
image.png
Explain topics along with diagram and flowcharts
analyse_media
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Here is the complete, richly structured reference covering all 15 topics with diagrams and flowcharts.
Reproductive Physiology - Complete Topic Guide
GROUP A: The Hypothalamo-Pituitary-Gonadal Axis
13. Hypothalamo-Pituitary-Ovarian (HPO) Axis
The HPO axis is the central control system for female reproduction. It operates differently in each phase of the menstrual cycle.
Key Hormones and Their Sources
| Hormone | Source | Action |
|---|---|---|
| GnRH (decapeptide) | Hypothalamic arcuate nuclei | Stimulates FSH & LH release (pulsatile) |
| FSH | Anterior pituitary | Granulosa cell growth + estradiol synthesis |
| LH | Anterior pituitary | Ovulation trigger + corpus luteum formation |
| Estradiol (E2) | Granulosa cells | Endometrial proliferation; feedback on HPO |
| Progesterone | Corpus luteum / Placenta | Endometrial secretory phase; negative feedback |
| Inhibin | Granulosa / Sertoli cells | Selective FSH suppression |
Feedback Flowchart - All Three Phases
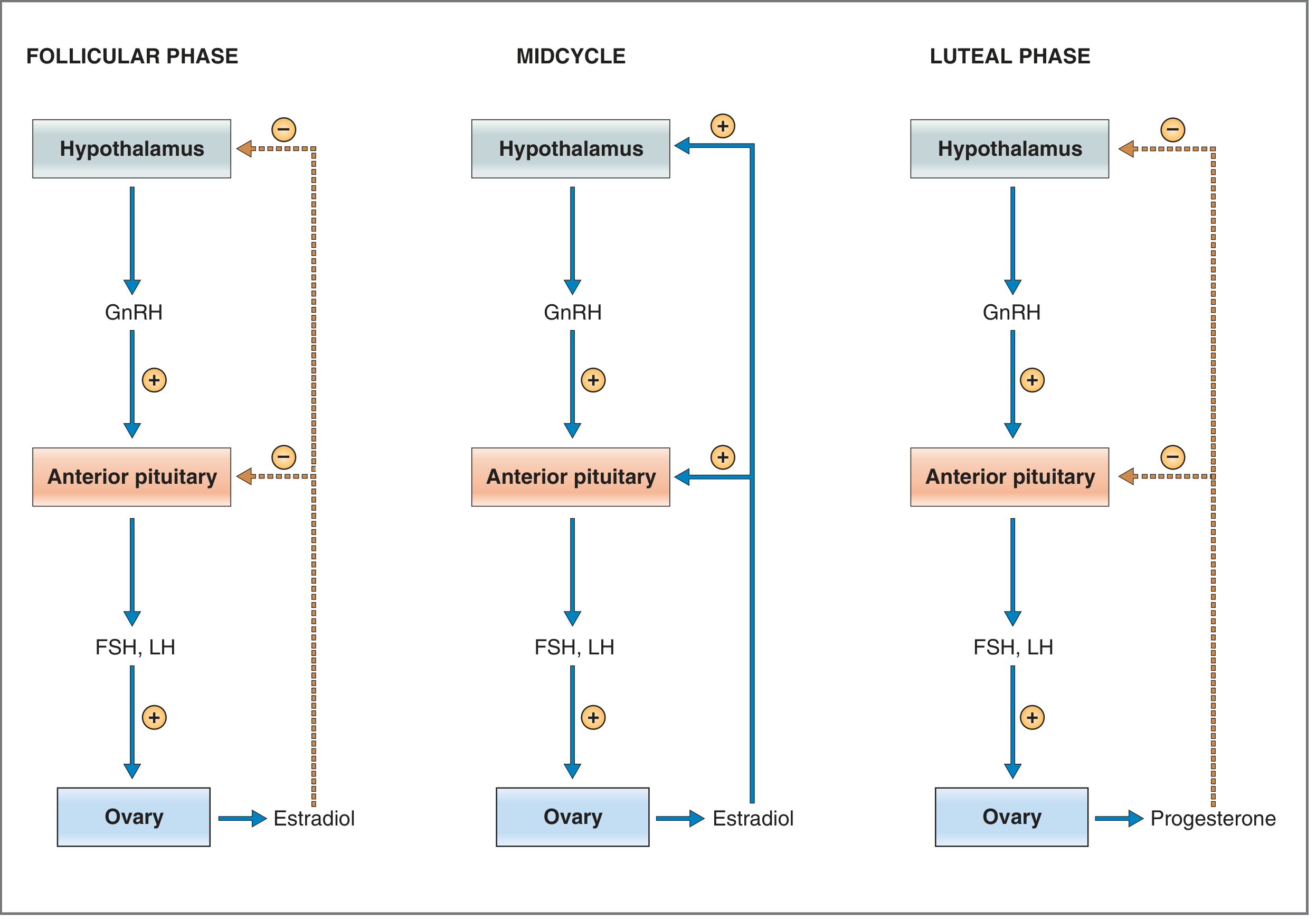
FOLLICULAR PHASE MIDCYCLE LUTEAL PHASE
───────────────── ───────────────── ─────────────────
Hypothalamus Hypothalamus Hypothalamus
│ GnRH │ GnRH │ GnRH
▼ (+) ▼ (+) ▼ (+)
Ant. Pituitary Ant. Pituitary Ant. Pituitary
│ FSH, LH │ FSH, LH ↑↑ │ FSH, LH
▼ (+) ▼ (+) ▼ (+)
Ovary Ovary Ovary
│ Estradiol ↑ │ Estradiol ↑↑↑ │ Progesterone ↑
└──► (−) feedback └──► (+) feedback └──► (−) feedback
on HPO (LH surge!) on HPO
Key rule: Low estradiol = negative feedback. Estradiol >200 pg/mL = switches to positive feedback, triggering the LH surge and ovulation.
4. Neuroendocrine Reflexes in Reproduction
These are reflex arcs where sensory inputs alter reproductive hormone release.
STIMULUS (sensory input)
│
▼
Neural pathway to hypothalamus
│
▼
GnRH secretion altered
│
▼
FSH/LH altered
│
▼
Gonadal response
Key Neuroendocrine Reflexes
| Reflex | Stimulus | Response | Example |
|---|---|---|---|
| Suckling reflex | Nipple stimulation | Oxytocin release; Prolactin ↑; GnRH ↓ | Lactation-induced anovulation |
| Ferguson reflex | Cervical/vaginal stretch | Oxytocin surge from posterior pituitary | Positive feedback in labor |
