Femur
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete anatomy review of the femur, drawn from authoritative orthopaedic and anatomy textbooks.
The Femur
The femur is the longest and strongest bone in the human body. It forms the skeleton of the thigh, articulating proximally with the acetabulum of the pelvis (hip joint) and distally with the tibia and patella (knee joint).
Gross Anatomy
The femur is divided into proximal, shaft, and distal parts.
Proximal Femur
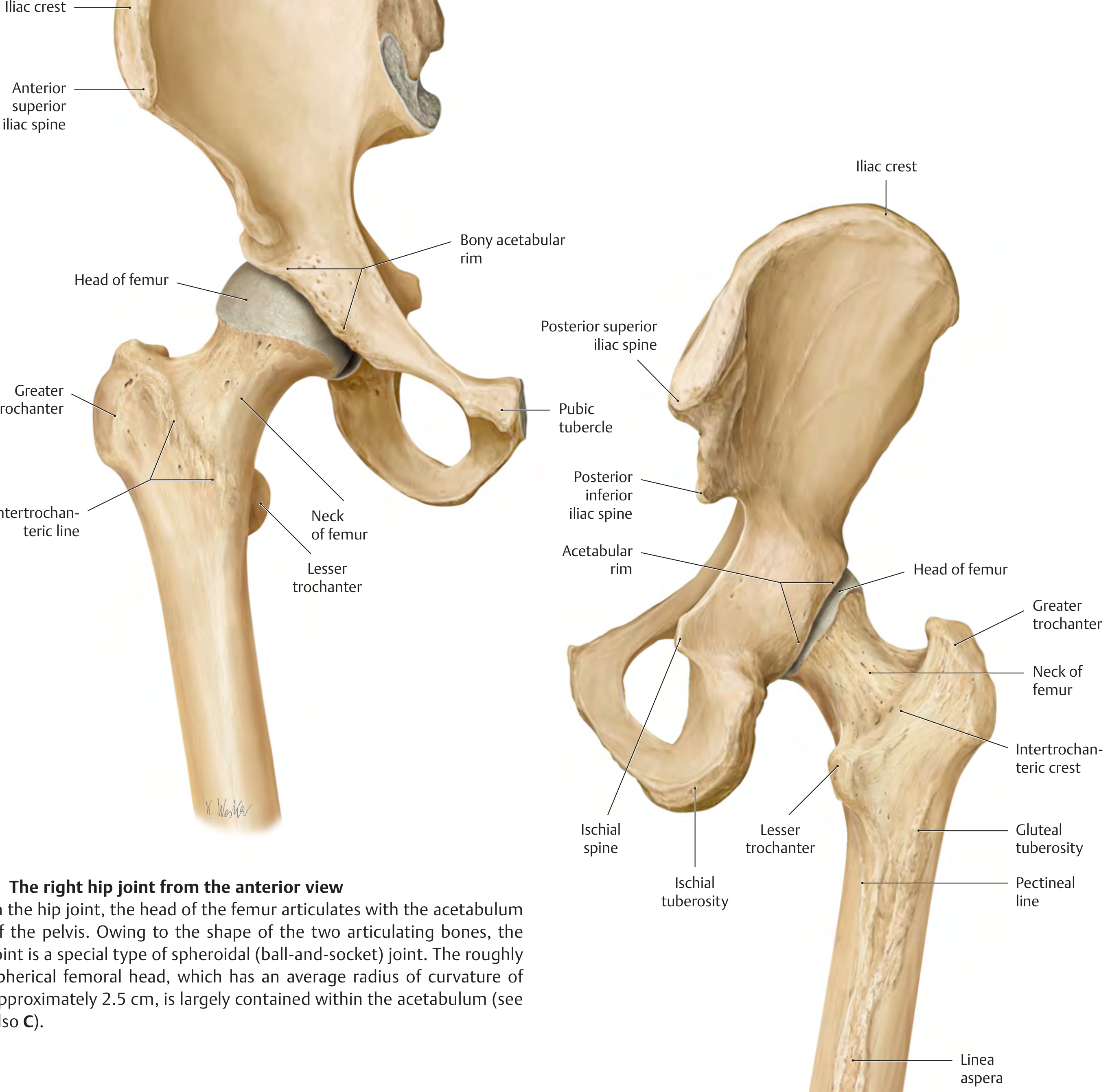
The right hip joint: anterior (left) and posterior (right) views, showing the head, neck, trochanters, and posterior surface of the proximal femur. - THIEME Atlas of General Anatomy
Head of femur
- Roughly spherical (~2.5 cm radius of curvature)
- Largely covered by hyaline articular cartilage except at the fovea capitis (a pit on the medial surface for attachment of the ligamentum teres / ligament of the head)
- Articulates with the acetabulum to form a ball-and-socket (spheroidal) joint
Neck of femur
- Connects the head to the shaft
- Neck-shaft angle averages 127° in adults (begins at ~141° in the fetus; decreases with age)
- Femoral neck is anteverted approximately 14° relative to the femoral condyles (range 1-40°)
- Largely intracapsular; the posterior neck is only partially covered by the joint capsule (basicervical and intertrochanteric regions are extracapsular)
Trochanters
| Feature | Greater Trochanter | Lesser Trochanter |
|---|---|---|
| Position | Lateral, proximal | Medial, posteromedial |
| Muscle attachments | Gluteus medius & minimus, obturators, piriformis, gemelli | Iliopsoas |
| Connecting ridge | Intertrochanteric line (anterior) | Intertrochanteric crest (posterior) |
The gluteal tuberosity is a roughened area on the posterior proximal shaft lateral to the lesser trochanter where gluteus maximus inserts.
