Pelvic floor formation (prolapses) gynaecology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"pelvic organ prolapse" management
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content to write a detailed, well-structured answer. Let me compile everything.
Pelvic Floor & Pelvic Organ Prolapse (POP) — Gynaecology
1. Pelvic Floor Anatomy
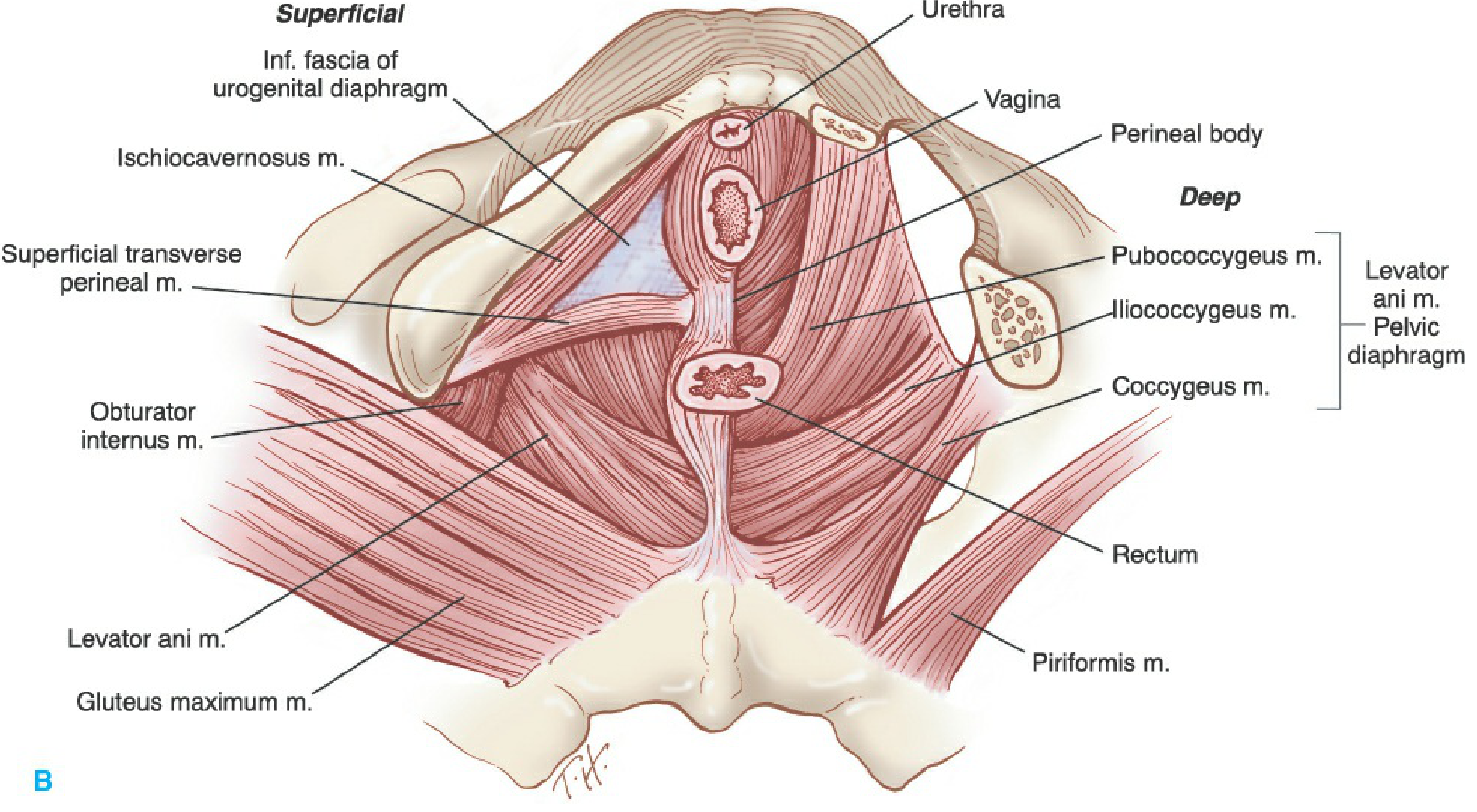
The pelvic floor is a funnel-shaped fibromuscular partition closing the pelvic outlet from the skin inferiorly to the peritoneum superiorly. It is divided by the pelvic diaphragm into a pelvic and a perineal portion.
