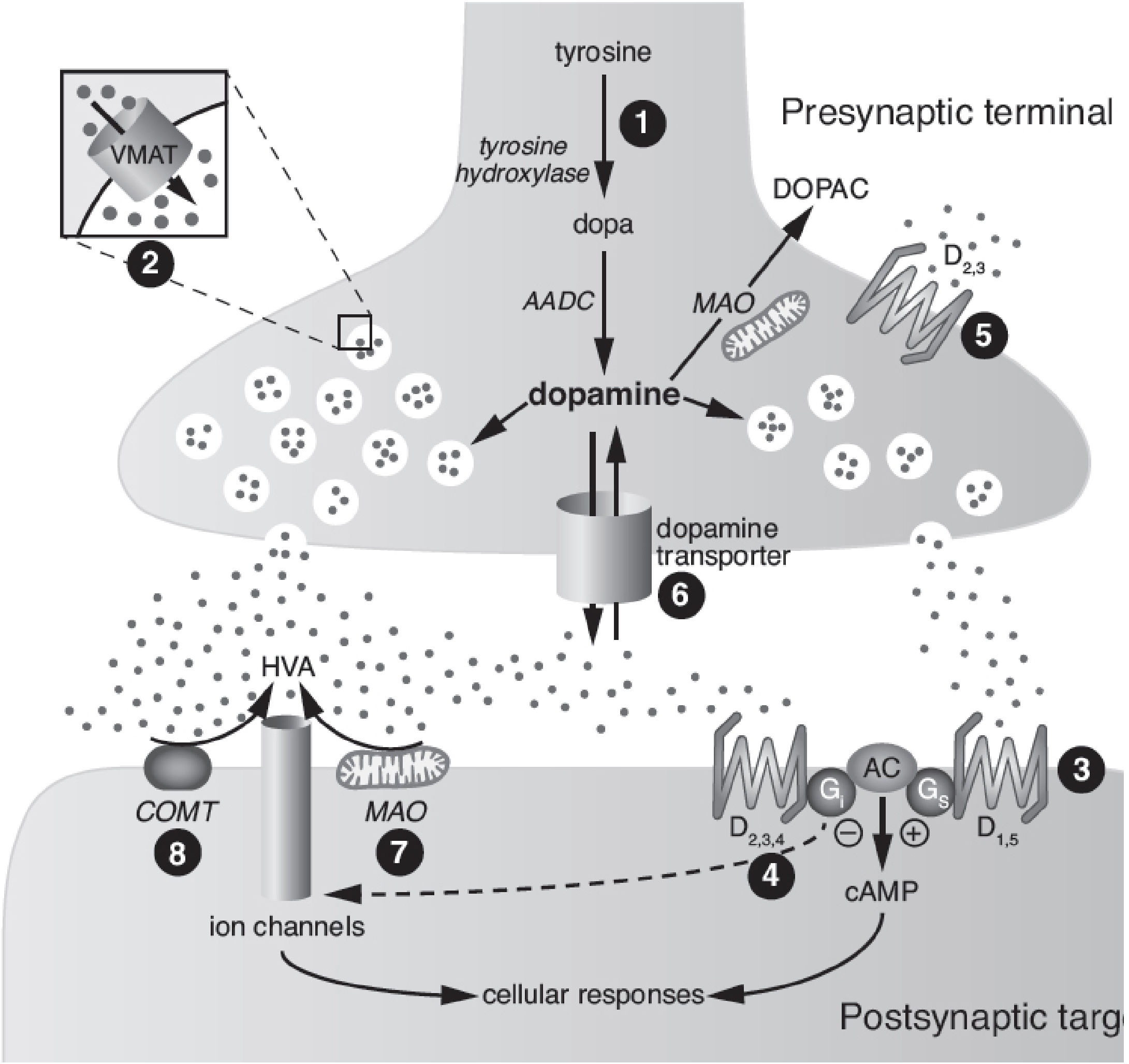
Fig. 1.7-2 - Kaplan & Sadock: Schematic of a dopaminergic synapse with numbered drug action sites.
