So now I'm starting CVS revision from first aid and then I'll solve all the questions from jumbled. So before I begin, I want to understand like in a few topics because that's important how the murmurs and all other things are tested, right? The Valsalva maneuver, explain me what exactly is happening, what is this straining, like sitting, standing positions can change the murmurs and explain me what Valsalva maneuver actually means, like squatting, what actually it does. So the conceptual things so that you use your brain to answer the question, I mean, conceptual wise rather than a memory wise. small concept notes to build blocks easily short notre
Murmur Dynamics: The Conceptual Framework
- Preload (how much blood fills the ventricle before it contracts = end-diastolic volume)
- Afterload (the resistance the ventricle pushes against)
The One Rule to Build Everything On
A bigger LV cavity = gradient decreases in dynamic obstruction (HOCM/MVP) A smaller LV cavity = gradient increases in dynamic obstruction (HOCM/MVP) All fixed obstruction murmurs (AS, MR, VSD, PDA) behave opposite - they are louder when more blood flows through them (increase with preload)
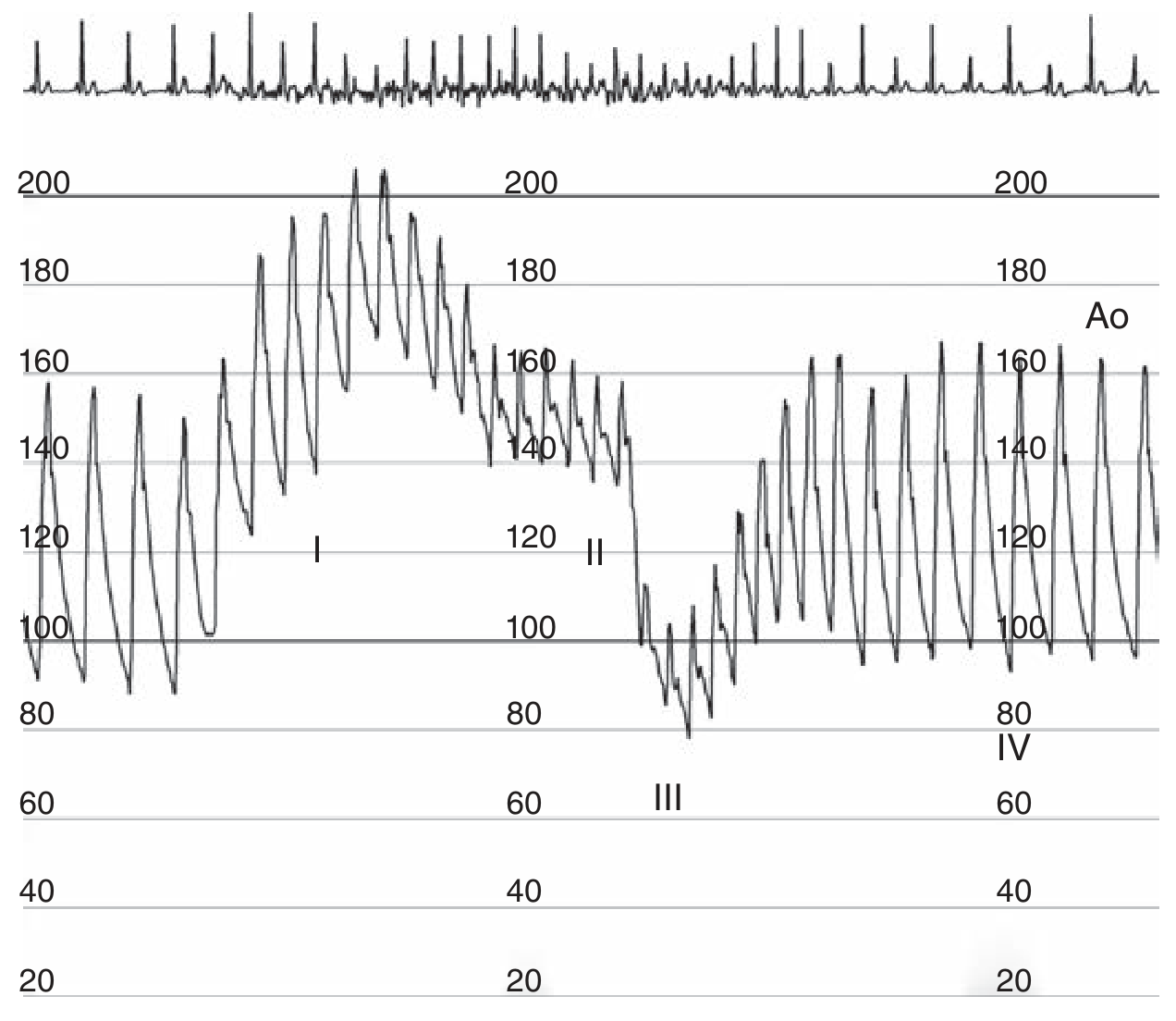
Valsalva Maneuver - What Actually Happens
- You forcefully close your glottis and contract your abdomen/thorax
- This briefly squeezes blood out of the pulmonary veins into the left side - tiny transient BP rise
- Sustained high intrathoracic pressure acts like squeezing the chest from outside