| Coital reflex | Copulation | LH surge (in induced ovulators like rabbits) | Reflex ovulation |
| Light/circadian | Photoperiod | Melatonin → GnRH modulation | Seasonal breeding |
| Stress reflex | CRH / cortisol ↑ | GnRH suppression → anovulation | Hypothalamic amenorrhea |
Critical axis:
Stress → ↑CRH → ↑ACTH → ↑Cortisol
│
└──► ↓GnRH → ↓FSH/LH → ↓Ovulation
GROUP B: The Menstrual Cycle
3. Menstrual Cycle
A 28-day cycle divided into two phases around ovulation on Day 14.
Phase Overview
| Phase | Days | Dominant Hormone | Endometrium |
|---|---|---|---|
| Menstrual | 1-5 | E2 & P4 fall | Shedding |
| Proliferative (Follicular) | 5-14 | Estrogen (E2) | Growth, gland elongation |
| Ovulation | Day 14 | LH surge | - |
| Secretory (Luteal) | 14-28 | Progesterone | Tortuous glands, glycogen, edema |
| Premenstrual | 26-28 | E2 & P4 fall | Spiral artery spasm |
Menstrual Cycle Flowchart
Day 1-5: MENSTRUATION
Corpus luteum degenerates → E2 & P4 ↓ → Spiral artery spasm
→ Endometrial necrosis + shedding
│
▼
Day 5-13: FOLLICULAR / PROLIFERATIVE PHASE
FSH ↑ → Follicle grows → E2 ↑
→ Endometrium proliferates (thickness: 1→10 mm)
→ Cervical mucus: watery, copious, "ferning" pattern, sperm-penetrable
│
▼
Day 13-14: OVULATORY PHASE
E2 > 200 pg/mL → Positive feedback → LH SURGE
→ Dominant follicle ruptures (day 14) → Secondary oocyte released
│
▼
Day 14-28: LUTEAL / SECRETORY PHASE
LH → Corpus luteum forms → Progesterone dominates
→ Glands tortuous + glycogen-rich
→ Cervical mucus: thick, non-elastic, non-ferning (blocks sperm)
→ BBT rises ~0.5°C (thermogenic effect of progesterone)
│
┌─────┴──────────────────────┐
│ If fertilized │ If NOT fertilized
▼ ▼
hCG maintains Corpus luteum → Corpus albicans
corpus luteum E2 & P4 fall → DAY 1 again
Cervical Mucus Changes (Clinical Tool)
| Phase | Consistency | Ferning | Spinnbarkeit | Significance |
|---|---|---|---|---|
| Follicular | Watery, abundant | Yes | >8 cm | Sperm entry permitted |
| Luteal | Thick, scanty | No | <3 cm | Sperm entry blocked |
| Ovulation | Max watery | Max fern | Max stretch | Peak fertility |
5. Mechanism of Ovulation
Ovulation is the rupture of the dominant Graafian follicle releasing the secondary oocyte.