Key Structures
| Structure | Components | Function |
|---|---|---|
| Pelvic diaphragm | Levator ani + coccygeus muscles + superior/inferior fasciae | Primary support hammock; holds pelvic floor closed |
| Levator ani | Pubococcygeus (pubovaginalis, pubourethralis), puborectalis, iliococcygeus | Lifts and closes the pelvic floor; perforated by urethra, vagina, rectum |
| Urogenital diaphragm (perineal membrane) | Deep transverse perineal muscle + sphincter urethrae | Anterior perineal support |
| Perineal body | Fibromuscular central tendon of perineum | Anchors posterior perineal structures |
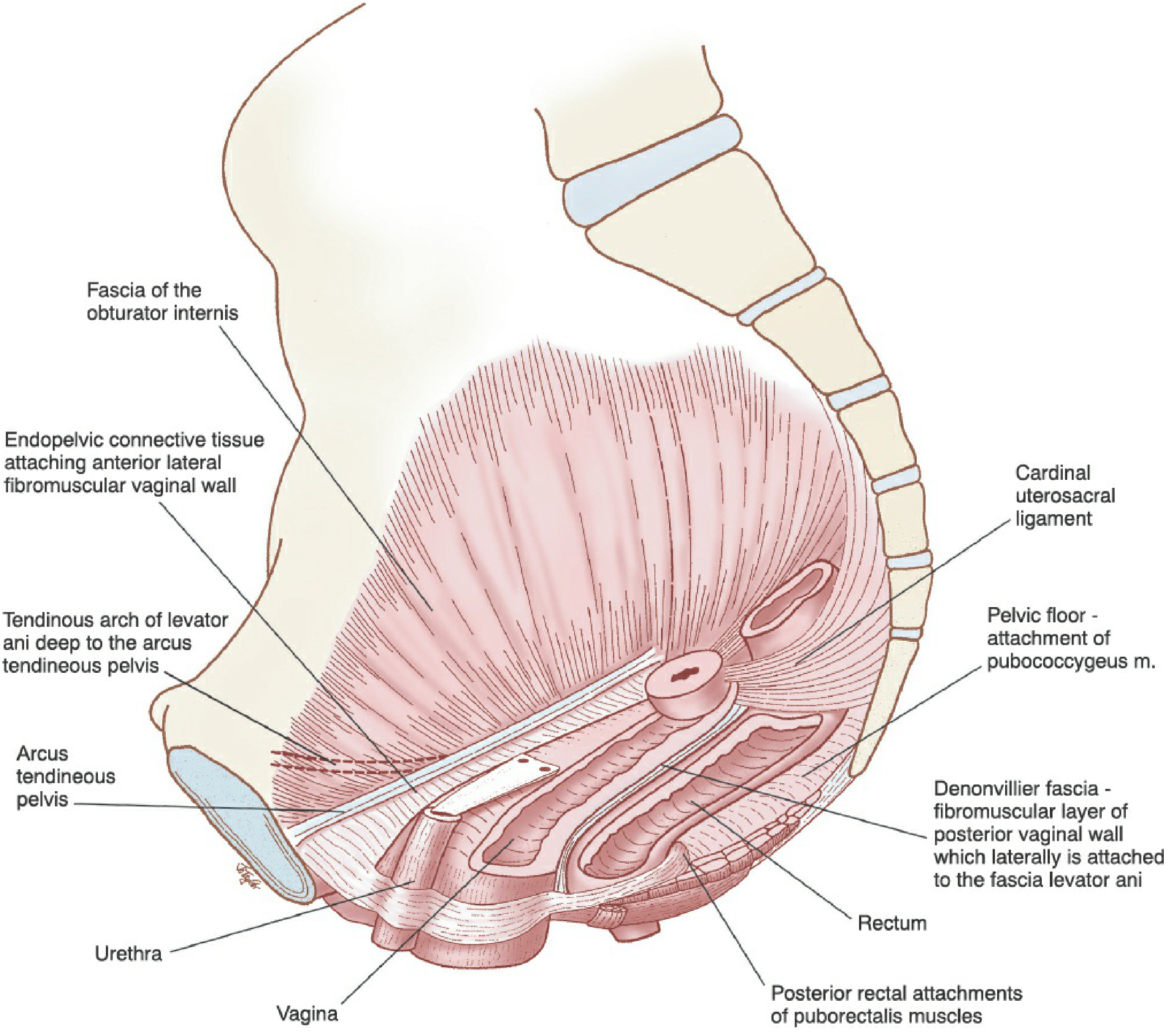
The levator ani originates from the arcus tendineus levator ani (a thickening of the obturator fascia extending from pubic body to ischial spine) and inserts into the perineal body, vaginal wall, anococcygeal ligament, and coccyx.