- This compresses the vena cava - venous return to the right heart drops
- Right heart fills less → less blood reaches the lungs → left heart filling drops
- Preload decreases. The LV becomes small and underfilled.
- Reflex tachycardia kicks in, pulse pressure narrows, BP drops
- Thoracic pressure drops suddenly
- Blood rushes back into the now-decompressed pulmonary circulation
- Brief further drop in aortic pressure
- Venous return suddenly normalizes
- Preload restored, BP overshoots above baseline
- Reflex bradycardia
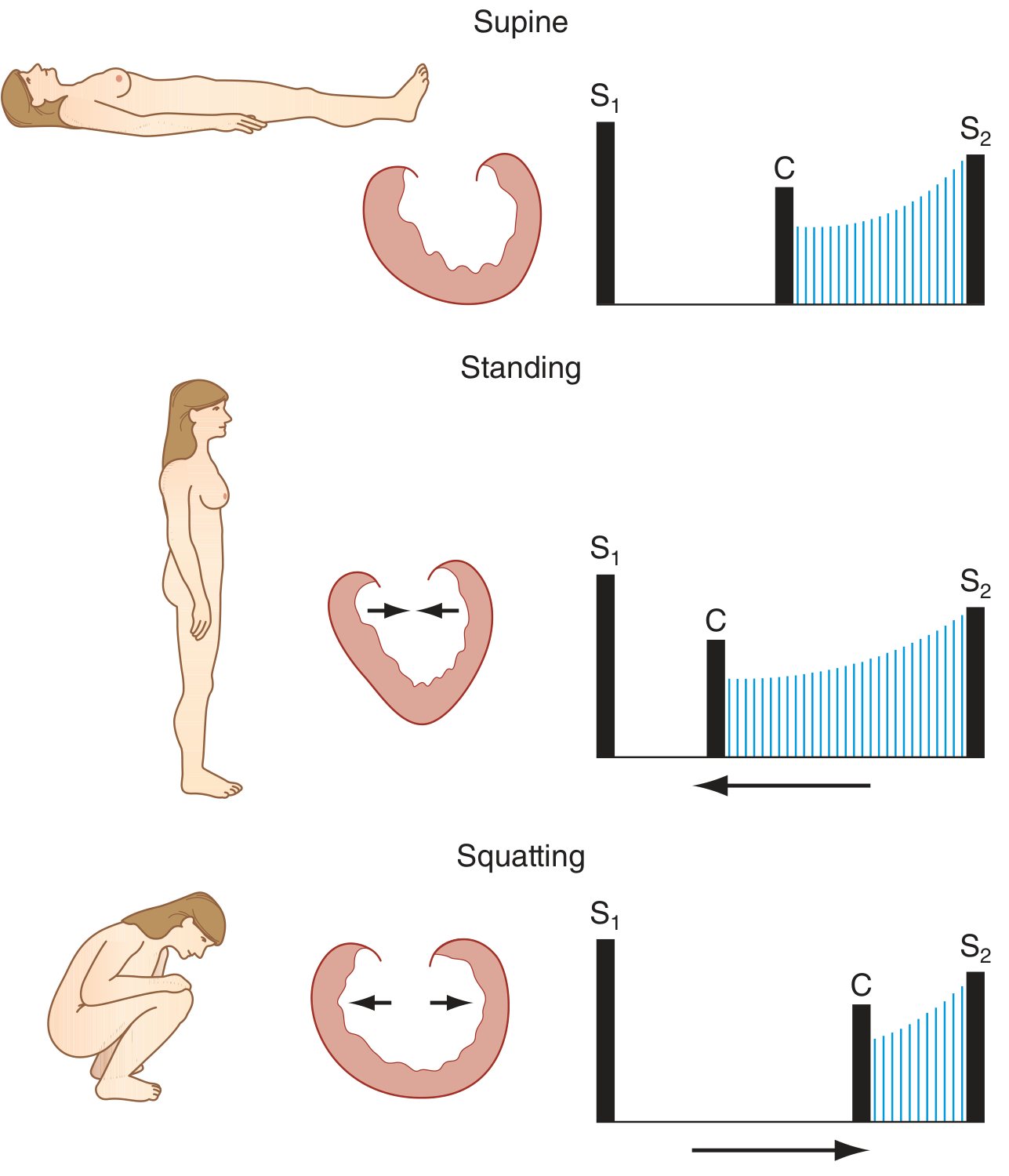
Squatting vs. Standing - What Actually Happens
Squatting
- The leg muscles compress the leg veins like squeezing a tube of toothpaste
- Venous return shoots up → preload increases
- At the same time, squatting also kinks the femoral arteries and increases peripheral vascular resistance → afterload increases
- Net effect: LV fills more, becomes bigger and fuller
Standing (rapidly from squat)
- Blood pools in the legs by gravity (venous pooling)
- Venous return drops → preload decreases
- Peripheral resistance drops too (afterload decreases)
- Net effect: LV fills less, becomes smaller
The Diagram Showing This (from Harrison's):
Applying This to the Two Key Murmurs
HOCM (Hypertrophic Obstructive Cardiomyopathy)
| Maneuver | Preload | LV size | Obstruction | Murmur |
|---|---|---|---|---|
| Valsalva (strain) | ↓ | Small | ↑ MORE | Louder |
| Standing | ↓ | Small | ↑ MORE | Louder |
| Squatting | ↑ | Big | ↓ LESS | Softer |
