Microbiological stains and cultures used for fungal corneal ulcer
Reading File
Finding Sources
Finding Sources
Searching PubMed
fungal keratitis diagnosis stain culture microbiological
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-cited answer. Here it is:
Microbiological Stains and Cultures for Fungal Corneal Ulcer
Specimen Collection
Before any staining or culture, adequate material must be obtained. Using a sterile Kimura spatula, knife blade, or moistened calcium alginate swab (with non-preserved saline or thioglycolate broth), the ulcer base AND leading edge of the infiltrate are scraped firmly at the slit lamp. For fungal infection specifically, deep scrapings are essential - filamentous fungi tend to proliferate just anterior to Descemet's membrane. Specimens are placed on slides first, then culture media. The spatula is flamed and cooled between each inoculation.
Important: All samples must be collected BEFORE commencing antifungal therapy.
Microbiological Stains
Routine Stains
| Stain | What it detects | Notes |
|---|---|---|
| Gram stain | Bacteria AND fungi | ~50% sensitive for fungi; identifies fungal elements as Gram-positive |
| Calcofluor white | Fungi and Acanthamoeba | Fluorescent dye - binds chitin in fungal cell walls; highly sensitive; requires fluorescence microscope |
| KOH (10%) wet mount | Fungi, Nocardia, Acanthamoeba | Rapid - KOH dissolves keratin/cellular debris, leaving fungal hyphae/spores visible; can be combined with calcofluor white |
Optional / Supplementary Stains
| Stain | What it detects | Notes |
|---|---|---|
| Giemsa stain | Bacteria, fungi, Acanthamoeba | ~50% sensitive for fungi; also shows inflammatory cells |
| Gomori Methenamine Silver (GMS) | Fungi and Acanthamoeba | Stains fungal cell walls black against green background; high sensitivity |
| Periodic Acid-Schiff (PAS) | Fungi and Acanthamoeba | Stains fungal cell walls magenta/pink; useful on biopsy material |
| Hematoxylin & Eosin (H&E) | General morphology | Used mainly on biopsy/histopathology specimens |
| Acid-fast stain (ZN/Kinyoun) | Mycobacterium, Nocardia | Not fungal-specific; used if co-infection suspected |
Sensitivity summary: KOH preparation is considered the most rapid and can be highly sensitive. Gram and Giemsa are each approximately 50% sensitive for fungi. Calcofluor white requires fluorescence microscopy but is highly sensitive. GMS and PAS are most sensitive of all but are usually applied to biopsy material.
Culture Media
Routine Media
| Medium | Organisms | Conditions |
|---|---|---|
| Blood agar | Most bacteria AND fungi | Most fungi will grow here too; incubate at 25-30°C |
| Sabouraud Dextrose Agar (SDA) - without cycloheximide | Primary medium for fungi | Room temperature (25-30°C); cycloheximide must be omitted as it inhibits many pathogenic fungi like Aspergillus and Candida |
| Thioglycolate broth | Aerobic and anaerobic bacteria; enrichment for fungi | Liquid enrichment medium |
| Chocolate agar | Haemophilus, Neisseria gonorrhoeae | Place in CO2 jar |
Optional Media
| Medium | Organisms |
|---|---|
| Löwenstein-Jensen (L-J) medium | Mycobacteria, Nocardia (add if post-LASIK history or atypical appearance) |
| Non-nutrient agar with E. coli overlay | Acanthamoeba |
Key point on SDA: Sabouraud dextrose agar is the primary dedicated fungal medium. The formulation used must not contain cycloheximide (actidione), as this inhibitor - added to some SDA formulations to suppress environmental fungi - will also suppress many clinically important pathogens including Aspergillus, Candida, and Cryptococcus species. - Kanski's Clinical Ophthalmology, 10th ed.
Special Diagnostic Modalities
Corneal Biopsy
Indicated when:
- No clinical improvement after 3-4 days of empirical treatment
- No growth from scrapings after 1 week
- Deep stromal involvement (filamentous fungi proliferate just anterior to Descemet's membrane)
A 2-3 mm deep stromal block is excised and sent for both culture and histopathology (GMS/PAS staining).