Endopelvic Fascia & Ligaments
The endopelvic (visceral) fascia envelops the pelvic organs and, via parietal condensations, forms the key suspensory ligaments:
- Cardinal ligament — lateral cervical support to pelvic sidewall
- Uterosacral ligament — posterior apical support to the sacrum
- Pubocervical fascia — anterior vaginal support
- Rectovaginal (Denonvilliers) fascia — posterior vaginal support, attached laterally to fascia of levator ani
Three Levels of Vaginal Support (DeLancey)
| Level | Structures | Supports |
|---|---|---|
| Level I | Cardinal/uterosacral ligament complex | Vaginal length and axis; uterus/vaginal apex |
| Level II | Paravaginal attachments of lateral vagina to arcus tendineus and levator fascia | Midline position of the vagina |
| Level III | Distal vaginal muscles and connective tissue; perineal body | Distal vagina and perineum |
2. Definition & Epidemiology
Pelvic organ prolapse (POP) = descent of one or more of the anterior vaginal wall, posterior vaginal wall, uterus/cervix, or vaginal apex, resulting in herniation of pelvic organs through the urogenital diaphragm.
- Prevalence of at least one pelvic floor disorder: 23.7% in US women; more than doubles in women ≥80 years
- Lifetime probability of surgery for POP by age 80: ~12.6%; combined risk (POP + SUI surgery) reaches 20.2% by age 80
- Most common segment to prolapse: anterior compartment (34.3% anterior, 18.6% posterior, 14.3% uterine in WHI data)
3. Risk Factors / Pathophysiology
POP results from attenuation of supportive structures through actual tears/breaks in fascia and ligaments, neuromuscular dysfunction, or both — allowing the levator hiatus to enlarge and organs to descend.
Risk Factors
| Category | Factors |
|---|---|
| Obstetric | Vaginal delivery (×2 risk vs nulliparous), multiparity, prolonged second stage, instrumental delivery |
| Age & hormonal | Postmenopausal oestrogen deficiency (atrophic changes in fascia/connective tissue) |
| Anatomical | History of hysterectomy, prior prolapse surgery |
| Mechanical/lifestyle | Chronic constipation (straining), obesity, chronic cough/COPD |
| Genetic/connective tissue | Connective tissue disorders, race (White women higher risk than Black) |
Birth-induced injury to the pubococcygeal portion of levator ani is seen in 55% of women with prolapse vs 16% of women with normal support. — Berek & Novak's Gynecology
4. Types & Definitions
Prolapse is described by vaginal compartment, not by the underlying organ (traditional terms like "cystocele/rectocele" are increasingly replaced by compartment terminology, per the POP-Q system):
| Traditional Term | Compartment | Mechanism |
|---|---|---|
| Cystocele | Anterior | Descent of bladder with anterior vaginal wall; pubocervical fascia weakens midline or detaches laterally from arcus tendineus |
| Urethrocele | Anterior distal | Descent of urethra alone (rare in isolation) |
| Cystourethrocele | Anterior | Descent of both bladder and urethra |
| Enterocele | Apical/posterior | True hernia — peritoneal sac containing small bowel descends between uterosacral ligaments into the rectovaginal space; only true hernia among pelvic support disorders |
| Rectocele | Posterior | Protrusion of rectum into vaginal lumen from weakness in rectal wall and paravaginal fibromuscular connective tissue |
| Uterine prolapse | Apical | Poor cardinal/uterosacral ligament support → downward protrusion of cervix and uterus |
| Vaginal vault prolapse | Apical | Post-hysterectomy descent of the vaginal cuff |
| Procidentia | All compartments | Complete uterine + vaginal eversion (Stage IV) |

5. POP-Q Staging System
The Pelvic Organ Prolapse Quantification (POP-Q) system is the international standard for grading prolapse objectively. Reference point = the hymenal ring (0 cm).
| Stage | Definition |
|---|---|
| 0 | No prolapse; all points at −3 cm (or less), Point C ≥ −(TVL−2) |
| I | Leading edge > 1 cm above the hymen (< −1 cm) |
| II | Leading edge within 1 cm proximal or distal to the hymen (−1 to +1 cm) |
| III | Leading edge > 1 cm below hymen but < (TVL−2 cm) |
| IV | Complete eversion; leading edge ≥ (TVL−2 cm) |
Six measured points: Aa, Ba (anterior), C, D (apical), Ap, Bp (posterior), plus total vaginal length (TVL) and genital hiatus (gh) and perineal body (pb).
6. Clinical Features
Symptoms
- Vaginal bulge visible or palpable — most specific symptom for POP; almost always present when prolapse extends beyond the hymen
- Pelvic pressure/heaviness, worse on prolonged standing
- Urinary symptoms: stress urinary incontinence (SUI), frequency, nocturia, voiding difficulty (urethral kinking by prolapse can actually mask SUI — occult SUI)
- Defecatory symptoms: constipation, incomplete emptying, need to splint (manually reduce the prolapse to defaecate)
- Sexual dysfunction: dyspareunia, negative body image
- Low backache, vaginal discharge or ulceration (from exposed epithelium in severe cases)
Key point: Symptoms correlate poorly with the site and size of prolapse until the leading edge passes beyond the hymenal ring. Bowel symptoms (constipation) alone should rarely prompt surgery for posterior compartment repair.