| Leg raise (passive) | ↑ | Big | ↓ LESS | Softer |
MVP (Mitral Valve Prolapse)
| Maneuver | LV size | When does prolapse happen | Click timing | Murmur duration |
|---|---|---|---|---|
| Standing | Small | Happens earlier in systole | Click → moves toward S1 | Longer murmur |
| Squatting | Big | Happens later (LV stays full longer) | Click → moves toward S2 | Shorter murmur |
| Valsalva (strain) | Small | Happens earlier | Click → toward S1 | Longer murmur |
All Other Murmurs (AS, MR-organic, VSD, TR, PS, etc.)
| Maneuver | Venous return / Flow | Murmur |
|---|---|---|
| Squatting | ↑ preload + ↑ afterload | Louder |
| Valsalva (strain) | ↓ preload | Softer |
| Standing | ↓ preload | Softer |
| Handgrip (isometric) | ↑ afterload | Louder (especially MR, AR, VSD) |
The Valsalva Aortic Pressure Trace (from Fuster & Hurst):
Summary Table for Quick Reference
| Condition | Valsalva (strain) | Standing | Squatting |
|---|---|---|---|
| HOCM | ↑ louder | ↑ louder | ↓ softer |
| MVP | ↑ longer + earlier click | ↑ longer + earlier click | ↓ shorter + later click |
| AS | ↓ softer | ↓ softer | ↑ louder |
| MR (organic) | ↓ softer | ↓ softer | ↑ louder |
| VSD | ↓ softer | ↓ softer | ↑ louder |
| AR | ↓ softer | ↓ softer | ↑ louder |
One-Line Core Concept to Never Forget
I told you very, very short note. I can't read. I'll get saturated if I have such long essays. Like exam-based NBME-ruled question-solving method, easy-to-remember and conceptual-based explanation, ultra-ultra-high-yield compact note.
