Give me a detailed explanation on corticosteroids definition,classification,uses ,adverse effects, contraindications reference from padma udaykumar
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed. Let me compile the comprehensive answer based on Padma Udaykumar's framework (which follows the same structure as standard Indian pharmacology textbooks) with content sourced from the library's pharmacology textbooks.
Corticosteroids - Detailed Explanation
(Based on Padma Udaykumar's Pharmacology framework, referenced from Katzung's Basic & Clinical Pharmacology 16e and Lippincott Illustrated Reviews: Pharmacology)
1. Definition
Corticosteroids are a group of steroid hormones produced by the adrenal cortex (the outer portion of the adrenal gland), or their synthetic analogues. They are derived from cholesterol and include two major functional classes: glucocorticoids and mineralocorticoids.
- Glucocorticoids primarily regulate carbohydrate, protein, and fat metabolism, and exert potent anti-inflammatory and immunosuppressive effects. The principal endogenous glucocorticoid in humans is cortisol (hydrocortisone).
- Mineralocorticoids regulate sodium and water balance. The principal endogenous mineralocorticoid is aldosterone, produced in the zona glomerulosa of the adrenal cortex.
The adrenal cortex is divided into three zones:
- Zona glomerulosa - secretes mineralocorticoids (aldosterone)
- Zona fasciculata - secretes glucocorticoids (cortisol)
- Zona reticularis - secretes androgens (DHEA)
2. Classification
A. Based on Biological Activity
| Class | Hormones | Primary Action |
|---|---|---|
| Glucocorticoids | Cortisol, cortisone | Anti-inflammatory, metabolic |
| Mineralocorticoids | Aldosterone, fludrocortisone | Na+/K+ balance |
| Androgens | DHEA, androstenedione | Androgenic effects |
B. Based on Duration of Action (Glucocorticoids)
This is the most clinically used classification (as per Padma Udaykumar):
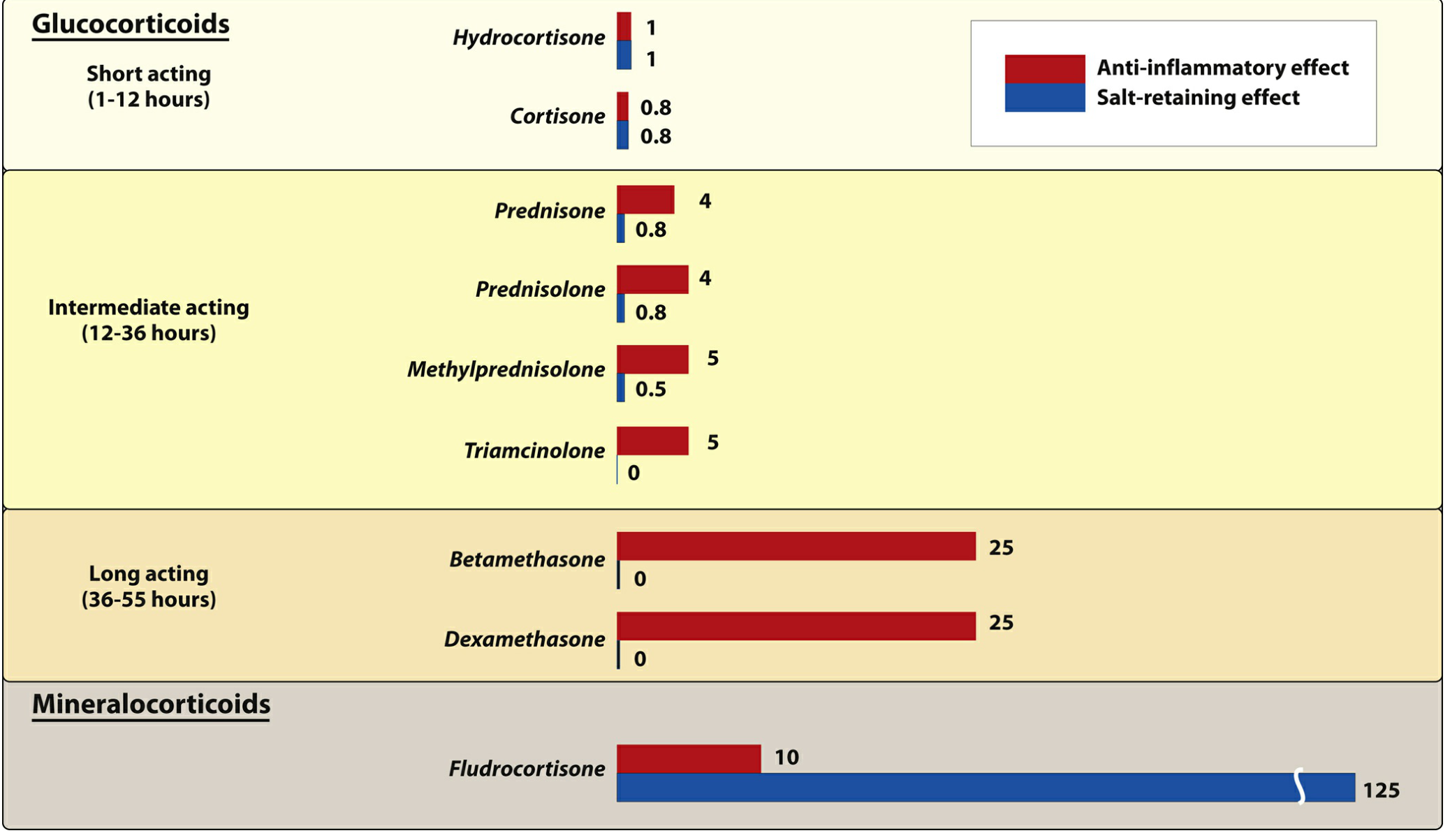
Short-acting (t½ 8-12 hours, biological activity 1-12 hours):
- Hydrocortisone (cortisol) - anti-inflammatory potency = 1 (reference), salt-retaining = 1, equivalent dose = 20 mg
- Cortisone - anti-inflammatory potency = 0.8, salt-retaining = 0.8, equivalent dose = 25 mg
Intermediate-acting (biological activity 12-36 hours):
- Prednisone - potency = 4, minimal salt-retaining = 0.3, equivalent dose = 5 mg
- Prednisolone - potency = 5, salt-retaining = 0.3, equivalent dose = 5 mg
- Methylprednisolone - potency = 5, salt-retaining = 0.25, equivalent dose = 4 mg
- Triamcinolone - potency = 5, salt-retaining = 0, equivalent dose = 4 mg
Long-acting (biological activity 36-55 hours):
- Betamethasone - potency = 25, no salt retention (0)
- Dexamethasone - potency = 25, no salt retention (0)
Mineralocorticoids:
- Fludrocortisone - anti-inflammatory = 10, salt-retaining = 125 (very potent)
C. Based on Route of Administration
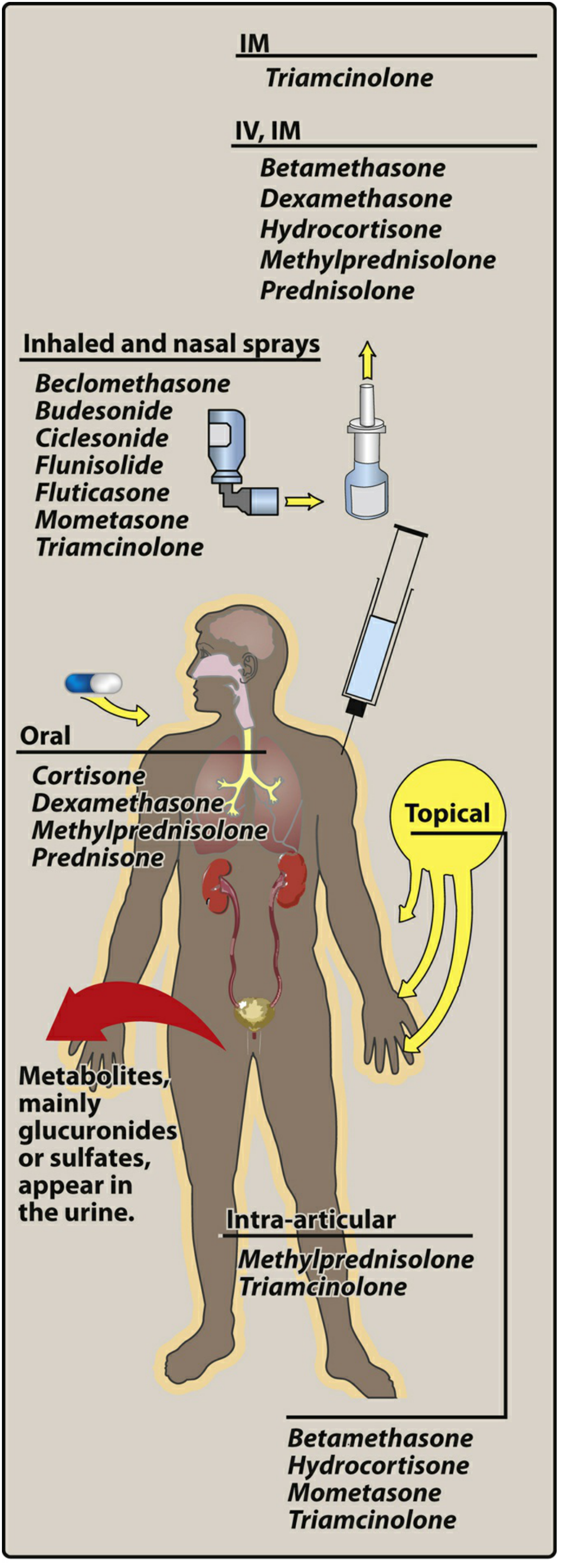
- Oral: Cortisone, prednisone, dexamethasone, methylprednisolone
- Parenteral (IV/IM): Hydrocortisone, methylprednisolone, betamethasone, dexamethasone, prednisolone
- Inhaled/Nasal sprays: Beclomethasone, budesonide, fluticasone, flunisolide, mometasone, ciclesonide
- Topical: Hydrocortisone, betamethasone, clobetasol, mometasone (creams, ointments)
- Intra-articular: Methylprednisolone, triamcinolone
3. Mechanism of Action
Corticosteroids work through an intracellular receptor mechanism (genomic mechanism):
- The steroid crosses the cell membrane (being lipid soluble) and binds to specific cytoplasmic receptors - glucocorticoid receptors (GR) widely distributed throughout the body, and mineralocorticoid receptors (MR) confined mainly to excretory organs (kidney, colon, salivary glands, sweat glands)