3. Tonic vs Phasic Dopamine Signalling
Dopamine neurons operate in two fundamentally different firing modes:
Tonic (Baseline) Mode
- Slow, pacemaker-like spontaneous firing (~2-5 Hz)
- Maintains a low, steady baseline of extracellular dopamine
- Preferentially activates high-affinity D3 receptors first, then D2, and last D1
- Functions: sets the background "tone" for motor function, motivation, cognition
- Loss of tonic DA is the basis of Parkinson disease and can be restored by L-DOPA
Phasic ("Abrupt") Mode - The Central Concept
- Burst firing of dopamine neurons - short, rapid volleys (~100 ms duration, ~100 ms latency from stimulus)
- Releases a flurry of dopamine that recruits all three DA receptor subtypes (D1, D2, D3)
- Triggered by: unexpected reward, novel stimuli, salient sensory events, or stimuli that predict reward
- Encodes the reward prediction error (RPE) signal:
- Reward better than predicted → phasic DA burst (positive RPE)
- Reward as predicted → no change in DA firing
- Expected reward omitted → transient dopamine neuron pause (negative RPE)
"The phasic activity of midbrain dopaminergic neurons provides a teaching signal for reinforcement learning." - Kandel's Principles of Neural Science, 6th ed.
-
Tonic and phasic modes operate as a continuum: the post-burst elevation in extracellular DA can sustain tonic DA function, linking the two modes
-
Stahl's Essential Psychopharmacology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
4. Major Dopamine Pathways
| Pathway | Origin → Target | Key Functions | Clinical Relevance |
|---|---|---|---|
| Mesolimbic | VTA → Nucleus accumbens, limbic | Reward, motivation, emotion | Addiction, schizophrenia (positive symptoms) |
| Mesocortical | VTA → Prefrontal cortex | Working memory, attention, executive function | Schizophrenia (negative/cognitive symptoms), ADHD |
| Nigrostriatal | Substantia nigra pars compacta → Striatum | Motor control, action selection | Parkinson disease, drug-induced EPS |
| Tuberoinfundibular | Hypothalamus → Pituitary | Inhibits prolactin release | D2 antagonists → hyperprolactinemia |
5. Phasic DA in the Basal Ganglia - Reinforcement Learning
The basal ganglia use phasic DA as an eligibility trace mechanism:
- A behavior is initiated, leaving an "eligibility trace" in recently active striatal neurons
- If the behavior leads to unexpected reward, a phasic DA burst is broadcast widely
- Only neurons carrying the eligibility trace are potentiated (by simultaneous phasic DA + glutamate)
- This strengthens the direct pathway (D1-expressing neurons → "Go" signal) for that behavior
- Future action selection is biased toward reward-predicting options
The indirect pathway (D2-expressing neurons → "No-Go" signal) is suppressed by phasic DA, releasing the brake on selected actions.
This mechanism underlies:
- Habit formation
- Drug addiction (drugs of abuse hijack phasic DA signaling - see below)
- Kandel's Principles of Neural Science, 6th ed., p. 992-993
6. Phasic DA and Addiction
"The time course of dopamine signalling is a key factor. Rapid phasic dopamine neuronal firing encodes the reward experience and value and is necessary to learn the association of stimuli with reward." - Kaplan & Sadock's
- Drugs of abuse (cocaine, amphetamine, opioids) produce abnormally large, rapid phasic DA surges in the nucleus accumbens
- This overwhelms normal reward circuitry, creating pathologically strong associations (conditioned cues)
- Cocaine blocks DAT → prolongs DA in the synapse
- Amphetamine reverses VMAT-2 and DAT → floods the synapse with DA (non-exocytotic release)
- The rate of DA rise matters: fast IV/smoked administration = greater abuse potential than slow oral routes
- Immediate-release stimulants (methylphenidate, amphetamine) amplify both tonic AND phasic DA signals; their abuse potential is linked to this phasic amplification - Stahl's Essential Psychopharmacology
7. Phasic DA in ADHD
In ADHD, both tonic and phasic DA are hypothetically reduced in the prefrontal cortex:
- Low tonic DA → inadequate D1 stimulation → impaired working memory and attention
- Impaired phasic DA → poor reward-based learning and motivation
Therapeutic goal: stimulants at therapeutic doses modestly enhance tonic DA (improving PFC function) without over-amplifying phasic DA (which would increase abuse potential). Slow-onset, long-duration formulations (extended-release methylphenidate, lisdexamfetamine) preferentially enhance tonic over phasic DA - Stahl's Essential Psychopharmacology
8. Receptor-Level Signal Transduction (Intracellular)
| Receptor | Pathway | Downstream Effects |
|---|---|---|
| D1/D5 (Gs) | ↑ cAMP → PKA activation | Phosphorylation of DARPP-32, AMPA/NMDA receptors; long-term potentiation |
| D2/D3/D4 (Gi) | ↓ cAMP → ↓ PKA | Reduced neuronal excitability; autoreceptor feedback inhibition of DA release |
| D2 (β-arrestin) | Non-canonical pathway | Akt inhibition, ERK activation (independent of cAMP) |
D2 autoreceptors on presynaptic terminals act as a negative feedback brake: when synaptic DA rises, D2 autoreceptors reduce further release.