7. Assessment
- History: symptom onset, obstetric history, bowel/bladder function, sexual function, prior surgery
- Physical examination: supine (lithotomy) and standing/straining; assess each compartment individually; POP-Q measurement
- Bladder function: post-void residual (PVR ≤100 mL acceptable if void ≥150 mL); prolapse reduction stress test (pessary or speculum) to unmask occult SUI
- Bowel function: if posterior repair planned, consider anorectal physiology (manometry, defaecography)
- Urodynamics: for complex lower urinary tract symptoms or before surgery
8. Management
Conservative (Non-Surgical)
| Approach | Details |
|---|---|
| Pelvic floor muscle training (PFMT / Kegel exercises) | First-line; supervised physiotherapy improves levator function; evidence for symptom reduction in Stage I–II |
| Lifestyle modification | Weight loss, treat constipation, smoking cessation (reduce COPD/chronic cough) |
| Topical oestrogen | Improves vaginal atrophy, tissue quality; used pre-operatively and long-term |
| Pessary | Intravaginal mechanical device; suitable for all stages; ring pessary for Stage I–II; Gellhorn/donut/cube for Stage III–IV; must be followed up at 4–12 weekly intervals if patient cannot self-manage |
Surgical Management
Surgery is individualised and guided by compartment affected, severity, uterus present/absent, patient age and activity level, and desire for future fertility.
Principles:
- Address all compartments including the apex (failure to suspend the apex is the leading cause of recurrent anterior prolapse)
- Choice of approach: vaginal vs abdominal (laparoscopic/robotic)
- Choice of repair type: native tissue vs synthetic mesh augmentation
- Reconstructive (restores anatomy) vs obliterative (colpocleisis — for women who no longer require vaginal intercourse)
Apical Procedures
| Procedure | Approach | Key Feature |
|---|---|---|
| Sacrospinous ligament fixation (SSLF) | Vaginal | Vaginal cuff suspended to sacrospinous ligament; risk of pudendal nerve/vessel injury |
| Uterosacral ligament suspension (USLS) | Vaginal/laparoscopic | Restores natural apical axis; risk of ureteric kinking (check cystoscopy) |
| Sacrocolpopexy | Abdominal/laparoscopic | Mesh bridge from vaginal apex to sacral promontory; gold standard for vault prolapse — high long-term success |
| McCall culdoplasty | Vaginal (at time of hysterectomy) | Uterosacral ligament plication |
Anterior Compartment
- Anterior colporrhaphy (native tissue): plication of pubocervical fascia; acceptable short-term but higher recurrence long-term
- Paravaginal repair: repair of lateral defect detachment from arcus tendineus (retropubic or vaginal approach)
Posterior Compartment
- Posterior colporrhaphy ± levatorplasty: plication of rectovaginal fascia; indicated when sensation of posterior bulge or need to splint
- Perineorrhaphy: repair of perineal body deficiency
Obliterative Procedures
- Colpocleisis (LeFort or complete): obliterates vaginal canal; high success and low complication rates; appropriate for elderly women no longer sexually active
9. Special Considerations
- Uterine preservation vs hysterectomy: Historically, hysterectomy was standard for uterine prolapse, but uterine-preserving procedures (sacrohysteropexy, Manchester repair) are gaining evidence and are appropriate for women desiring preservation
- Mesh controversy: Following regulatory actions (FDA, MHRA), transvaginal mesh for anterior/posterior repair is now restricted or banned in many countries due to mesh erosion/exposure complications; abdominal mesh (sacrocolpopexy) retains a strong evidence base
- Occult SUI: Women with advanced prolapse may develop de novo or unmasked SUI after repair; consider concomitant mid-urethral sling if demonstrated on reduction stress testing
Recent Evidence
A 2025 meta-analysis (PMID 40120730) found a significant association between prior hysterectomy and subsequent pelvic floor disorders including POP, reinforcing the importance of concurrent apical suspension at the time of hysterectomy.
Sources: Berek & Novak's Gynecology, Chapter 30 (Pelvic Organ Prolapse) & Chapter 5 (Pelvic Anatomy); Campbell-Walsh-Wein Urology, Part XIII (Vaginal Prolapse, Pelvic Floor Defects, POP-Q Classification)
5.After an IV bolus, the drug concentration declined along a biphasic curve. Plot the graph in semi-logarithmic coordinates and identify the α- and β-phases. What is the clinical significance of each phase?
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.