TAP block
Reading File
Finding Sources
Searching PubMed
"transversus abdominis plane" block analgesia
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Transversus Abdominis Plane (TAP) Block
Anatomy
The TAP block is a fascial plane block targeting the somatic nerves of the anterolateral abdominal wall. Four thoracoabdominal peripheral nerves pass through this plane:
- Subcostal nerve (T12)
- Iliohypogastric nerve (L1)
- Ilioinguinal nerve (L1)
- Genitofemoral nerve (partial contribution for lower abdomen)
These nerves travel in the fascial layer between the transversus abdominis (TA) and internal oblique (IO) muscles - this is the injection target.
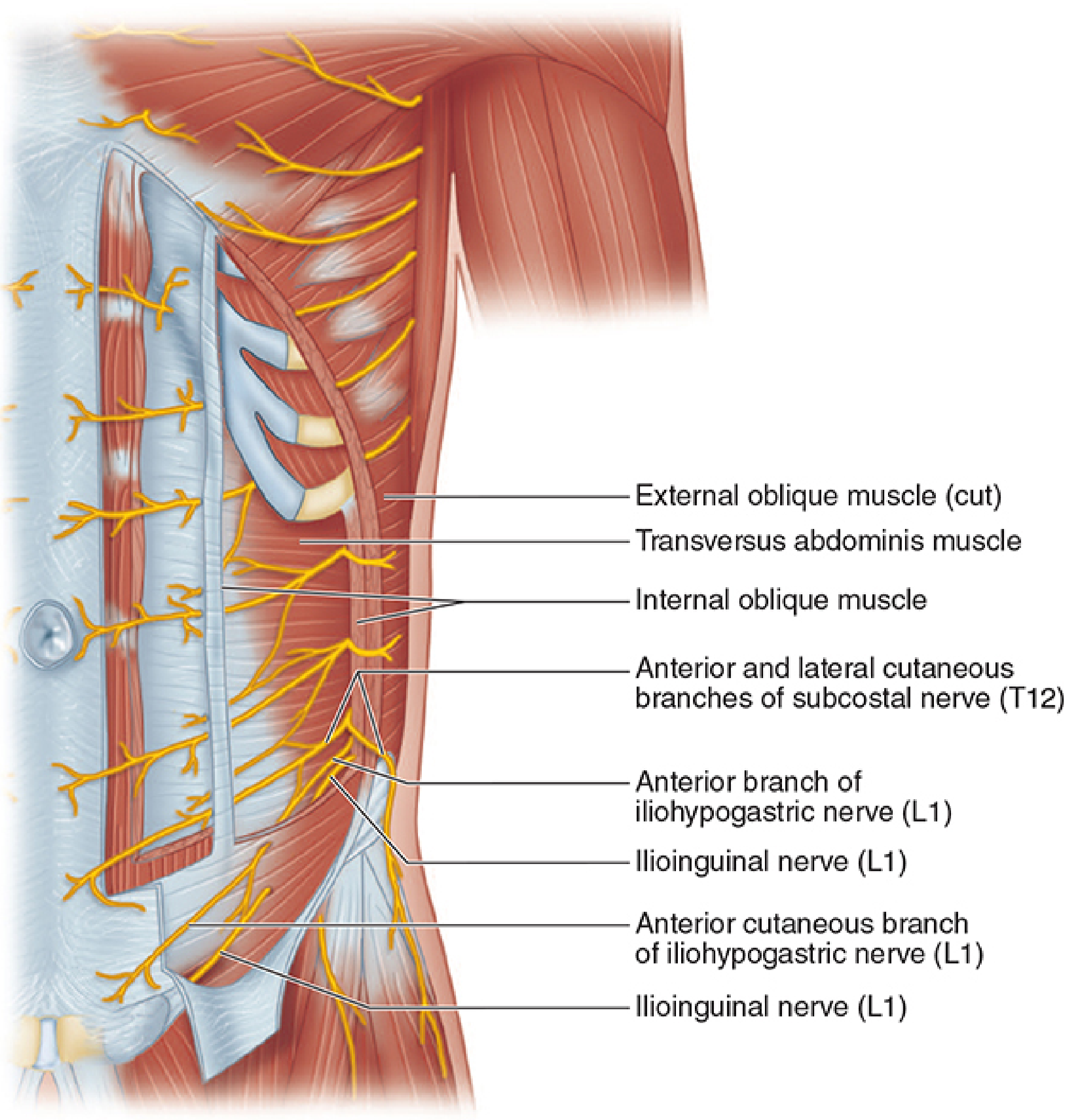
Figure: Lateral abdominal wall anatomy showing the external oblique (cut), internal oblique, and transversus abdominis muscles, with the subcostal (T12), iliohypogastric, and ilioinguinal nerves (L1) coursing in the TAP plane. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Key Concept: Somatic-Only Block
The TAP block provides somatic analgesia only - it has no visceral analgesic benefit. This means:
- Effective for skin, fascia, and muscle pain from incisions
- Does not cover peritoneal traction pain (e.g., during inguinal hernia repair, supplementation is often needed)
Indications