- The hormone-receptor complex dimerizes, recruits coactivator or corepressor proteins, and translocates to the nucleus
- It binds to glucocorticoid response elements (GRE) in gene promoter regions, acting as a transcription factor to turn genes on or off depending on tissue context
- This results in altered protein synthesis - because of this mechanism, effects take hours to days to manifest
Key anti-inflammatory mechanisms:
- Enhance production of lipocortin (annexin-1), which inhibits phospholipase A2, thereby blocking release of arachidonic acid (precursor of prostaglandins and leukotrienes)
- Decrease production and release of pro-inflammatory cytokines (IL-1, IL-2, IL-6, TNF-alpha)
- Stabilize mast cell and basophil membranes, reducing histamine release
- Reduce circulating lymphocytes, eosinophils, basophils, and monocytes by redistributing them to lymphoid tissue
4. Pharmacological Actions / Uses
I. Physiological (Replacement) Uses
1. Primary Adrenal Insufficiency (Addison's Disease)
- Caused by dysfunction of the adrenal cortex (diagnosed by lack of response to ACTH)
- Hydrocortisone (identical to natural cortisol) is the drug of choice for replacement
- Two-thirds of the daily dose is given in the morning and one-third in the afternoon to mimic normal diurnal variation
- Fludrocortisone is added to correct mineralocorticoid deficiency
- Failure to treat results in death (adrenal crisis)
2. Secondary Adrenal Insufficiency
- Usually due to pituitary or hypothalamic disease
- Glucocorticoid replacement (hydrocortisone, prednisone) required; mineralocorticoid supplementation usually not needed
3. Congenital Adrenal Hyperplasia (CAH)
- Due to enzyme defect in adrenal steroid synthesis, leading to androgen excess
- Corticosteroids are used to suppress ACTH and normalize adrenal androgen production
- Drug choice depends on the specific enzyme defect
II. Therapeutic (Pharmacological) Uses
4. Inflammatory and Autoimmune Disorders
- Rheumatoid arthritis, SLE, polymyositis, giant cell arteritis, scleroderma, mixed connective tissue disease, temporal arteritis
- Used to reduce inflammation and suppress immune responses
- Note: corticosteroids are not curative in these conditions
5. Allergic Conditions
- Anaphylaxis, angioedema, drug reactions, serum sickness, urticaria, contact dermatitis, bee stings, severe allergic rhinitis
- IV hydrocortisone or methylprednisolone used in acute severe reactions
6. Asthma
- Inhaled corticosteroids (ICS: beclomethasone, budesonide, fluticasone) are the cornerstone of persistent asthma management - provide long-term symptom control with minimal systemic effects
- Oral/IV corticosteroids used in acute severe exacerbations
7. Skin Diseases
- Atopic dermatitis, psoriasis, pemphigus, lichen planus, contact dermatitis, seborrheic dermatitis, mycosis fungoides
- Topical preparations of varying potency used
8. Gastrointestinal Diseases
- Inflammatory bowel disease (Crohn's disease, ulcerative colitis)
- Subacute hepatic necrosis, nontropical sprue
9. Eye Diseases
- Acute uveitis, allergic conjunctivitis, choroiditis, optic neuritis
10. Hematologic Disorders
- Idiopathic thrombocytopenic purpura (ITP), autoimmune hemolytic anemia, leukemia, lymphoma, multiple myeloma
11. Renal Diseases
- Nephrotic syndrome (minimal change disease responds well to prednisolone)
12. Neurological Disorders
- Cerebral edema: large doses of dexamethasone after brain surgery or head injury
- Multiple sclerosis acute exacerbations
13. Organ Transplantation
- Prevention and treatment of rejection (used as part of immunosuppressive regimens)
14. Pulmonary Uses