Flowchart
Dominant follicle reaches 20 mm (Day 12-13)
│
▼
Estradiol ≥ 200 pg/mL for ≥ 50 hours
│
▼
POSITIVE FEEDBACK → GnRH pulse frequency ↑
│
▼
ANTERIOR PITUITARY: LH SURGE (10-12x rise)
│
▼
LH acts on follicle → ↑ prostaglandins (PGE2, PGF2α)
→ ↑ proteolytic enzymes (collagenase, plasmin)
→ Resumption of meiosis I in oocyte
│
▼
Follicular wall thins, stigma forms
│
▼
OVULATION: Follicle ruptures (~38 hrs after LH surge)
Secondary oocyte + cumulus oophorus expelled into peritoneum
│
▼
Fimbriae sweep oocyte into fallopian tube
│
▼
LUTEINIZATION: Granulosa + theca cells → Corpus luteum
Corpus luteum secretes Progesterone + Estradiol
Follicular Development Stages
| Stage | Duration | Diameter | Key Event |
|---|---|---|---|
| Primordial follicle | Years (from birth) | <0.03 mm | Primary oocyte arrested in prophase I |
| Primary follicle | Months | 0.1 mm | Granulosa proliferates; trophic FSH effect |
| Secondary (antral) | 70-85 days | 2-5 mm | Antrum forms with fluid; 2-cell/2-gonadotropin theory |
| Graafian follicle | Day 1-12 cycle | 5-20 mm | Dominant follicle selected; E2 surges |
| Ovulation | Day 14 | 20-25 mm | LH surge → rupture |
| Corpus luteum | Day 14-28 | - | Produces P4 for 14 days |
1. Indicators (Tests) of Ovulation and Their Clinical Significance
Table of Ovulation Indicators
| Test | Finding at Ovulation | Timing | Significance |
|---|---|---|---|
| Basal Body Temperature (BBT) | Rise of 0.2-0.5°C | Day after ovulation | Confirms ovulation (retrospective) |
| Cervical mucus (Spinnbarkeit) | >8 cm stretch | Just before ovulation | Peak fertility window |
| Ferning pattern | Crystalline fern pattern | Pre-ovulatory | Due to high E2; disappears post-ovulation |
| Serum LH (urine LH kit) | Sharp surge peak | 24-36 hrs before ovulation | Best predictor - used in fertility kits |
| Serum Progesterone | >3-5 ng/mL | Day 21 of cycle (mid-luteal) | Confirms ovulation occurred |
| Endometrial biopsy | Secretory endometrium | Mid-luteal | Confirms ovulation + adequate luteal phase |
| Ultrasound (USS) | Follicle ≥18 mm → collapses | Periovulatory | Direct visualization of follicle rupture |
| Mid-cycle pain (Mittelschmerz) | Unilateral pelvic pain | Around day 14 | Peritoneal irritation from follicular fluid |
| Vaginal cytology | Eosinophilic shift | Pre-ovulatory | Estrogen effect on vaginal epithelium |
Clinical Significance
- Infertility workup: Day-21 progesterone is the gold standard for confirming ovulation
- Safe period / rhythm method: Uses BBT + mucus pattern to identify infertile days
- ART timing: LH surge detected by urine kits for optimal intercourse/IUI timing
GROUP C: Spermatogenesis and Male Physiology
10. Spermatogenesis
The complete process from spermatogonium to mature sperm takes ~64-74 days total and occurs in the seminiferous tubules.