PCR Analysis
- Rapid and highly sensitive (up to 90%)
- May be the current investigation of choice where available
- Note: calcium-containing swabs can inhibit polymerase activity - check local collection protocols before specimen collection
Anterior Chamber Tap
Advocated in resistant cases with endothelial exudate, as organisms may penetrate the endothelium.
In Vivo Confocal Microscopy (IVCM)
Permits real-time identification of fungal hyphae in vivo without scraping. Not widely available outside tertiary centers.
Contact Lens Cases
When fungal keratitis is associated with contact lens wear, the lens itself, lens case, and storage solution should all be sent for culture.
When to Biopsy vs. Scrape
| Situation | Action |
|---|---|
| Ulcer < 1 mm | Treat empirically; no scraping needed |
| Ulcer > 1-2 mm, visual axis, unresponsive | Culture + stains |
| No growth after 1 week, no improvement after 3-4 days | Corneal biopsy |
| Deep stromal infiltrate | Deep biopsy - filamentous fungi grow near Descemet's |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. - Investigations section, p. 233
- The Wills Eye Manual, 7th ed. - Appendix 8: Corneal Culture Procedure, p. 1119-1120 and Section 4.12 Fungal Keratitis, p. 210-211
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - Infectious Keratitis, p. 1496
Acanthemeba staining and culture
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough answer. Here it is:
Acanthamoeba Keratitis - Microbiological Stains and Cultures
Clinical Context (Key Points Before Investigation)
Acanthamoeba spp. are free-living protozoa found in soil, fresh/brackish water, and the upper respiratory tract. They exist in two forms:
- Trophozoite - active feeding form, pleomorphic, small nucleus with large central karyosome
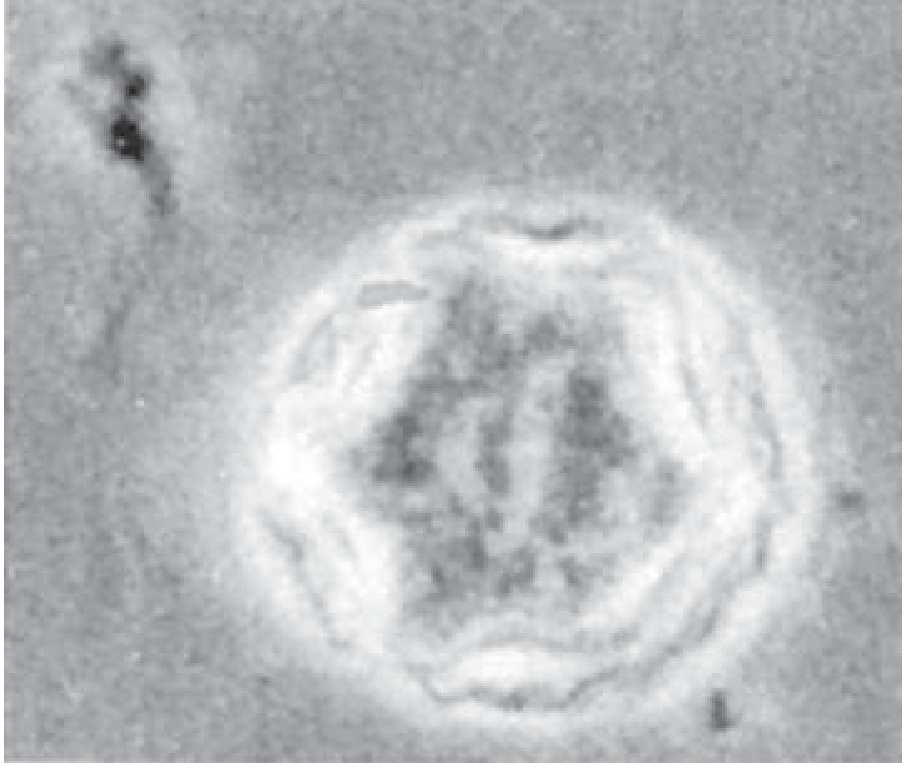
- Cyst - double-walled, highly resistant form with 1 nucleus and large karyosome; the form most commonly identified on staining
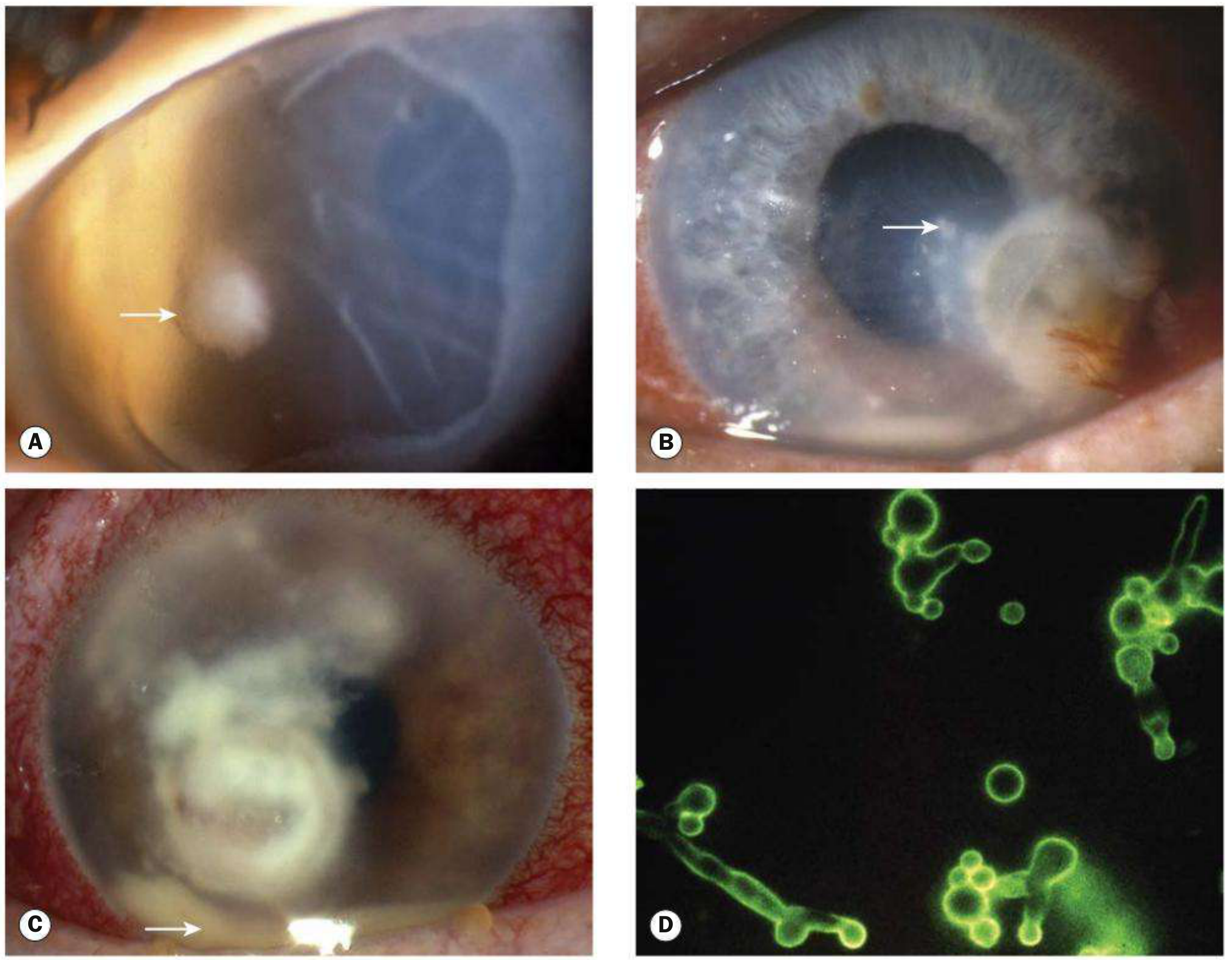