- Acceleration of fetal lung maturation: Betamethasone given to mothers with threatened preterm delivery stimulates surfactant production, preventing neonatal respiratory distress syndrome (RDS)
- Aspiration pneumonia, sarcoidosis
15. Malignancies
- Lymphoma, leukemia (as part of chemotherapy protocols, e.g., CHOP regimen)
- Dexamethasone used as antiemetic in chemotherapy
16. Septic Shock / ARDS
- Low-dose corticosteroids (e.g., hydrocortisone) used in vasopressor-refractory septic shock
- COVID-19 severe/critical illness: dexamethasone shown to reduce mortality
17. Diagnostic Use
- Dexamethasone suppression test (DST): Diagnosing Cushing syndrome
- Low-dose DST: 1 mg dexamethasone given at midnight; serum cortisol measured at 8 AM - normal individuals show suppression
- High-dose DST: Differentiates Cushing disease from adrenal tumor/ectopic ACTH
5. Adverse Effects
Adverse effects are generally dose-dependent and more common with long-term systemic therapy:
A. Metabolic Effects (Cushing-Like Syndrome)
- Hyperglycemia / Steroid-induced diabetes - due to increased gluconeogenesis and insulin resistance
- Hyperlipidemia
- Central obesity, moon facies (round, plethoric face)
- Buffalo hump (fat pad at back of neck/upper back)
- Truncal obesity with thin limbs
- Hypokalemic alkalosis (especially with mineralocorticoid activity)
- Sodium and water retention - leading to edema, hypertension
B. Musculoskeletal Effects
- Osteoporosis - due to decreased bone formation and increased resorption (most serious long-term effect)
- Avascular necrosis (osteonecrosis) of femoral head - important and often overlooked
- Proximal myopathy / muscle wasting - weakness of proximal limb muscles
- Growth retardation in children
C. Skin and Connective Tissue
- Skin thinning (dermal atrophy)
- Purple/red striae (stretch marks due to protein loss)
- Easy bruising (ecchymoses)
- Poor wound healing - due to impaired collagen synthesis
- Hirsutism
- Acne
D. Immunological / Increased Susceptibility to Infection
- Increased risk of infections - bacterial, fungal (Candida, Aspergillus), viral (reactivation of TB, Herpes zoster), opportunistic infections (Pneumocystis jirovecii pneumonia)
- Reactivation of latent tuberculosis - always perform tuberculin test and chest X-ray before starting prolonged therapy
- Impaired wound healing
E. Endocrine Effects
- HPA axis suppression - the most important effect with prolonged use; ACTH secretion is suppressed, leading to adrenal atrophy
- Adrenal insufficiency on abrupt withdrawal - hence gradual tapering is mandatory
- Menstrual irregularities
- Impotence
F. Cardiovascular Effects
- Hypertension (due to sodium retention and renin-angiotensin activation)
- Atherosclerosis with long-term use
- Increased risk of thromboembolism
G. Gastrointestinal Effects
- Peptic ulcer - controversial but increased risk, especially in combination with NSAIDs
- Gastritis, gastrointestinal bleeding
- Pancreatitis (rare)
H. Ocular Effects
- Posterior subcapsular cataracts - with prolonged use
- Increased intraocular pressure (glaucoma)
I. CNS/Psychiatric Effects
- Euphoria - common initially; may progress to frank psychosis
- Insomnia, mood swings, behavioral changes
- Depression on withdrawal
- Benign intracranial hypertension (pseudotumor cerebri) - especially in children on withdrawal
J. Withdrawal Syndrome
If corticosteroids are stopped abruptly after prolonged use:
- Nausea, vomiting, fever, joint pain (arthralgia)
- Hypotension, hypoglycemia
- Acute adrenal crisis (life-threatening)
- The underlying disease may flare (rebound phenomenon)
Therefore, always taper the dose gradually when discontinuing prolonged corticosteroid therapy.