Spermatogenesis Flowchart
SPERMATOGONIUM (2n, diploid) - Seminiferous tubule basal layer
│ Mitosis (self-renewal + differentiation)
▼
TYPE A SPERMATOGONIUM → TYPE B SPERMATOGONIUM
│ Mitosis
▼
PRIMARY SPERMATOCYTE (2n, 46 chromosomes) - largest germ cell
│ MEIOSIS I (reduction division) - ~22 days
▼
2× SECONDARY SPERMATOCYTES (n, 23 chromosomes)
│ MEIOSIS II - hours
▼
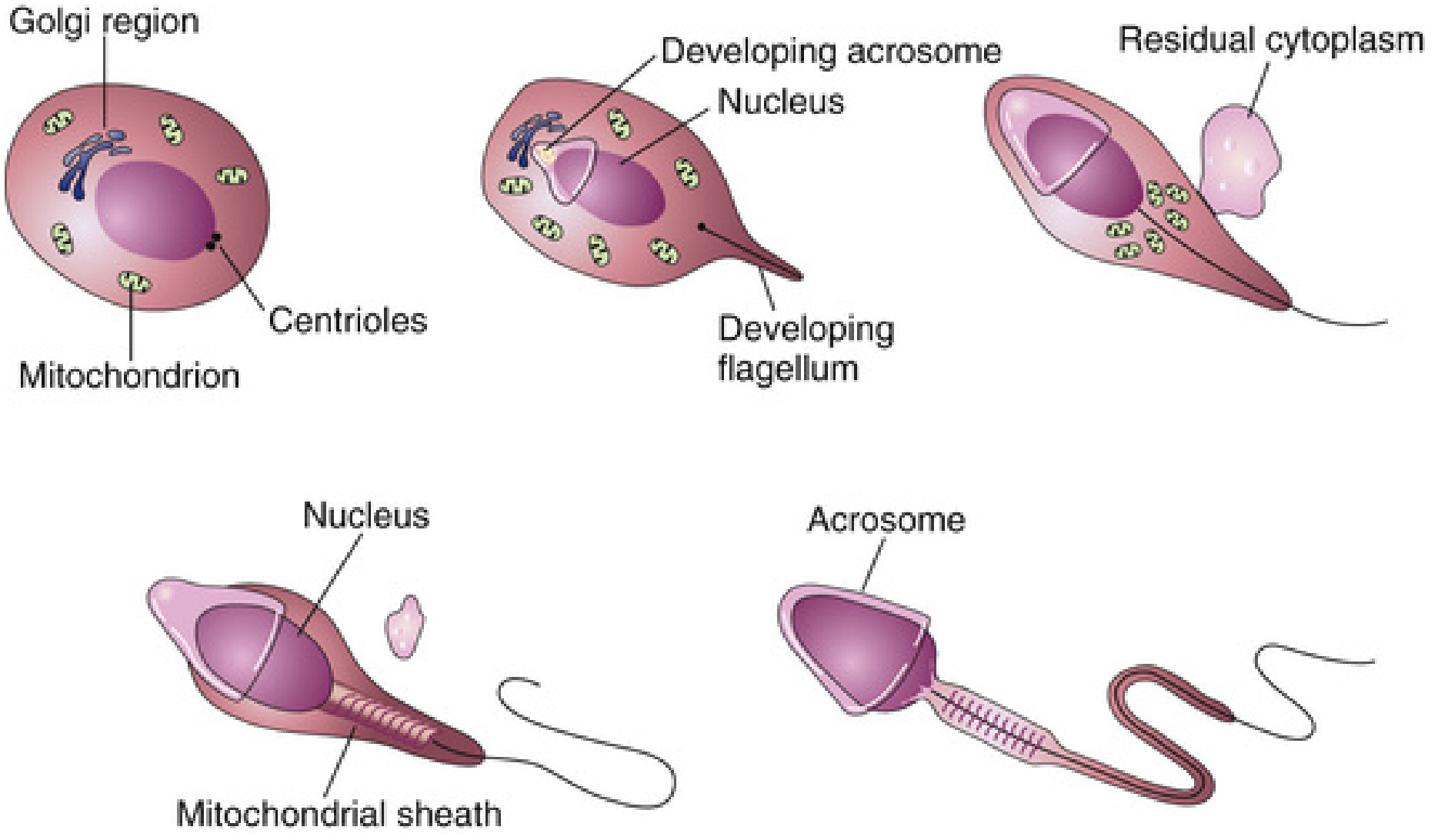
4× SPERMATIDS (n, 23 chromosomes - haploid round cells)
│ SPERMIOGENESIS (~24 days)
│ [Acrosome formation, tail growth, nucleus condensation,
│ cytoplasm shedding, mitochondrial sheath development]
▼
4× MATURE SPERMATOZOA
│
▼ (enter lumen of seminiferous tubule)
EPIDIDYMIS → functional maturation + storage (~12 days)
│
▼
DUCTUS DEFERENS → VAS DEFERENS → URETHRA
Spermiogenesis - Transformation Diagram
Hormonal Regulation
Hypothalamus → GnRH (pulsatile)
│
▼
Anterior Pituitary
├── FSH → Sertoli cells → supports spermatogenesis, secretes Inhibin
└── LH → Leydig cells → Testosterone → (paracrine) supports Sertoli cells
│
▼
TESTOSTERONE (+ FSH) → Complete spermatogenesis
Feedback:
Testosterone → (−) Hypothalamus & Pituitary (↓ GnRH, ↓ LH)
Inhibin → (−) Anterior Pituitary (↓ FSH selectively)
12. Functions of Sertoli Cells
Sertoli cells are "nurse cells" of the seminiferous tubules. They are stimulated by FSH and testosterone.
Summary Table
| Function | Mechanism | Significance |
|---|---|---|
| Structural support | Form tight junctions → Blood-Testis Barrier (BTB) | Protects haploid sperm from immune attack |
| Nutritional support | Provide lactate, amino acids, lipids to germ cells | Essential for germ cell survival |
| Phagocytosis | Engulf residual bodies shed during spermiogenesis | Cleans up excess cytoplasm |