9. Pharmacological Targets
| Drug / Drug Class | Mechanism | Clinical Use |
|---|---|---|
| L-DOPA + carbidopa | TH bypass; peripheral AADC inhibition | Parkinson disease |
| D2/D3 agonists (pramipexole, ropinirole) | Mimic DA at receptors | Parkinson disease, restless legs |
| D2 antagonists (haloperidol, chlorpromazine) | Block mesolimbic/mesocortical D2 | Antipsychotics (schizophrenia) |
| Cocaine | DAT blockade | Drug of abuse |
| Amphetamine/methylphenidate | DAT blockade + VMAT-2 reversal / DAT blockade | ADHD, narcolepsy; abuse |
| MAO-B inhibitors (selegiline, rasagiline) | Block DA catabolism | Parkinson disease |
| Reserpine/tetrabenazine | VMAT-2 inhibition → depletes DA stores | Huntington chorea; hyperkinetic disorders |
10. Clinical Disorders Involving Abnormal DA Signalling
| Disorder | DA Abnormality |
|---|---|
| Parkinson disease | Loss of nigrostriatal dopamine neurons (tonic DA deficiency) |
| Schizophrenia | Excess mesolimbic phasic DA (positive symptoms); deficit in mesocortical DA (negative/cognitive symptoms) |
| ADHD | Reduced tonic (and phasic) DA in PFC |
| Addiction | Pathologically amplified phasic DA bursts hijack reinforcement learning |
| Depression | Reduced mesolimbic DA (anhedonia) |
| Hyperprolactinemia | Loss of tuberoinfundibular DA (e.g., from D2 antagonist drugs) |
Sources: Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Kandel's Principles of Neural Science 6e | Stahl's Essential Psychopharmacology | Goodman & Gilman's Pharmacological Basis of Therapeutics
Restless leg syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"restless legs syndrome" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it:
Restless Legs Syndrome (RLS) / Willis-Ekbom Disease
Definition & Overview
Restless Legs Syndrome (RLS), also known as Willis-Ekbom disease, is a chronic, lifelong sensory-motor neurological disorder characterized by an irresistible urge to move the legs, typically accompanied by unpleasant sensations, worsening at rest and in the evening. It is one of the most common movement disorders, with an overall adult prevalence of ~7.2% (moderate-to-severe: ~2.7%), higher in North American and European populations and greater in women than in men.
Diagnostic Criteria (IRLSSG 2014)
All 5 essential criteria must be present for diagnosis - purely clinical, no tests required:
| # | Essential Criterion |
|---|---|
| 1 | An urge to move the legs, usually accompanied by or caused by unpleasant or uncomfortable sensations |
| 2 | Symptoms begin or worsen during rest or inactivity (lying, sitting) |
| 3 | Symptoms are partially or totally relieved by movement (walking, stretching) - at least while the activity continues |
| 4 | Symptoms are worse in the evening or night than during the day (circadian pattern; peaks midnight-4 AM) |
| 5 | Symptoms are not solely accounted for by another medical/behavioral condition |
Supportive (Non-Essential) Features
- Positive family history (3-5x higher prevalence in first-degree relatives)
- Response to dopaminergic therapy
- Periodic limb movements during sleep (PLMS) - present in ~80-90% of patients
- Sleep disturbance (sleep-onset insomnia, daytime sleepiness)
- Normal examination in the primary/idiopathic form
Note: DSM-5 additionally requires frequency ≥3 times/week and duration ≥3 months. AASM requires a clinical significance specifier.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Bradley and Daroff's Neurology in Clinical Practice
Sensory Descriptions
Patients describe the sensations as:
- Creeping, crawling, tingling
- Burning, aching, cramping
- Itching, "internal itch"
- Knife-like, heaviness, tension
- "Worms under the skin," coldness
Typically located between the knee and ankle (distinguishing from acral paresthesias). In advanced stages, symptoms may spread to the arms or, rarely, the abdomen (relieved by dopamine agonists).