6. Contraindications
Absolute Contraindications
- Systemic fungal infections (unless used as replacement therapy)
- Hypersensitivity to the specific corticosteroid preparation
Relative Contraindications (Use with Great Caution)
- Peptic ulcer disease - risk of perforation/bleeding (use PPI cover if unavoidable)
- Active tuberculosis or other serious infections (varicella, herpes, candidiasis) - corticosteroids may worsen these; treat infection simultaneously if corticosteroids are unavoidable
- Uncontrolled diabetes mellitus - will worsen hyperglycemia
- Hypertension with heart failure - sodium retention and fluid retention worsen cardiovascular status
- Psychiatric disorders (psychoses) - can precipitate or worsen psychiatric illness
- Osteoporosis - will accelerate bone loss
- Glaucoma - will increase intraocular pressure
- Pregnancy - risk of fetal adrenal suppression, cleft palate (first trimester); however, life-threatening maternal conditions override this
- Live vaccines - avoid in immunosuppressed patients on high-dose corticosteroids (e.g., BCG, MMR, oral polio)
- Myasthenia gravis - may worsen initially (but is also used to treat it long term)
- Congestive heart failure - sodium retention worsens fluid overload
Special Precautions
Patients receiving glucocorticoids must be regularly monitored for:
- Hyperglycemia and glycosuria
- Sodium retention with edema or hypertension
- Hypokalemia
- Peptic ulcer
- Osteoporosis
- Hidden/occult infections (including TB reactivation)
Stress dosing: Even patients on relatively low-dose corticosteroids may need supplementary (stress) doses during surgical procedures, intercurrent illnesses, or accidents, due to blunted HPA axis response.
Summary Table
| Feature | Glucocorticoids | Mineralocorticoids |
|---|---|---|
| Prototype | Hydrocortisone | Aldosterone / Fludrocortisone |
| Receptor | Glucocorticoid receptor (GR) | Mineralocorticoid receptor (MR) |
| Main action | Anti-inflammatory, metabolic | Na+ retention, K+ excretion |
| Endogenous source | Zona fasciculata | Zona glomerulosa |
| Key therapeutic use | Inflammation, immunosuppression | Addison's disease (replacement) |
| Major ADR | Cushing syndrome, infections, osteoporosis | Hypertension, hypokalemia |
Note on reference: Padma Udaykumar's Pharmacology (CBS Publishers) is the standard Indian medical pharmacology textbook widely used for MBBS. While that specific title is not in the digital library, the above content follows her textbook's classification framework precisely (short/intermediate/long-acting glucocorticoids; glucocorticoid vs mineralocorticoid; uses in adrenal and non-adrenal disorders; adverse effects and contraindications as taught in Indian pharmacology curricula). Content is cross-referenced from Katzung's Basic and Clinical Pharmacology, 16e and Lippincott Illustrated Reviews: Pharmacology.
Glaucoma
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a complete, detailed answer. Let me compile the full overview:
GLAUCOMA - Complete Overview
References: Kanski's Clinical Ophthalmology 10e, Robbins & Kumar Basic Pathology, Goodman & Gilman's Pharmacological Basis of Therapeutics, Katzung's Basic & Clinical Pharmacology 16e (aligned with Padma Udaykumar Pharmacology framework)
1. Definition
Glaucoma is a term used to describe a group of conditions that share a common pathway of chronic progressive optic neuropathy, resulting in:
- Characteristic morphological changes at the optic nerve head (optic disc cupping)
- Retinal nerve fibre layer (RNFL) thinning
- Retinal ganglion cell death
- Progressive visual field loss
Intraocular pressure (IOP) is the key modifiable risk factor. Normal IOP is 10-21 mmHg. However, glaucoma can occur with normal IOP (normal-tension glaucoma), and some individuals tolerate elevated IOP without developing damage (ocular hypertension).