| Hormone secretion | Inhibin (↓ FSH), androgen-binding protein (ABP), activin | Fine-tunes spermatogenesis |
| Androgen-binding protein | Concentrates testosterone in seminiferous tubule lumen | Maintains high local T for spermatogenesis |
| Testicular fluid secretion | Creates luminal flow to push sperm toward epididymis | Sperm transport |
| MIF (Müllerian Inhibiting Factor / AMH) | Secreted in fetal life | Causes regression of Müllerian ducts in males |
FSH + Testosterone
│
▼
SERTOLI CELL
┌──────────────────────────────────────┐
│ • Secretes ABP (concentrates T) │
│ • Secretes Inhibin → ↓ FSH │
│ • Secretes MIF/AMH (fetal) │
│ • Secretes transferrin │
│ • Phagocytoses residual bodies │
│ • Forms Blood-Testis Barrier │
│ • Nurtures developing spermatids │
└──────────────────────────────────────┘
GROUP D: Contraception
2. Methods of Contraception (Overview)
CONTRACEPTION METHODS
├── HORMONAL
│ ├── Combined OCP (estrogen + progestogen)
│ ├── Progestogen-only pill (mini-pill)
│ ├── Injectables (DMPA - Depo-Provera)
│ ├── Implants (subdermal progestogen)
│ └── Emergency contraception (levonorgestrel/ulipristal)
│
├── BARRIER
│ ├── Male condom
│ ├── Female condom
│ ├── Diaphragm + spermicide
│ └── Cervical cap
│
├── INTRAUTERINE
│ ├── Copper IUD (non-hormonal)
│ └── Levonorgestrel IUS (Mirena)
│
├── NATURAL / BEHAVIORAL
│ ├── Rhythm/Calendar method
│ ├── Basal body temperature method
│ ├── Billings (cervical mucus) method
│ └── Lactational amenorrhea method (LAM)
│
└── PERMANENT
├── Vasectomy (male)
└── Tubal ligation / Tubectomy (female)
11. Combined Oral Contraceptive Pills (COCP) - Mechanism of Action
Components
- Estrogen component: Ethinyl estradiol (20-35 mcg)
- Progestogen component: Levonorgestrel, norethindrone, desogestrel, drospirenone, etc.