Murmur Dynamics - Ultra Compact
One Core Concept
Small LV → HOCM/MVP worse Big LV → HOCM/MVP better, everyone else worse
What Each Maneuver Does to LV Size
| Maneuver | What happens | LV size |
|---|---|---|
| Valsalva (strain) | Bearing down → ↓ venous return | Small |
| Standing | Blood pools in legs → ↓ venous return | Small |
| Squatting | Leg veins compressed + ↑ resistance → ↑ venous return | Big |
The 2 Exceptions (HOCM + MVP)
Master Table
| Valsalva / Standing | Squatting | |
|---|---|---|
| HOCM | ↑ louder | ↓ softer |
| MVP | ↑ longer, click → S1 | ↓ shorter, click → S2 |
| AS / MR / VSD / AR | ↓ softer | ↑ louder |
NBME Answer Trigger
- "Louder with standing/Valsalva" → HOCM or MVP
- "Softer with squatting" → HOCM or MVP
- Distinguish HOCM vs AS? → Valsalva makes HOCM louder, AS softer
endocardial cushions mesns ELI5
Endocardial Cushions - ELI5
What They Build
| Structure | What it becomes |
|---|---|
| Top + bottom cushions fuse | AV septum (divides mitral from tricuspid) |
| Same fusion | Lower part of atrial septum (primum) |
| Same fusion | Upper part of ventricular septum (membranous) |
| Cushion tissue itself | Mitral + tricuspid valve leaflets |
If They Fail to Fuse (Down Syndrome classically)
- Hole between atria (primum ASD) + hole between ventricles (VSD) + abnormal AV valves
- All because the "handshake never happened"
One-Line Memory
Endocardial cushions = the middle wall of the heart. No fusion = everything in the middle is missing.
Technically, if you're seeing from the top to the bottom, it's basically like splitting atria into two and ventricle into two. But if you're talking about atrioventricular defects, it means a horizontal line, right? Side to side, like two people from the side are what walking towards the middle and fusing there. Hence, the atrioventricular septum is formed where the mitral valve and also the tricuspid valve are formed. If it's coming from the middle, there are no septums or walls where we have mitral and tricuspid. When it's horizontal line, we have atrial and mitral. Sorry, we have mitral and tricuspid. If it's a vertical line from the middle, then we have no defects in the middle, right?
Your Model is Correct
LA | RA
----+---- ← endocardial cushions fuse HERE (horizontal)
LV | RV
What That Horizontal Fusion Creates
- The floor of the atria / roof of the ventricles = AV septum
- Mitral valve (left side of fusion)
- Tricuspid valve (right side of fusion)
The Other Walls are Different Structures
| Wall | Built by |
|---|---|
| Vertical atrial wall (LA vs RA) | Septum primum + septum secundum (separate story) |
| Vertical ventricular wall (LV vs RV) | Muscular + membranous ventricular septum |
So Your Logic Holds
Cushion defect = hole at the AV plane = primum ASD + inlet VSD + bad valves Vertical walls = built by completely different embryological structures, cushions not involved
So, your explanation of coming from top and coming from bottom and meeting in the middle is not endocardial cushion, right? Endocardial cushion means coming from the left wall, right wall and meeting in the centre. That is what forms the atrioventricular septum and this is where the left side forms the mitral valve and the right side forms the tricuspid valve. These are the cushion defects. Am I right? Am I clear?