"Glaucoma is the second leading cause of blindness in the world." - Kanski's Clinical Ophthalmology 10e
2. Aqueous Humor Dynamics (Pathophysiology Basis)
Understanding glaucoma requires understanding how IOP is regulated:
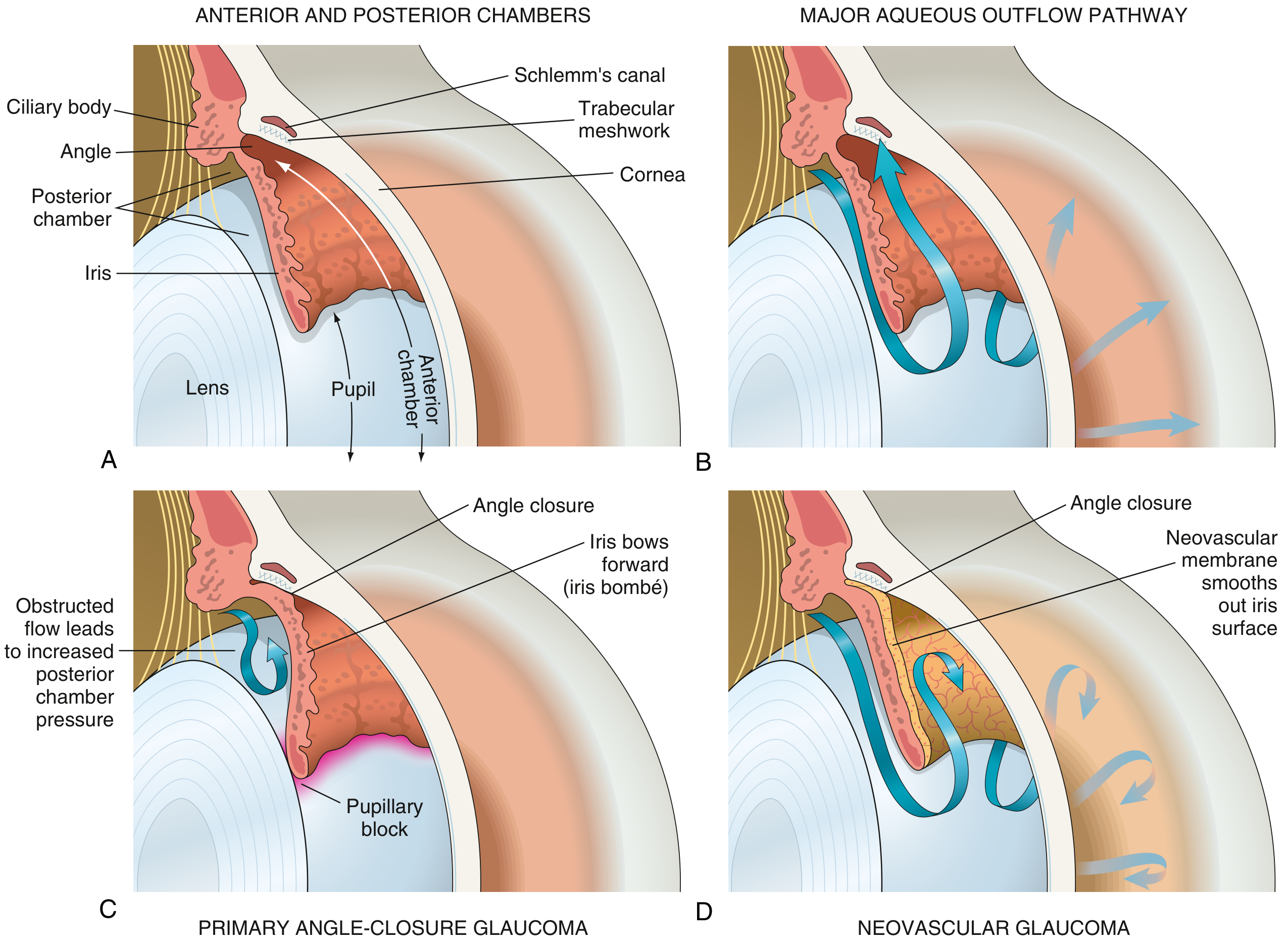
Fig. A: Normal eye anatomy. B: Normal aqueous outflow through trabecular meshwork → Schlemm's canal. C: Primary angle-closure glaucoma with iris bombé. D: Neovascular glaucoma with membrane occluding angle.