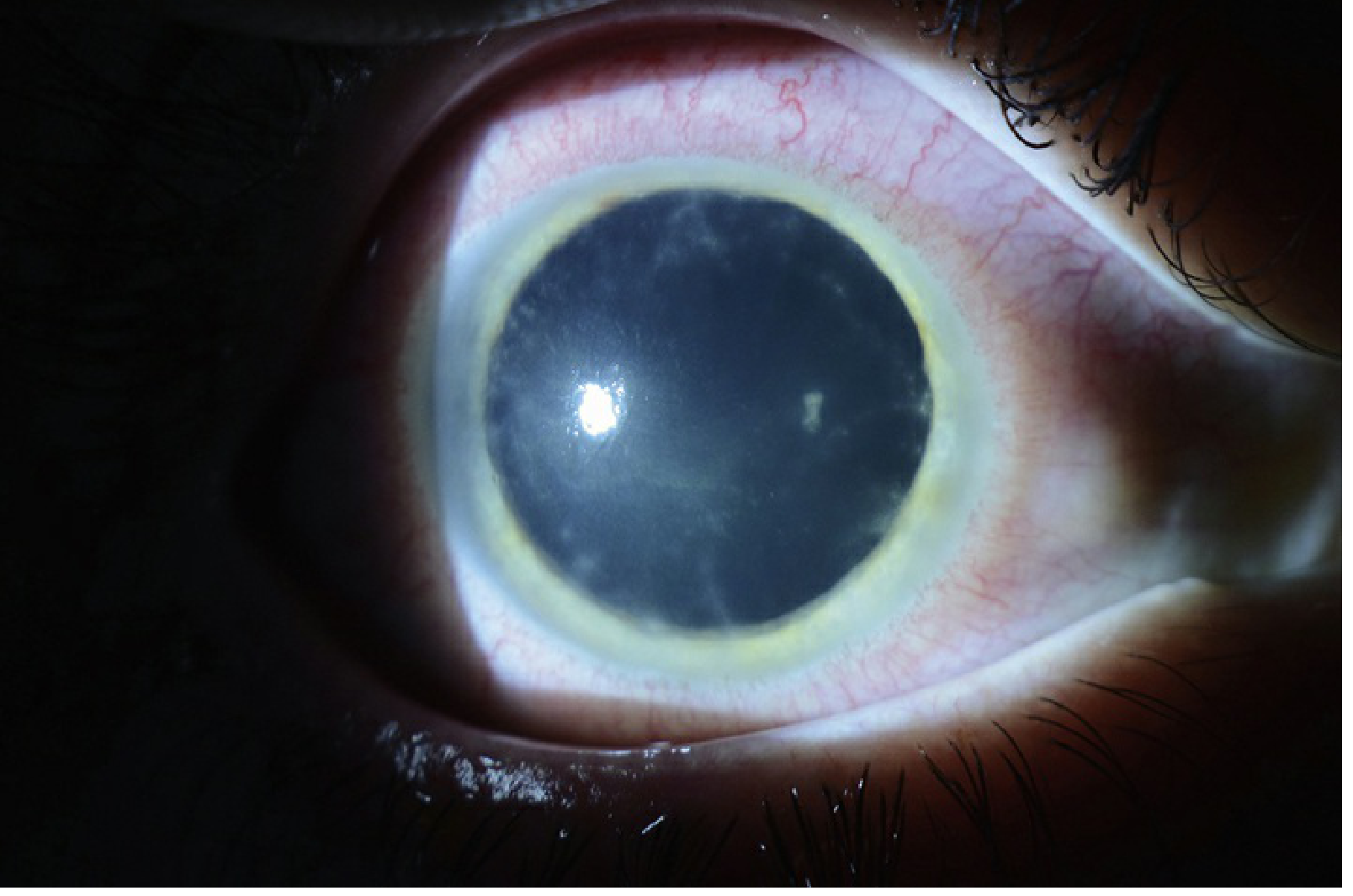
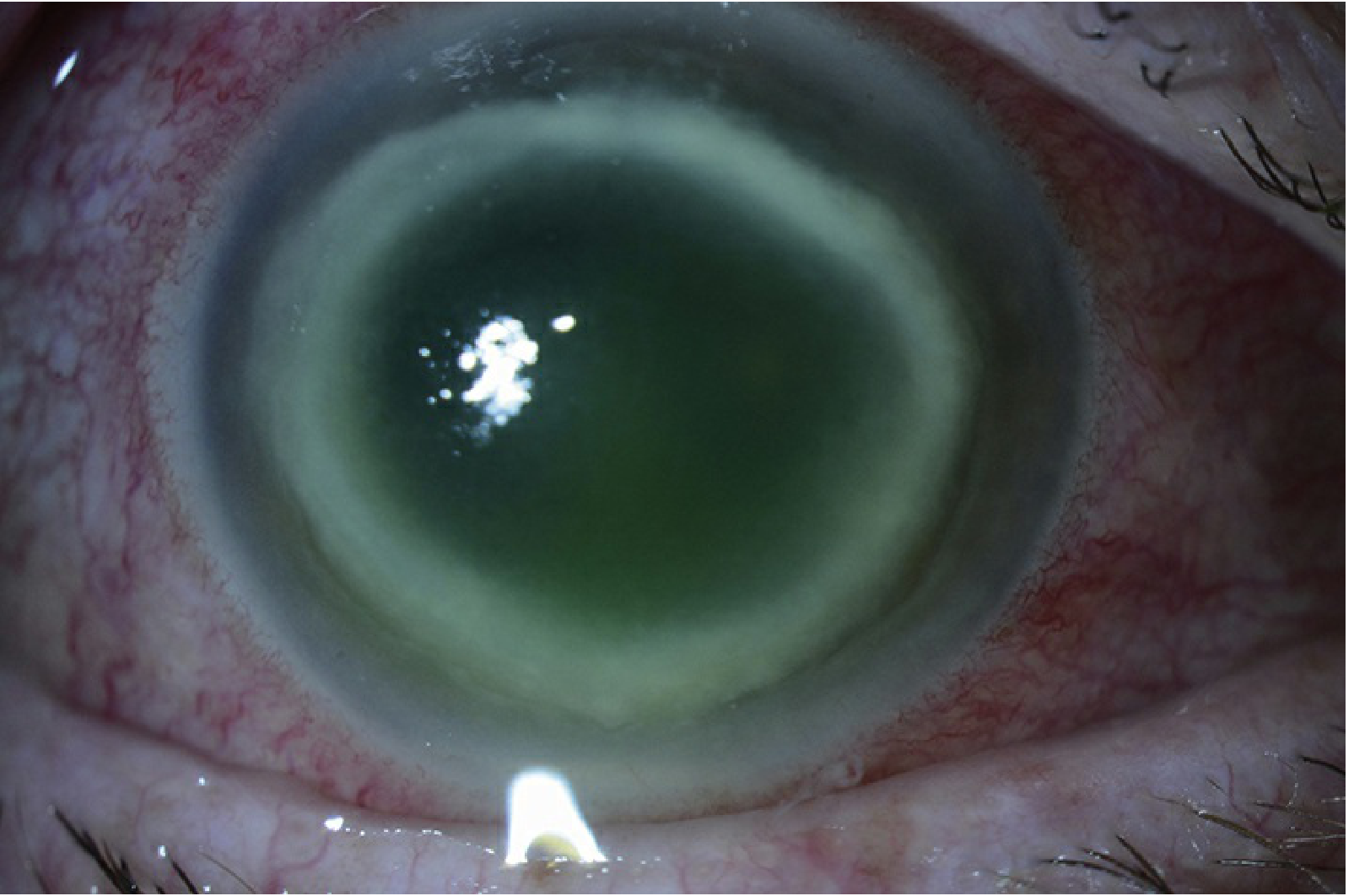
The condition is strongly associated with contact lens wear (especially using tap water to clean lenses), trauma, and water exposure. It is frequently misdiagnosed as HSV keratitis early in its course. The hallmark sign is radial keratoneuritis (perineural infiltrates), which is virtually pathognomonic.
Specimen Collection
Corneal scrapings are taken at the slit lamp using a sterile Kimura spatula or blade. Material is placed on slides first, then inoculated onto culture media. Contact lenses and lens cases should also be sent for culture.
Stains
Routine Stains
| Stain | Appearance of Acanthamoeba | Notes |
|---|---|---|
| Calcofluor White | Cysts fluoresce bright green/yellow-green | Most sensitive routine stain; fluorescent dye binds to the polysaccharide double wall of cysts; requires fluorescence microscope; also detects fungi |
| Periodic Acid-Schiff (PAS) | Cyst wall stains magenta/pink | Highlights polysaccharide-rich cyst wall; useful on both scrapings and biopsy material; may show typical cysts |
| Gram stain | May show cysts; variable sensitivity | Cysts may appear Gram-positive; less sensitive than calcofluor; also identifies co-infecting bacteria |
| Giemsa stain | May demonstrate cysts | Useful supplementary stain; also shows inflammatory cells and intracellular details |
Optional / Confirmatory Stains
| Stain | Use |
|---|---|
| Gomori Methenamine Silver (GMS) | Stains cyst walls black; useful on biopsy material |
| Haematoxylin & Eosin (H&E) | Used on biopsy specimens to identify cysts and trophozoites in tissue |
| KOH wet mount | Can reveal cysts, though less specific than calcofluor |
| Fluorescein-labeled antiserum (immunofluorescence) | Available from the CDC; highly specific; used on biopsy specimens |
What to look for: The irregular, polygonal double-walled cysts of Acanthamoeba are the key finding on staining. On confocal microscopy they appear as pear-shaped cysts measuring 11-15 μm.