- Postoperative analgesia for procedures below the umbilicus: appendectomy, cesarean section, inguinal hernia repair, laparoscopic abdominal surgery
- The subcostal approach extends coverage to the upper abdomen (T6-T9)
- Part of enhanced recovery after surgery (ERAS) multimodal analgesia protocols
Ultrasound-Guided Technique
Patient position: Supine (lateral decubitus ideal but not always feasible)
Transducer placement: Linear array (curvilinear for obese patients) placed between the iliac crest and the costal margin in the midaxillary line, parallel to the inguinal ligament, just superior to the ASIS.
Sonoanatomy ("three-layer cake"):
- External oblique (EO) - most superficial
- Internal oblique (IO) - middle
- Transversus abdominis (TA) - deepest
The muscles appear as striated hypoechoic structures with hyperechoic fascial borders between them.
Needle approach: In-plane from the anterior side, directed toward the posterolateral corner of the TA muscle. The needle tip is advanced to the hyperechoic effacement of the deep border of IO / superficial border of TA.
Injection: 15-30 mL of dilute local anesthetic is deposited in the fascial layer. Correct placement is confirmed by:
- Visualization of the fascial layer expanding (elliptical fluid spread)
- The "kayak sign" - the fascia between IO and TA splits apart in a kayak shape
- Posterior movement of the TA muscle
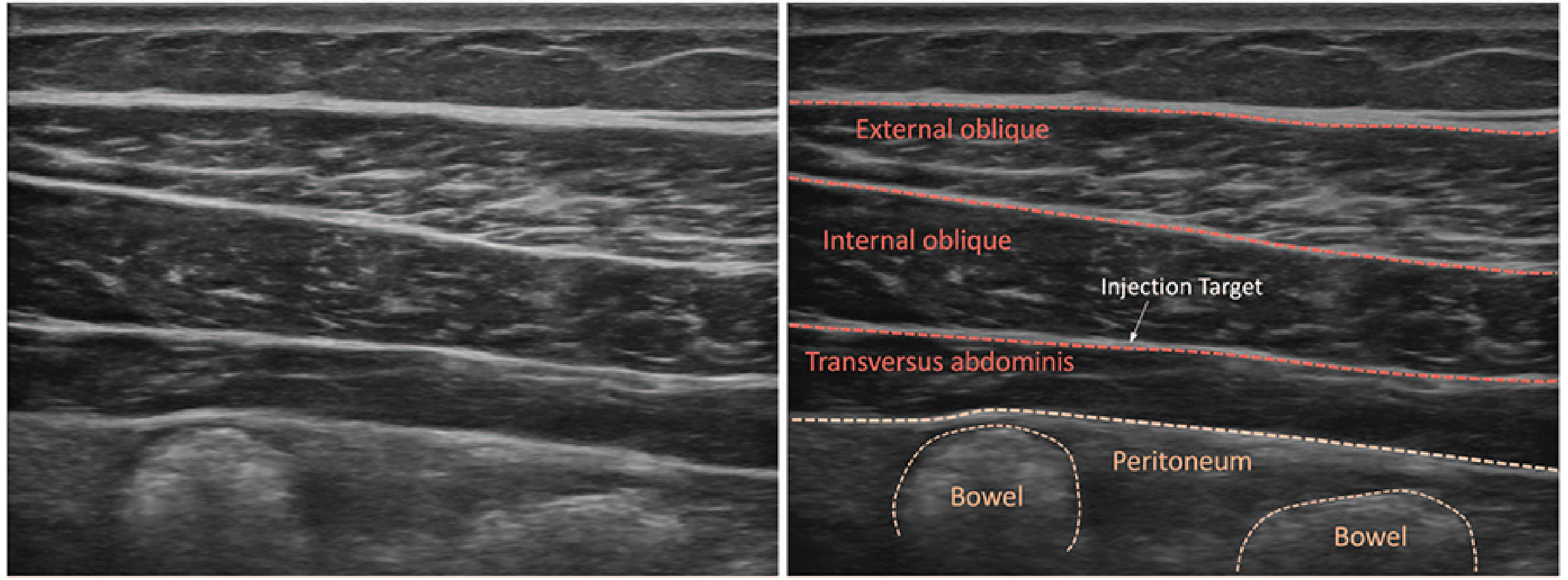