- Aqueous humor is produced by the ciliary body (posterior chamber)
- Flows through the pupil into the anterior chamber
- Drains primarily through the trabecular meshwork → Schlemm's canal → episcleral veins (conventional/trabecular route, ~75-80%)
- Secondary drainage via uveoscleral route (~20-25%)
- IOP is elevated when:
- Outflow is obstructed (most common cause), OR
- Aqueous production is increased (rare)
3. Classification
A. Based on Anatomy of the Anterior Chamber Angle
| Type | Mechanism | Notes |
|---|---|---|
| Open-angle glaucoma | Trabecular meshwork or downstream obstruction with open angle | Most common in Caucasians and Africans |
| Angle-closure glaucoma | Iris physically occludes the trabecular meshwork | Common in Asians |
B. Based on Etiology
I. PRIMARY GLAUCOMA (no identifiable ocular/systemic cause)
1. Primary Open-Angle Glaucoma (POAG)
- Most common type worldwide in Whites, Hispanics, and Black individuals
- Chronic, insidious, bilateral (often asymmetric)
- IOP typically >21 mmHg
- Open anterior chamber angle
- No identifiable secondary cause
2. Normal-Tension Glaucoma (NTG)
- Also called low-tension or normal-pressure glaucoma
- IOP consistently ≤ 21 mmHg
- All other features of glaucomatous optic neuropathy are present
- More common in Japanese people and women
- Vascular insufficiency plays a greater role
- Associated with: migraine, Raynaud phenomenon, nocturnal hypotension
3. Primary Angle-Closure Glaucoma (PACG)
- Iris occludes trabecular meshwork (iridotrabecular contact - ITC)
- Particularly common in Asians; constitutes up to half of all cases globally
- Progresses rapidly, more likely to cause visual loss than POAG
- Mechanism: Relative pupillary block → pressure differential between posterior and anterior chambers → iris bows forward (iris bombé) → angle closure
4. Primary Congenital / Developmental Glaucoma
- Present at birth or early childhood
- Due to maldevelopment of the drainage angle (trabeculodysgenesis)
- Signs: buphthalmos (enlarged eye), corneal clouding, photophobia, epiphora
II. SECONDARY GLAUCOMA (identifiable cause)
Open-angle types:
- Pre-trabecular: Membrane covers trabeculum - neovascular glaucoma (fibrovascular), iridocorneal endothelial (ICE) syndrome
- Trabecular clogging:
- Pigmentary glaucoma (pigment particles)
- Pseudoexfoliation glaucoma (exfoliative material)
- Ghost cell glaucoma (degenerated red cells)
- Phacolytic glaucoma (lens proteins + macrophages)
- Post-traumatic (angle recession)
- Post-trabecular: Elevated episcleral venous pressure - Sturge-Weber syndrome, carotid-cavernous fistula
- Steroid-induced glaucoma - corticosteroids (topical or systemic) increase IOP
Angle-closure types:
- With pupillary block: seclusio pupillae (360° posterior synechiae), subluxated lens, phacomorphic glaucoma
- Without pupillary block: neovascular glaucoma (advanced), cilio-choroidal effusion
4. Risk Factors
For POAG:
- Elevated IOP (most important modifiable factor)
- Increasing age (>40 years)
- Black race (4x higher risk, earlier onset, harder to control)
- Positive family history (first-degree relatives: 4x risk to siblings, 2x to offspring)
- Myopia
- Thin central corneal thickness (CCT)
- Low ocular perfusion pressure
- Anti-VEGF therapy (recurrent intravitreal injections)
- Systemic calcium-channel blockers
For PACG:
- Hypermetropia (small eye, shallow anterior chamber)
- Female sex
- Asian ethnicity
- Advancing age (lens thickens)
- Family history
5. Clinical Features
POAG (Chronic, Insidious)
- Usually asymptomatic until late stages (peripheral field loss goes unnoticed)
- Visual acuity is normal until advanced disease
- Slow, progressive, bilateral field loss
- No pain, no redness
- Detected on routine eye examination
Acute Angle-Closure Glaucoma (AACG) - Medical Emergency
- Sudden onset of severe eye pain
- Headache (often frontal, may be accompanied by nausea, vomiting)
- Blurred vision
- Coloured halos around lights (corneal oedema)
- Red eye (ciliary congestion)
- Mid-dilated, fixed, oval pupil
- Rock-hard eyeball on palpation
- Cornea: steamy/hazy (oedematous)
- Shallow anterior chamber
- IOP: markedly elevated (often 40-70 mmHg)
- Precipitated by: dim lighting, stress, drugs (anticholinergics, sympathomimetics)
NTG
- Similar to POAG but IOP is normal
- Visual field defects tend to be deeper and closer to fixation
- More paracentral scotomas
6. Examination and Investigations
A. Tonometry (IOP Measurement)
- Goldmann applanation tonometry - gold standard
- Normal IOP: 10-21 mmHg (mean ~15 mmHg)
- Must correlate with central corneal thickness (CCT): thick cornea overestimates, thin cornea underestimates IOP
B. Gonioscopy
- Essential for distinguishing open-angle from angle-closure
- Shaffer grading system (0-4):
- Grade 4 (35-45°): Wide open, myopia
- Grade 3 (25-35°): Open, scleral spur visible
- Grade 2 (20°): Trabeculum visible, no scleral spur
- Grade 1 (10°): Very narrow, Schwalbe line only
- Grade 0 (0°): Closed - iridocorneal contact
- Grade ≤2 should undergo gonioscopy; Grade 1 = dangerously narrow
C. Optic Disc Examination (Dilated Fundoscopy)
- Neuroretinal rim (NRR): ISNT rule - Inferior > Superior > Nasal > Temporal (normal pattern)
- Cup/Disc (C/D) ratio:
- Vertical C/D >0.7 suspicious (only 2% of population)
- Asymmetry of C/D ≥0.2 between eyes is significant
- Glaucomatous disc changes:
- Disc haemorrhage (splinter haemorrhage at disc margin - important sign)
- Focal notching of the NRR
- RNFL defects (wedge-shaped, visible in red-free light)
- Bayonetting of vessels
- Nasal shift of vessels
- Increased cup size
D. Perimetry (Visual Field Testing)
-
Standard Automated Perimetry (SAP) - Humphrey visual field analyzer
-
Patterns: 24-2 (routine), 10-2 (central field monitoring in advanced glaucoma)
-
Glaucomatous field defects (in order of progression):
- Increased variability and slight asymmetry (early)
- Paracentral scotomas (small depressions, often superonasally)
- Nasal step (difference above and below horizontal midline nasally)
- Temporal wedge (less common)
- Arcuate scotoma (Bjerrum scotoma) - sweeps from blind spot around fixation
- Ring scotoma - superior and inferior arcuates join
- End stage - small central and temporal island only
-
Criteria for significant glaucomatous damage (Hodapp-Parrish-Anderson):
- Glaucoma Hemifield Test (GHT) outside normal limits on 2 consecutive occasions
- Cluster of ≥3 non-edge points depressed at P<5%, one at P<1%
- Corrected Pattern Standard Deviation (CPSD) <5%
E. Imaging
- Optical Coherence Tomography (OCT): RNFL thickness, ganglion cell analysis - gold standard for structural assessment
- Heidelberg Retinal Tomography (HRT): Optic nerve head topography
- Scanning Laser Polarimetry (GDx VCC)
F. Central Corneal Thickness (CCT)
- Measured by pachymetry
- Influences IOP measurement accuracy
- Thin CCT is an independent risk factor for POAG progression
7. Treatment
Goal of Treatment
To slow/halt progression of optic nerve damage and maintain visual function throughout the patient's lifetime. Treatment is based on achieving a target IOP - typically reducing baseline IOP by at least 20-30%.