Shaft (Diaphysis)
- Cylindrical; directed obliquely downward and medially, so the knee lies near the body's midline
- The posterior surface bears a prominent longitudinal ridge, the linea aspera, which serves as attachment for adductor and other thigh muscles
- The linea aspera splits distally into the medial and lateral supracondylar lines, which form the floor and sides of the popliteal fossa
- The pectineal line runs from the lesser trochanter to the linea aspera (adductor longus and brevis, pectineus insert here)
Distal Femur
- Expands into two large articular masses: the medial condyle (larger) and lateral condyle (smaller)
- The condyles articulate with the tibial plateaus and with the patella (via the patellar/trochlear surface anteriorly)
- Between the condyles posteriorly lies the intercondylar (intercondyloid) fossa:
- Lateral wall = attachment of the anterior cruciate ligament (ACL)
- Medial wall = attachment of the posterior cruciate ligament (PCL)
- The roof is demarcated by the intercondylar line
- Non-articular bony prominences above the condyles = medial and lateral epicondyles (attachment sites of collateral ligaments and muscles)
- The adductor tubercle sits above the medial epicondyle; it is the termination of the medial supracondylar line and receives the adductor magnus tendon
Blood Supply
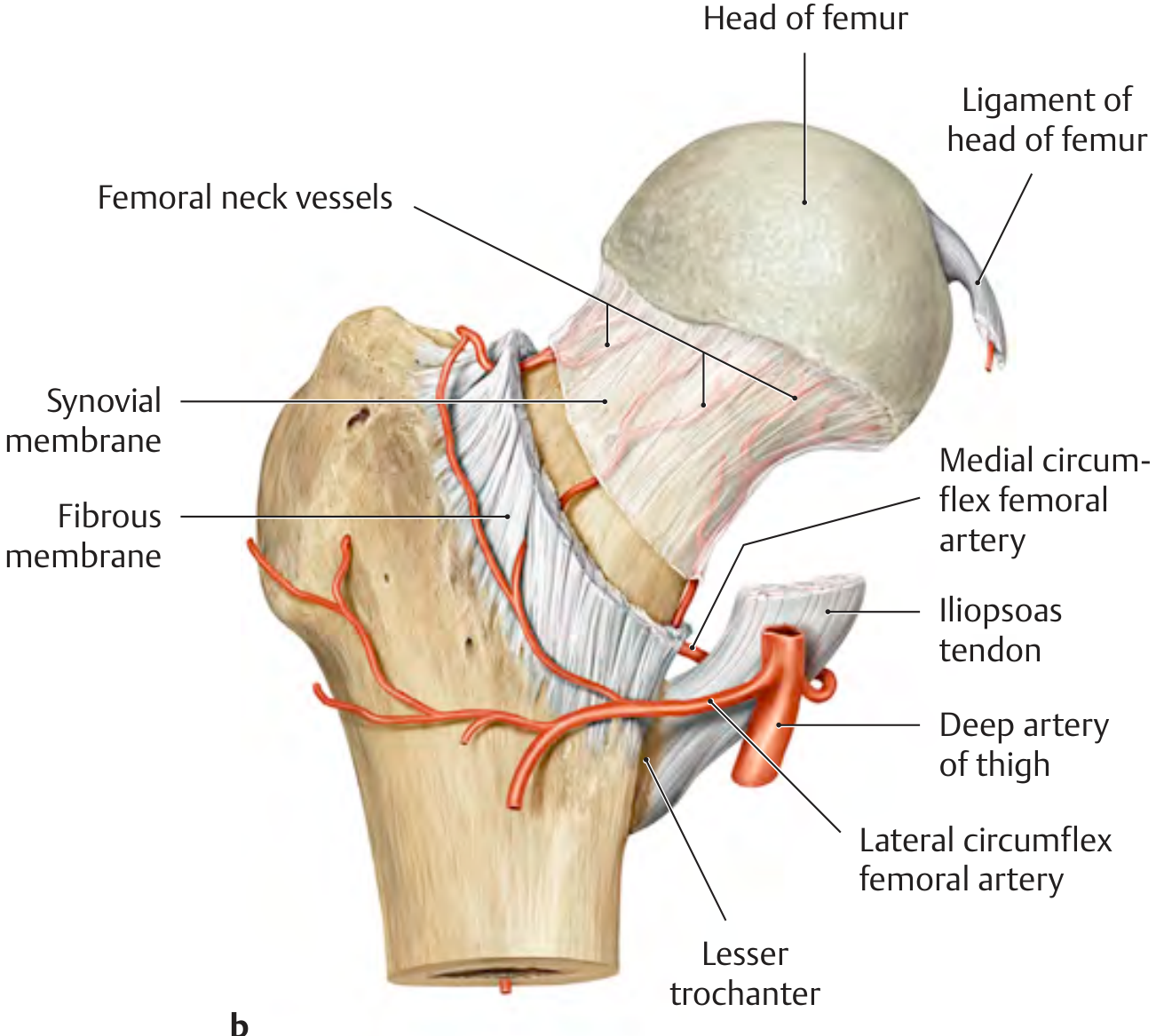
Course of femoral neck vessels and blood supply to the femoral head via medial and lateral circumflex femoral arteries. - THIEME Atlas of General Anatomy
The femoral head's blood supply is tenuous and clinically important:
- Medial circumflex femoral artery (MFCA) - the dominant supply; a branch of the profunda femoris (deep artery of thigh). It runs posteriorly around the neck and its deep branch penetrates retinacular vessels under the joint capsule to supply the femoral head
- Lateral circumflex femoral artery (LCFA) - contributes mainly to the anterior neck via ascending branch
- Artery of the ligamentum teres - a branch of the obturator artery; relatively minor in adults but contributes to the foveal area
Clinical point: Femoral neck fractures and hip dislocations can rupture the MFCA retinacular vessels, interrupting the main blood supply and causing avascular necrosis (AVN) of the femoral head. In children, the piriformis fossa nail entry point for intramedullary nailing risks damage to the posterosuperior retinacular vessels off the MFCA - this is why lateral trochanteric entry is preferred.
Ossification
| Epiphysis | Appearance | Fusion |
|---|---|---|
| Distal femoral epiphysis | Present at birth (important in forensic/gestational age assessment) | ~19 years |