Culture
Primary Culture Medium
| Medium | Details |
|---|---|
| Non-nutrient agar (NNA) with dead E. coli overlay | Definitive culture medium - Acanthamoeba trophozoites feed on the E. coli by phagocytosis and leave characteristic tracks/trails across the agar surface; incubate at 30-35°C |
How it works: The non-nutrient agar provides no growth factors itself. The dead (heat-killed or UV-killed) E. coli bacteria seeded onto the surface serve as the sole food source. As trophozoites phagocytose the bacteria, they leave clear trails visible to the naked eye and light microscopy. Absence of growth on blood agar or other standard media strongly supports Acanthamoeba when combined with positive NNA culture.
Other Culture Options
| Medium | Relevance |
|---|---|
| Blood agar | Included in the routine panel; Acanthamoeba usually will NOT grow here, so it serves as the negative control that distinguishes it from bacteria |
| Thioglycolate broth | Routine enrichment for bacteria; negative result supports amoebic etiology |
From Wills Eye Manual, Appendix 8: Non-nutrient agar with E. coli overlay is listed as an optional culture medium in the standard corneal culture procedure, to be added specifically when Acanthamoeba is suspected.
Advanced / Supplementary Investigations
| Method | Details |
|---|---|
| PCR (Real-time PCR) | Highly sensitive and specific; can detect Acanthamoeba, Naegleria, and Balamuthia simultaneously; available from the CDC and many reference labs; rapidly becoming the investigation of choice |
| In vivo Confocal Microscopy (IVCM) | Non-invasive; can identify double-walled cysts and trophozoites in real-time without scraping; cysts appear as pear-shaped structures 11-15 μm; not widely available outside tertiary centres |
| Corneal Biopsy | Indicated when scrapings are negative and clinical suspicion remains high; full-thickness specimen submitted for histopathology (PAS/GMS/H&E) AND culture on NNA with E. coli; filamentous forms (trophozoites) tend to be found in deeper stroma |
| Immunohistochemistry | Fluorescein-labeled antiserum for detection of protozoa in biopsy specimens; available from CDC |
Summary Table
| Investigation Type | Method | What it Detects |
|---|---|---|
| Stain (routine) | Calcofluor white | Cyst double-wall (fluorescent) |
| Stain (routine) | PAS | Cyst double-wall (magenta) |
| Stain (supplementary) | Gram | Cysts (variable) |
| Stain (supplementary) | Giemsa | Cysts and trophozoites |
| Stain (confirmatory) | GMS, H&E | Tissue biopsy |
| Culture (primary) | Non-nutrient agar + dead E. coli | Trophozoites (feeding trails) |
| Molecular | Real-time PCR | Acanthamoeba DNA |
| Imaging | In vivo confocal microscopy | Cysts and trophozoites in situ |
| Serology | Immunofluorescence (CDC) | Trophozoites and cysts in tissue |
Important note: Bacterial cultures are negative in uncomplicated Acanthamoeba keratitis (unless superinfection is present). Failure to respond to antibacterial or antiviral therapy in a contact lens wearer should always raise suspicion for Acanthamoeba.
Sources:
- Wills Eye Manual, 7th ed. - Section 4.13 Acanthamoeba Keratitis, p. 214-217; Appendix 8, p. 1119-1120
- Kanski's Clinical Ophthalmology, 10th ed. - Acanthamoeba section, p. 249
- Harrison's Principles of Internal Medicine, 22nd ed. - Chapter 230, Acanthamoeba Infections, p. 1802
- Quick Compendium of Clinical Pathology, 5th ed. - Section 3.3.2.3.2
- Goldman-Cecil Medicine - Acanthamoeba Keratitis section
This is a shared conversation. Sign in to Orris to start your own chat.