Mechanism Flowchart
COMBINED OCP (Estrogen + Progestogen) taken daily
│
├──► Constant hormone levels
│
▼
1. SUPPRESS HPO AXIS (Primary mechanism)
Estrogen + Progestogen → negative feedback on hypothalamus & pituitary
→ ↓ GnRH pulsatility → ↓ FSH and LH → NO follicular development
→ NO LH surge → NO OVULATION
│
├──► 2. CERVICAL MUCUS THICKENING (Progestogen effect)
│ Thick, hostile mucus → sperm cannot penetrate cervix
│
├──► 3. ENDOMETRIAL CHANGES (Progestogen effect)
│ Thin, atrophic, non-receptive endometrium
│ → Impairs implantation even if fertilization occurs
│
└──► 4. TUBAL MOTILITY CHANGES (minor)
Altered peristalsis → delays sperm/egg transport
Pearl Index (failure rates/100 woman-years)
| Method | Typical use | Perfect use |
|---|---|---|
| COCP | 7-9 | 0.3 |
| Progestogen-only pill | 9 | 0.3 |
| Copper IUD | 0.8 | 0.6 |
| Condom (male) | 13 | 2 |
15. Hormonal Contraceptives (Full Classification)
| Type | Route | Hormones | Duration | Mechanism |
|---|---|---|---|---|
| Combined OCP | Oral daily | E2 + progestogen | Daily | Ovulation suppression + mucus |
| Progestogen-only pill | Oral daily | Progestogen only | Daily | Mucus + partial ovulation suppression |
| Emergency contraceptive | Oral | Levonorgestrel (1.5mg) or Ulipristal | Single dose (within 72/120h) | Delays ovulation; may inhibit implantation |
| DMPA (Depo-Provera) | IM injection | Medroxyprogesterone acetate | 3 months | Ovulation suppression |
| Subdermal implant (Nexplanon) | Subcutaneous | Etonogestrel | 3 years | Ovulation suppression + mucus |
| Hormonal IUS (Mirena) | Intrauterine | Levonorgestrel | 5 years | Local: mucus + endometrium |
| Combined patch | Transdermal | E2 + progestogen | Weekly (3/4 weeks) | Same as COCP |
| Vaginal ring (NuvaRing) | Vaginal | E2 + etonogestrel | Monthly | Same as COCP |
8 & 9. Rhythm Method of Contraception and Safe Period
Both methods exploit the predictable infertile window in the cycle.
Calendar/Rhythm Method
Based on a 28-day cycle:
Ovulation → Day 14
Sperm survival → up to 5 days
Egg survival → 12-24 hours
FERTILE WINDOW = Day 9 to Day 15 (avoid unprotected sex)
SAFE PERIOD = Day 1-8 (post-menstrual) + Day 16-28 (pre-menstrual)
Calculation Rule (for irregular cycles)
Record last 6-12 cycles
Shortest cycle - 18 = First fertile day
Longest cycle - 11 = Last fertile day
e.g., 26-30 day cycles:
First fertile: 26 - 18 = Day 8
Last fertile: 30 - 11 = Day 19
Lactational Amenorrhea Method (LAM)
Three conditions must ALL be met:
- Baby < 6 months old
- Exclusive breastfeeding (day and night)
- Amenorrhea (no periods returned)
Efficacy: >98% when all three criteria met.