"Patients may report that the discomfort can be torturously debilitating and cause them to walk or continuously move their legs until the early morning hours." - Goldman-Cecil Medicine
Pathophysiology
Central Iron-Dopamine Hypothesis
The dominant mechanistic model:
- Iron deficiency in the CNS (even with normal serum hemoglobin/hematocrit) → reduced activity of tyrosine hydroxylase (iron is a cofactor) → decreased dopamine synthesis
- Reduced dopaminergic modulation of spinal cord excitability → sensory overactivity and motor restlessness
- PET/SPECT studies show reduced dopamine receptor and transporter binding in the basal ganglia
- Serum ferritin is often low in RLS patients, even when other iron indices are normal - the most clinically useful screening test
Genetics
RLS is frequently inherited in an autosomal dominant fashion (in primary/idiopathic form). Key loci:
-
MEIS1, BTBD9, MAP2K5/LBXCOR1, PTPRD, PCDHA3
-
Loci on chromosomes 2p14, 16q12.1, 12q, 14q, 9p, 2q, 20p
-
~40-50% prevalence in first-degree relatives of idiopathic cases; 83% concordance in monozygotic twins
-
Goldman-Cecil Medicine; Bradley and Daroff's Neurology
Secondary Causes
| Category | Specific Causes |
|---|---|
| Metabolic | Iron-deficiency anemia, low ferritin |
| Renal | Uremia, dialysis-dependent CKD (prevalence ~68% in renal failure); resolves after kidney transplantation |
| Pregnancy | Especially third trimester |
| Neurological | Peripheral neuropathy (especially uremic), Parkinson disease |
| Drugs | Antidepressants (especially SSRIs, TCAs), antihistamines, antipsychotics, alcohol before sleep |
| Other | Thyroid disease, folate deficiency |
Associated Condition: Periodic Limb Movements of Sleep (PLMS)
- Present in ~80-90% of RLS patients (but only a minority of PLMS patients have RLS)
- Repetitive movements every 20-90 seconds for minutes to an hour
- Primarily involve the tibialis anterior - dorsiflexion of foot and big toe, sometimes triple flexion of hip and knee (similar to Babinski response)
- Duration 1-2 seconds (slower than myoclonus)
- Causes microarousals or full arousals; patient is usually unaware - told by bed partner or suspects from disarray of bedclothes
- Diagnosis requires polysomnography (unlike RLS which is diagnosed clinically)
Investigation
- Serum ferritin - the only recommended routine test; check for iron deficiency
- Treat if ferritin < 75 µg/L (some guidelines use lower cutoffs)
- Serum iron, TIBC, CBC - assess iron stores and anemia
- Polysomnography - if PLMS suspected, sleep apnea co-exists, or diagnosis is uncertain
- Renal function (creatinine, eGFR) - rule out uremia
- Thyroid function tests if clinically indicated
- No neuroimaging required for typical primary RLS
Management
Step 1: Treat Secondary Causes First
- Iron replacement if ferritin < 75 µg/L: Ferrous sulfate 325 mg BID-TID (note GI side effects)
- Ferrous sulfate + vitamin C enhances absorption
- Correct uremia, discontinue offending drugs, treat underlying neuropathy
Step 2: Non-Pharmacological Measures
- Good sleep hygiene
- Avoid caffeine, alcohol, sleep deprivation
- Regular moderate exercise; leg stretching
- Hot baths or massage before bed
- Early mobilization post-surgery (best strategy in post-op patients)
- Mental engagement (video games, puzzles) while sedentary
Step 3: Pharmacological Treatment
Based on international IRLSSG/EURLSSG guidelines and the 2025 AASM Clinical Practice Guideline (PMID: 39324694):
Current First-Line: Alpha-2-Delta (α₂δ) Ligands
Current guidelines have shifted preference toward α₂δ ligands over dopamine agonists for first-line therapy due to lower risk of augmentation:
| Drug | Dose | Notes |
|---|---|---|
| Gabapentin enacarbil (prodrug) | 600-1200 mg/day | FDA-approved for RLS; preferred over gabapentin (more consistent absorption) |
| Pregabalin | 25-300 mg/day | Comparable efficacy to pramipexole 0.25 mg; lower augmentation than pramipexole 0.5 mg; monitor for suicidal ideation |
| Gabapentin | 300-2700 mg/day | Useful especially with comorbid pain or insomnia; variable absorption |
Dopamine Agonists (Use Cautiously - Augmentation Risk)
If used, keep dopaminergic load as low as possible and screen regularly for augmentation:
| Drug | Dose | Notes |
|---|---|---|
| Pramipexole | 0.125-0.5 mg, 1.5-2h before bedtime | FDA-approved; risk of augmentation, impulse control disorders |
| Ropinirole | 0.25-2 mg, 1.5-2h before bedtime | FDA-approved |
| Rotigotine patch | 1-3 mg/24h transdermally | Useful for augmentation (longer-acting); also for daytime symptoms |
Augmentation: A paradoxical worsening where symptoms appear earlier in the day, spread to other body parts, and intensify - the major limitation of dopaminergic therapy. Risk is higher with levodopa > dopamine agonists. If augmentation occurs, carefully withdraw the dopaminergic agent and switch to α₂δ ligand.