Figure: Ultrasound view of the lateral abdominal wall with labeled layers. The injection target (white arrow) lies between the internal oblique and transversus abdominis. - Morgan & Mikhail's Clinical Anesthesiology, 7e
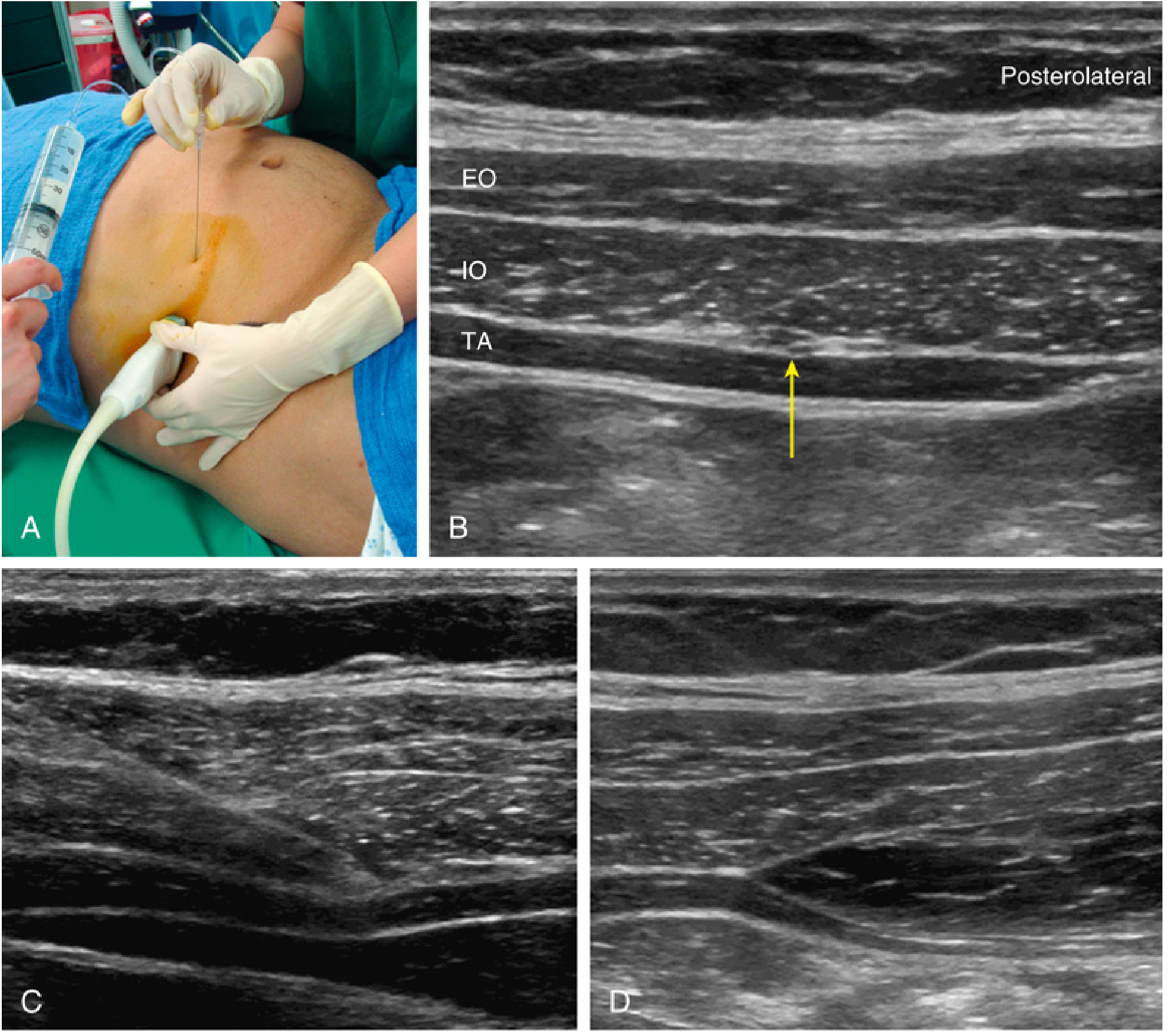
Figure: TAP block with ultrasound guidance. (A) Probe on midaxillary line. (B) Three-layer appearance with nerves entering IO-TA plane (yellow arrow). (C) In-plane needle approach. (D) Kayak sign confirming successful injection. - Miller's Anesthesia, 10e
Approaches
| Approach | Probe Placement | Coverage |
|---|---|---|
| Lateral (midaxillary) | Between iliac crest and costal margin | Lower abdominal wall, T10-L1 |
| Subcostal | Below costal margin at midclavicular line | Upper abdomen, T6-T9 |
| Posterior | At lumbar triangle of Petit | Extended spread, some visceral coverage via QL |
Blind/Landmark Technique (Historical)
The lumbar triangle of Petit (bounded by the iliac crest, latissimus dorsi, and external oblique) can be used as a landmark. Two "pops" indicate correct positioning:
- First pop: penetration of external oblique fascia
- Second pop: penetration of internal oblique fascia
Ultrasound guidance is now strongly preferred and recommended, particularly in children and to avoid peritoneal puncture.
Local Anesthetic Choice
- Typically 0.25-0.5% bupivacaine or ropivacaine (0.2-0.375%)
- Volume: 15-30 mL per side (bilateral for midline incisions)
- Direct visualization is not required if 15-20 mL of dilute LA is deposited in the correct fascial plane
Complications
- Peritoneal perforation with or without bowel injury (main risk - the TA is thin; deep injection penetrates peritoneum)
- Local anesthetic systemic toxicity (LAST) - particularly relevant with high volumes and bilateral injections due to the vascularity of the region
- Intra-abdominal visceral injury
Special Populations: Pediatrics
- Ultrasound guidance is mandatory in children
- Probe placed on the midclavicular line between iliac crest and last rib
- The ilioinguinal/iliohypogastric block provides better analgesia than TAP for inguinal hernia in children, likely due to inadequate blockade of the genitofemoral nerve with the TAP approach
- Pharmacokinetic studies confirm safety in neonates
Recent Evidence (2024-2025): Two recent systematic reviews/meta-analyses (PMID 39709396, PMID 40694119) compared laparoscopic-assisted vs. ultrasound-guided TAP blocks for laparoscopic abdominal surgeries. A PROSPECT systematic review (PMID 39129451) also addressed pain management after laparoscopic cholecystectomy, including TAP block recommendations.
Sources: Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Barash Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.