A reasonable initial target is IOP <18 mmHg (AGIS trial data).
A. Medical Treatment (Drug Therapy)
(Padma Udaykumar framework: drugs classified by mechanism)
1. Prostaglandin Analogues - FIRST-LINE
Drugs: Latanoprost, bimatoprost, travoprost, tafluprost, unoprostone
Mechanism: Increase uveoscleral outflow (and some trabecular outflow) by acting on FP receptors in ciliary muscle and trabecular meshwork
Dose: Once daily (evening), as eye drops
IOP reduction: 25-35% (most potent class)
Adverse effects:
- Iris pigmentation - irreversible brown pigmentation (melanin deposition)
- Eyelash changes - increased length, thickness, darkening (bimatoprost used for lash hypotrichosis)
- Periorbital fat atrophy (prostaglandin-associated periorbitopathy)
- Conjunctival hyperemia
- Drying of eyes, conjunctivitis
- Reactivation of herpetic keratitis (contraindication)
Contraindications: Active ocular inflammation, herpes simplex keratitis, pregnancy
2. Beta-Adrenoceptor Blockers
Drugs: Timolol (most widely used), betaxolol, levobunolol, carteolol
Mechanism: Reduce aqueous humor production by blocking β-receptors on ciliary epithelium
Dose: Timolol 0.25% or 0.5% twice daily; once daily for long-acting formulations
IOP reduction: 20-30%
Adverse effects (systemic - most important):
- Bronchoconstriction (risk of fatal bronchospasm in asthmatics)
- Bradycardia, heart block (cardiac conduction disturbances)
- Hypotension
- Masking of hypoglycemia symptoms in diabetics
- Depression, fatigue, impotence
- Betaxolol (β1-selective) has less pulmonary risk
Contraindications: Asthma, COPD, heart failure, heart block (2nd/3rd degree), bradycardia, peripheral vascular disease
3. Alpha-2 Adrenoceptor Agonists
Drugs: Brimonidine (selective α2-agonist), apraclonidine
Mechanism: Dual action:
- Decrease aqueous production (α2 receptors on ciliary body)
- Increase uveoscleral outflow
IOP reduction: 20-25%
Adverse effects:
- Dry mouth, dry nose
- Allergic conjunctivitis (brimonidine - common)
- CNS sedation (brimonidine crosses blood-brain barrier)
- Apraclonidine: tachyphylaxis (loss of effect over time)
Contraindications: Infants and young children (CNS depression, apnea), MAO inhibitor use
4. Carbonic Anhydrase Inhibitors (CAIs)
Drugs:
- Systemic: Acetazolamide (oral/IV), methazolamide (oral)
- Topical: Dorzolamide, brinzolamide (eye drops)
Mechanism: Inhibit carbonic anhydrase (primarily CA-II isoenzyme) in ciliary body → reduce bicarbonate and aqueous humor production
IOP reduction: 15-26%
Adverse effects - Systemic acetazolamide (most important):
- Hypokalemia, metabolic acidosis
- Renal stones (nephrolithiasis)
- Paraesthesias (tingling in fingers/toes - very common)
- Malaise, fatigue, anorexia, nausea
- Aplastic anemia, agranulocytosis (rare but serious)
- Contraindicated with sulfonamide allergy (sulfonamide derivative)
Topical CAIs (dorzolamide, brinzolamide): Minimal systemic effects; local stinging, metallic taste, conjunctivitis
Systemic use: Reserved for acute angle-closure crisis (IV acetazolamide) or adjunct when topical therapy inadequate
5. Cholinergic Agonists (Miotics)
Drugs: Pilocarpine (most important), carbachol, echothiophate (long-acting, anticholinesterase)
Mechanism: Act on muscarinic receptors in ciliary muscle and iris sphincter → contraction of ciliary muscle → opens trabecular meshwork spaces → increases conventional outflow
Dose: Pilocarpine 1-4% eye drops 3-4 times daily
IOP reduction: 20-25%
Adverse effects:
- Miosis - difficulty in dim light, darkening of vision
- Brow ache (ciliary muscle spasm)
- Myopia (ciliary spasm)
- Retinal detachment risk (especially in myopes) - perform prophylactic retinal check
- Accommodation spasm (especially in young patients)
- Sweating, increased salivation (if systemic absorption)
Current use: Largely superseded by prostaglandins and beta-blockers; still used in angle-closure crisis
6. Sympathomimetics
Drugs: Dipivefrine (prodrug of epinephrine), adrenaline
Mechanism: Increase uveoscleral outflow, may reduce aqueous production
Adverse effects: Ocular hyperemia, allergy; cardiac effects (palpitations, hypertension); macular edema in aphakic patients
Largely obsolete - replaced by newer classes
7. Rho Kinase (ROCK) Inhibitors - Newer Class
Drug: Netarsudil
Mechanism: Increase trabecular outflow by relaxing trabecular meshwork cells; also reduce episcleral venous pressure
Adverse effects: Conjunctival hyperemia (very common), cornea verticillata
8. Osmotic Agents (for Acute Angle-Closure)
Drugs: Glycerol (oral), mannitol (IV 20%)
Mechanism: Increase plasma osmolarity → draw fluid from vitreous → rapidly reduce IOP