Levodopa (Not for Chronic Use)
- Levodopa/carbidopa 25/100 mg, ½-3 tabs 30 min before bedtime
- Effective short-term; significant augmentation risk with chronic use
- Best reserved for intermittent, "on-demand" use
Second/Third-Line Agents
| Drug | Dose | Indication |
|---|---|---|
| Clonazepam | 0.125-0.5 mg at bedtime | Adjunct; caution in sleep apnea |
| Clonidine | 0.1 mg BID | Useful if hypertensive comorbidity |
| Opioids (oxycodone, codeine, methadone) | Variable | Refractory RLS; addiction potential |
| Oxycodone-naloxone | 40/20 mg BID | Effective; reduces opioid abuse potential |
| Baclofen, carbamazepine | Variable | Occasionally helpful |
Medication Selection Guide (IRLSSG-Adapted)
| Clinical Situation | Preferred Drug |
|---|---|
| Comorbid insomnia | α₂δ ligand |
| Comorbid pain/neuropathy | α₂δ ligand |
| Impulse control disorder history | α₂δ ligand |
| Generalized anxiety disorder | α₂δ ligand |
| Very severe RLS | Dopamine agonist |
| Daytime symptoms | Long-acting agent or BID dosing |
| Pregnancy | Avoid DA and α₂δ ligands; use iron |
| Renal impairment | Avoid renally excreted drugs (pramipexole, α₂δ); adjust doses |
| PLMS-predominant | Dopamine agonist |
Intravenous Iron
- IV iron (e.g., ferric carboxymaltose, low-molecular-weight iron dextran) can be highly effective especially if oral iron is not tolerated or ferritin remains low
- Effective even in patients without frank iron-deficiency anemia
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Akathisia (drug-induced) | No sensory component; related to antipsychotic use |
| Peripheral neuropathy | Acral distribution; no circadian pattern |
| Nocturnal leg cramps | Painful muscle cramps, visible; brief; no urge to move |
| Positional discomfort | Relieved by changing position, not movement per se |
| Venous insufficiency | Edema, varicosities; relieved by elevation |
| Peripheral arterial disease | Intermittent claudication; relieved by rest |
| PLMS without RLS | No subjective sensory discomfort or urge to move |
Recent Evidence (2025 AASM Guidelines)
The 2025 AASM systematic review and clinical practice guideline (PMID: 39324694; PMID: 39324664) updated treatment recommendations using GRADE methodology. Key shifts include:
- Dopamine agonists are no longer unconditionally first-line - α₂δ ligands are now preferred in many clinical scenarios given augmentation risk
- Strong evidence supports gabapentin enacarbil and pregabalin
- IV iron is increasingly recognized as an effective disease-modifying intervention
- A 2024 systematic review (PMID: 39064758) assessed dietary supplementation (especially iron, magnesium, vitamin D) with modest supportive evidence
Sources: Adams and Victor's Principles of Neurology 12e | Bradley and Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Miller's Anesthesia 10e | Stahl's Essential Psychopharmacology | 2025 AASM Practice Guideline (PMID: 39324694)
This is a shared conversation. Sign in to Orris to start your own chat.