| Femoral head epiphysis | ~11 months (one large physis including both trochanters) | ~18 years |
- The distal femur is responsible for the highest percentage of longitudinal growth in the lower extremity (~70% of femoral length; ~37% of total lower limb length)
- Slipped capital femoral epiphysis (SCFE) occurs through the femoral head physis at the zone of hypertrophy
Key Angles and Measurements
| Parameter | Normal Value |
|---|---|
| Neck-shaft angle | ~127° (coxa vara < 120°, coxa valga > 135°) |
| Anteversion of femoral neck | ~14° (range 1-40°) relative to condyles |
| Acetabular transverse angle | ~40° in adults (51° at birth) |
| Femoral head radius | ~2.5 cm |
Proximal Femoral Trabecular Architecture
The proximal femur has two main trabecular systems that resist loading:
- Compression trabeculae - arching from calcar to superolateral femoral head cortex
- Tension trabeculae - from the lateral cortex, arching medially toward the femoral head
- The Ward triangle is a relatively weak area between the two systems where trabecular density is low - a common site for stress fractures and osteoporotic fractures
Muscle Attachments Summary
| Region | Muscles Attaching |
|---|---|
| Greater trochanter | Gluteus medius, gluteus minimus, piriformis, obturator internus & externus, gemelli |
| Lesser trochanter | Iliopsoas |
| Gluteal tuberosity | Gluteus maximus |
| Linea aspera | Adductors (longus, brevis, magnus), vastus lateralis, vastus medialis, short head of biceps femoris |
| Adductor tubercle | Adductor magnus (lower/hamstring part) |
| Lateral epicondyle | Lateral collateral ligament, popliteus, gastrocnemius (lateral head) |
| Medial epicondyle | Medial collateral ligament, gastrocnemius (medial head) |
Clinical Correlations
- Femoral neck fractures: Commonest in elderly osteoporotic women (minimal trauma); risk of AVN and non-union due to tenuous blood supply. Classification: subcapital, transcervical, basicervical
- Intertrochanteric fractures: More vascular region, lower AVN risk; treated with intramedullary nail or dynamic hip screw
- Subtrochanteric fractures: High biomechanical stress; treated with intramedullary nail
- Femoral shaft fractures: High energy in young (MVA), lower energy in elderly; intramedullary nail is gold standard treatment
- Distal femur fractures: Up to 6% of all femur fractures; bimodal distribution (high energy in young, low energy in elderly); thin cortices and wide medullary canal make fixation challenging
Sources: THIEME Atlas of General Anatomy and Musculoskeletal System; Imaging Anatomy Vol. 3 Bones, Joints, Vessels and Nerves; Miller's Review of Orthopaedics 9th Ed; Rockwood and Green's Fractures in Adults 10th Ed 2025; Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.