GROUP E: Pregnancy, Placenta, and Parturition
6. Physiological Changes During Pregnancy
System-by-System Table (from Morgan & Mikhail's Clinical Anesthesiology)
| System | Change | Clinical Implication |
|---|---|---|
| Cardiovascular | Cardiac output +40%; HR +20%; Blood volume +35%; Plasma volume +55% | Physiological anemia; increased cardiac work |
| Blood pressure | Systolic -5%; Diastolic -15%; SVR -15% | Hypotension common; aortocaval compression in supine |
| Respiratory | Minute ventilation +50%; TV +40%; RR +15%; FRC -20% | ↑ PaO2; ↓ PaCO2 (respiratory alkalosis compensated) |
| O2 consumption +20-50%; Airway resistance -35% | Rapid desaturation during apnea | |
| Hematological | RBCs +20%; Plasma +55% → Hb -20% (dilutional anemia) | Hb ~11 g/dL is normal; ↑ clotting factors (+30-250%) |
| Coagulation | Hypercoagulable state | VTE risk ↑ 5x; DIC risk in placental abruption |
| Renal | GFR +50%; Creatinine ↓ | Normal creatinine in pregnancy = 0.4-0.8 mg/dL |
| GI | Gastric emptying delayed; LES tone ↓; Progesterone relaxes smooth muscle | Risk of aspiration ↑ |
| Endocrine | hCG surge (first trimester); Estrogen ↑↑↑; Progesterone ↑↑↑; HPL ↑ | Insulin resistance → gestational diabetes risk |
| CNS | MAC (anesthetic requirement) -40% | Reduced drug doses needed |
Hormone Changes Flowchart
CONCEPTION
│
▼
Trophoblast → hCG secretion begins (Day 8-10)
│ hCG peaks at 8-10 weeks
│ hCG maintains corpus luteum
│ → Corpus luteum → E2 + P4
▼
PLACENTA forms (8-10 weeks) → Takes over steroid production
│
├── Progesterone: synthesized entirely by placenta from maternal cholesterol
│ → Maintains uterine quiescence; prevents preterm labor
│
└── Estriol (E3): Requires fetal DHEAS (adrenal) + fetal liver + placenta
→ Used as marker of fetal wellbeing
│
▼
FIRST TRIMESTER: hCG ↑ (morning sickness, thyroid stimulation)
SECOND TRIMESTER: HPL ↑ (insulin resistance, fetal fuel partitioning)
THIRD TRIMESTER: E3 ↑↑, P4 ↑↑, cortisol ↑ (maturation of fetal organs)
14. Functions of the Placenta
The placenta is a transient, highly specialized organ serving as the fetal lung, gut, kidney, liver, and endocrine gland.
PLACENTA FUNCTIONS
├── TRANSPORT
│ ├── O2 delivery to fetus (diffusion, fetal Hb has higher O2 affinity)
│ ├── CO2 removal from fetus
│ ├── Glucose (facilitated diffusion - most important fetal fuel)
│ ├── Amino acids (active transport)
│ ├── Fatty acids (diffusion)
│ ├── IgG (active transport - passive immunity to fetus)
│ └── Water, electrolytes, vitamins
│
├── ENDOCRINE
│ ├── hCG: Maintains corpus luteum; basis of pregnancy test; TSH-like action
│ ├── hPL (Human Placental Lactogen): Insulin antagonist; promotes lipolysis
│ │ (spares glucose for fetus)
│ ├── Progesterone: Uterine quiescence; breast preparation
│ ├── Estrogens (E1, E2, E3): Uterine growth; ductal breast development
│ └── CRH: Drives fetal cortisol production near term; linked to labor onset
│
└── BARRIER (selective)
├── Blocks most maternal antibodies EXCEPT IgG
├── Blocks most bacteria (but NOT viruses like CMV, rubella, HIV)
└── Blocks some drugs (but NOT alcohol, nicotine, warfarin, thalidomide)
7. Parturition
Parturition (labor and delivery) occurs at ~40 weeks gestation. The exact trigger is multifactorial.