Use: Acute angle-closure crisis when IOP is very high (>40 mmHg)
Adverse effects: Dehydration, headache, nausea; mannitol causes expansion of plasma volume (caution in heart failure)
B. Laser Treatment
1. Laser Peripheral Iridotomy (LPI) / Nd:YAG Iridotomy
- Indication: Primary angle closure and PACG
- Mechanism: Creates a hole in peripheral iris → equalizes pressure between anterior and posterior chambers → relieves pupillary block → angle opens
- First-line definitive treatment for PACG
- Also performed prophylactically in fellow eye
2. Laser Trabeculoplasty
- Argon Laser Trabeculoplasty (ALT) - older technique
- Selective Laser Trabeculoplasty (SLT) - preferred; selectively targets pigmented trabecular cells
- Indication: POAG not controlled on medications, or as alternative/adjunct to medications
- Mechanism: Stimulates trabecular meshwork cells → improves drainage
- Can be repeated (SLT is repeatable); effect may wane over years
3. Diode Laser Cycloablation (Cyclophotocoagulation)
- Destroys ciliary body → reduces aqueous production
- Reserved for advanced or refractory glaucoma
C. Surgical Treatment
1. Trabeculectomy (Filtration Surgery)
- Most common glaucoma operation (gold standard)
- Creates a fistula (guarded bleb) between anterior chamber and subconjunctival space
- Mitomycin C (MMC) or 5-fluorouracil (5-FU) used adjunctively to prevent scarring
- Complications: bleb failure, bleb leak, hypotony, infection (blebitis, endophthalmitis), cataract
2. Glaucoma Drainage Devices (Tube Shunts)
- E.g., Ahmed, Baerveldt, Molteno tubes
- Silicone tube drains aqueous into a plate in subconjunctival space
- Used when trabeculectomy has failed or is likely to fail (uveitic, neovascular, previously operated eyes)
- Offer best chance of long-term IOP control in complex glaucomas
3. Minimally Invasive Glaucoma Surgery (MIGS)
- iStent, Hydrus microstent, OMNI, goniotomy
- Ab interno procedures through the trabecular meshwork
- Lower IOP reduction than trabeculectomy but safer profile
- Often combined with cataract surgery
4. Combined Trabeculotomy-Trabeculectomy
- Used in primary congenital and developmental glaucoma
- Goniotomy also used in congenital cases
5. Clear Lens Extraction
- Phacoemulsification with IOL implantation more cost-effective than LPI in PAC patients with IOP >29 mmHg or established PACG
8. Management of Acute Angle-Closure Crisis (Emergency)
This is a medical emergency requiring immediate treatment:
-
Immediate IOP lowering:
- IV acetazolamide 500 mg (or oral if not vomiting)
- IV mannitol 20% (1-2 g/kg) if IOP very high
- Topical timolol 0.5% (beta-blocker)
- Topical brimonidine 0.2%
- Topical apraclonidine 1%
-
Topical steroids: To reduce inflammation
-
Pilocarpine 1-2%: Applied to both eyes once IOP is below 40 mmHg (ciliary sphincter is ischemic and unresponsive at higher pressures)
-
Definitive treatment: Laser peripheral iridotomy once attack is broken and cornea is clear
-
Prophylactic LPI to the fellow eye (risk of fellow eye developing acute attack is ~50% within 5 years if untreated)
9. Steroid-Induced Glaucoma (Special Note - Padma Udaykumar Connection)
As relevant from the previous corticosteroids discussion:
- Topical, periocular, inhaled, or systemic steroids can cause IOP elevation in susceptible individuals ("steroid responders")
- Mechanism: glucocorticoids alter trabecular meshwork cell morphology and reduce aqueous outflow
- Onset: weeks to months after starting steroids
- Usually reversible on discontinuing the steroid
- If not recognized, can lead to permanent glaucomatous damage
- Management: stop steroid if possible, add IOP-lowering drops, consider surgical intervention
10. Summary
| Feature | POAG | PACG (Acute) | NTG |
|---|---|---|---|
| Onset | Insidious | Sudden | Insidious |
| IOP | Elevated (usually) | Very high (40-70) | Normal (≤21) |
| Angle | Open | Closed | Open |
| Pain | Absent | Severe | Absent |
| Cornea | Clear | Hazy/steamy | Clear |
| Pupil | Normal | Mid-dilated, fixed | Normal |
| Visual field | Peripheral loss | Peripheral loss | Often deeper, paracentral |
| First-line Rx | Prostaglandin analogue or beta-blocker | IV acetazolamide + pilocarpine + mannitol | Reduce IOP (even if normal) |
| Definitive Rx | Medical/SLT/trabeculectomy | Laser peripheral iridotomy | Reduce IOP, neuroprotection |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach 10e, pp. 364-396 | Robbins & Kumar Basic Pathology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic & Clinical Pharmacology 16e
This is a shared conversation. Sign in to Orris to start your own chat.