Actual Direction of Cushion Growth
What Your Model Gets Right
- Fusion happens at the center of the AV plane ✓
- Left side → mitral valve ✓
- Right side → tricuspid valve ✓
- Defect = hole at that plane + bad valves ✓
One Correction
So, is Eisenmenger syndrome reversible or irreversible? Irreversible. Because after the chronic left-to-right shunt, there will be fibrosis, hypertrophy of smooth muscles and hyperplasia of the intima and the pulmonary vasculature, and eventually it causes increasing pulmonary vascular resistance. So, and after some point, it will undergo a reversal of the shunt from right to left. This is how where cyanotic symptoms start appearing. So my next question, what NMBE always will attest it if Eisenmenger is reversible or irreversible? That is what the question in the asks, right?
What NBME Actually Tests
The One High-Yield Rule
Eisenmenger = surgical repair is CONTRAINDICATED
NBME Trigger Phrase
Why Polycythemia?
Three-Word Summary
| Stage | Shunt | Surgery? |
|---|---|---|
| Early L→R | L→R | ✅ Fix it |
| Eisenmenger | R→L | ❌ Too late |
Now make a small note of Eisenegger syndrome, including my knowledge, concept, functions, and only what we're going to do, and late what we're going to do. Small high yield, MB and MB level, compact, high yield, short note. Very, very short.
Eisenmenger Syndrome
Trigger
Mechanism
Symptoms (when R→L starts)
NBME Rule
| Timing | Action |
|---|---|
| Early (L→R, no cyanosis) | Fix the defect surgically ✅ |
| Late (Eisenmenger, cyanosis) | Surgery CONTRAINDICATED ❌ |
One-Line Trigger for MCQ
Late VSD/ASD/PDA + cyanosis + clubbing = don't touch the defect
See, I have one doubt now. Like on thiazide diuretics, thiazide diuretics are blocking sodium chloride co-transporter. That means it's preventing sodium and chloride reabsorption in the tubular fluid. That means the urine in urine, we are losing a lot of sodium and chloride. As sodium is going, water follows and that is the diuretic effect. Right, we are losing a lot of sodium and chloride. So, So indirectly, it's going to affect the sodium-calcium exchanger because they say that the intracellular sodium levels are dropped down now. As an exchanger to increase the intracellular sodium, we are going to take up a lot of calcium so that we'll drain sodium into the urine. In that case, first of all, the cells in the body only have low sodium. Now in an exchange for calcium, you are taking more calcium from the exchanger, from the urine and you are dumping sodium outside, right? In sodium-calcium exchanger, you are taking calcium into the blood and you are throwing sodium out into the urine. In this way, you are losing sodium doubly, right? Like through the reabsorption, you are blocking some of the sodium, losing sodium and also through the channel, we are absorbing calcium back and dumping back sodium. So, we are losing sodium double-handedly. Am I right? So my question is, how does a low intracellular sodium gonna stimulate sodium-calcium exchanger, which is causing in turn to lose more sodium and absorbing more calcium?
Where This Happens: Distal Tubule Cell
- Luminal side (facing urine)
- Basolateral side (facing blood)
Step by Step
- Normal job: 3 Na⁺ in → 1 Ca²⁺ out (into blood)
- Now intracellular Na⁺ is very low → exchanger works harder to bring Na⁺ in
- To bring Na⁺ in, it pumps more Ca²⁺ out into blood
- = Hypercalcemia / ↓ urine calcium
Your Confusion - Corrected
You said "dumping sodium into urine via NCX" - No.
Net Result
| Effect | |
|---|---|
| Na⁺ in urine | ↑ (lost - diuretic effect) |
| Ca²⁺ in urine | ↓ (reabsorbed back to blood) |
| Ca²⁺ in blood | ↑ (hypercalcemia) |
NBME Trigger
Thiazide = hypercalcemia (opposite of loop diuretics which waste calcium) Used in hypercalciuria / kidney stones to keep calcium in blood, out of urine
but the calcium has to come from the luminal side, right? Because the calcium is present in the urine should come into the vasolateral, come into the cell. And how is that gonna work?