Hormonal Mechanism of Parturition
NEAR TERM (38-40 weeks)
│
▼
Fetal hypothalamic-pituitary-adrenal axis activated
│
▼
Fetal cortisol ↑
│
▼
↑ Estrogen : Progesterone ratio in uterus
(Cortisol converts P4 → E2 via placental enzymes)
│
├──► E2 stimulates:
│ • Oxytocin receptors ↑ (up-regulated on uterine muscle)
│ • PGE2 and PGF2α production ↑
│ • Gap junction formation between myometrial cells
│
└──► P4 inhibition removed → Uterus becomes "primed"
│
▼
OXYTOCIN (Ferguson reflex: cervical stretch → oxytocin ↑)
│ + PROSTAGLANDINS
▼
Uterine contractions (coordinate, synchronized via gap junctions)
│
▼
LABOR - THREE STAGES:
Stage 1: Cervical dilation + effacement (longest stage)
Stage 2: Fetal expulsion through birth canal
Stage 3: Placental delivery (+ uterine contraction to stop bleeding)
│
▼
After delivery: E2, P4 fall rapidly → Prolactin ↑ → LACTATION begins
Key Players in Parturition
| Hormone/Mediator | Role |
|---|---|
| Fetal cortisol | Initiates E2/P4 ratio shift |
| Estrogen | Up-regulates oxytocin receptors, gap junctions, PG synthesis |
| Progesterone | "Uterine quiescence" - its withdrawal allows labor |
| PGE2 / PGF2α | Cervical ripening (effacement + dilation); ↑ intracellular Ca2+ |
| Oxytocin | Powerful uterotonic; receptors up-regulated at term |
| Relaxin | Softens symphysis pubis + cervical collagen |
| CRH | Rises sharply at term; may act as "placental clock" |
GROUP F: Gametogenesis
10. Spermatogenesis (Comparison Table with Oogenesis)
| Feature | Spermatogenesis | Oogenesis |
|---|---|---|
| Starts | Puberty | Fetal life (20-24 weeks gestation) |
| Continuous? | Yes - throughout adult life | No - arrested at prophase I until ovulation |
| Pool | Continuously renewed | Fixed pool, declining from birth |
| At birth | Spermatogonia dormant | 2 million oocytes (arrested in prophase I) |
| At puberty | Resumes full production | 400,000 oocytes |
| At menopause | No equivalent | Pool exhausted |
| Products | 4 functional sperm per primary spermatocyte | 1 egg + 3 polar bodies |
| Duration | ~64-74 days | Years (arrested) + 24 hrs |
| Site | Seminiferous tubules | Ovarian follicles |
Summary Flowchart: Integration of All Topics
HYPOTHALAMUS
GnRH (pulsatile)
│
▼
ANTERIOR PITUITARY
FSH ──────────────────────────► Follicle growth (Spermatogenesis in males)
LH ───────────────────────────► Ovulation / Corpus luteum (Testosterone in males)
│ │
│ ┌───────────┘
│ │
▼ ▼
OVARY / TESTIS MENSTRUAL CYCLE (28 days)
E2, P4, Inhibin [Follicular → Ovulation → Luteal → Menstruation]
│
▼ (if fertilized)
PREGNANCY
hCG → maintains corpus luteum
Placenta → E2, P4, hPL, hCG
Physiological changes in all organ systems
│
▼ (at 40 weeks)
PARTURITION
Fetal cortisol → ↑ E2/P4 ratio → Prostaglandins + Oxytocin → Labor
│
▼
LACTATION
Prolactin ↑ (milk production) + Oxytocin (milk ejection)
→ Suckling → ↓ GnRH → Lactational amenorrhea
Quick Reference: Ovulation Indicators + Safe Period Summary
MENSTRUAL CYCLE DAY:
1 5 8 9 13 14 15 16 21 28
│ │ │ │ │ │ │ │ │ │
MENSES │ │ │ │ │ │ │ │
│ FERTILE WINDOW (Days 9-15)│
│ │───────────│ │ │ │
│ │ ↑ LH SURGE (day 13) │
│ │ │ OVULATION (d14) │
│ │ │
PROLIFERATIVE PHASE SECRETORY (LUTEAL) PHASE
(E2 dominance) (P4 dominance + BBT ↑)
BBT: Low until ovulation → Rises 0.5°C on day after ovulation
Ferning: Present Day 8-13 → Absent post-ovulation
Progesterone: Checked Day 21 → >3 ng/mL confirms ovulation
Sources:
- Costanzo Physiology, 7th Edition (Chapters 9-10: Male and Female Reproduction)
- The Developing Human: Clinically Oriented Embryology (Chapter 2: Spermatogenesis, Oogenesis)
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition (Chapter 40: Physiological Changes in Pregnancy)
- Ganong's Review of Medical Physiology, 26th Edition (Chapter: Menstrual Cycle, Parturition)
This is a shared conversation. Sign in to Orris to start your own chat.