The Full Two-Step Calcium Journey
URINE → [luminal side] → CELL → [basolateral side] → BLOOD
How Low Intracellular Na⁺ Drives the Whole Thing
Simple Flow
Low intracellular Na⁺
↓
NCX works harder → Ca²⁺ out to blood
↓
Intracellular Ca²⁺ drops
↓
TRPV5 pulls more Ca²⁺ from urine into cell
↓
Net: Ca²⁺ leaves urine → enters blood
got it
Imagine a parking brake on a pump. When the brake is engaged, the pump works sluggishly. When you release the brake, the pump runs at full speed. Phospholamban is that parking brake on SERCA (the sarcoplasmic reticulum calcium ATPase), the pump that sucks calcium back into the SR after each heartbeat. When phospholamban is unphosphorylated, it inhibits SERCA, slowing calcium reuptake. When sympathetic stimulation activates beta-1 receptors, protein kinase A phosphorylates phospholamban, releasing its inhibition on SERCA. Now SERCA pumps calcium into the SR faster — the heart relaxes more quickly (lusitropy) and the next contraction is stronger (inotropy, because more SR calcium is available for release). Now bridge to USMLE ↓ 2 On the Exam This is the molecular mechanism behind why sympathetic stimulation increases both contractility and relaxation rate. The phospholamban-SERCA interaction is the key step: phosphorylation removes the brake, allowing faster calcium cycling. On the exam, when they ask what is phosphorylated to increase contractility during sympathetic stimulation, the answer is phospholamban. When they ask which protein normally inhibits SERCA, the answer is phospholamban. It is a single-protein answer to both questions because phospholamban is the regulated brake on the calcium recycling pump. 🎯 The Trap the Exam Sets Students know sympathetic stimulation increases contractility but do not know the molecular step. Phospholamban phosphorylation is the specific mechanism by which beta-1 stimulation enhances SERCA activity. i want this concept as NBMe note
Phospholamban - NBME Note
One Line
Pathway
Two NBME Questions, One Answer
| Question | Answer |
|---|---|
| What inhibits SERCA normally? | Phospholamban |
| What is phosphorylated to ↑ contractility via β1? | Phospholamban |
The Trap
The NCX needs a steep sodium gradient to export calcium — flatten the gradient and calcium gets trapped inside. 1 The Story The Na+/Ca2+ exchanger (NCX) is a molecular seesaw: it uses the steep sodium gradient (high outside, low inside) to drive calcium OUT of the cell. For every calcium ion exported, three sodium ions rush in. The seesaw works because the sodium gradient provides the energy. Now imagine the sodium gradient gets flattened — sodium inside the cell rises (from digoxin blocking the Na/K ATPase or from any cause of intracellular sodium accumulation). The seesaw loses its driving force. The NCX can no longer efficiently export calcium, and calcium accumulates inside the cell. Now bridge to USMLE ↓ 2 On the Exam This is the molecular link between digoxin and increased contractility, but it is also a general principle. Anything that raises intracellular sodium will, through the NCX, raise intracellular calcium. On the exam, when they describe the mechanism by which sodium accumulation leads to calcium accumulation, the answer is impaired NCX function due to a reduced sodium gradient. The exchanger is not broken — it just lost the energy gradient that drives it. Think of it as a water wheel that stops spinning when the river level equalizes on both sides. 🎯 The Trap the Exam Sets Students memorize that 'sodium goes up, calcium goes up' without understanding why. The NCX is the link — it requires the sodium gradient as fuel for calcium extrusion. this concpt same lika above short note
NCX & Digoxin - NBME Note
One Line
Digoxin Pathway
Two NBME Questions, One Answer
| Question | Answer |
|---|---|
| Why does digoxin ↑ contractility? | NCX impaired due to ↑ intracellular Na⁺ |
| Link between Na⁺ accumulation and Ca²⁺ accumulation? | NCX loses its gradient = can't export Ca²⁺ |
The Trap
Memory Hook
NCX = seesaw powered by Na⁺ gradient. Flatten the gradient = seesaw stops = Ca²⁺ trapped inside.