Explain Diphtheria in infective epidemiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough answer. Let me compile the full response.
Diphtheria - Infective Epidemiology
Definition
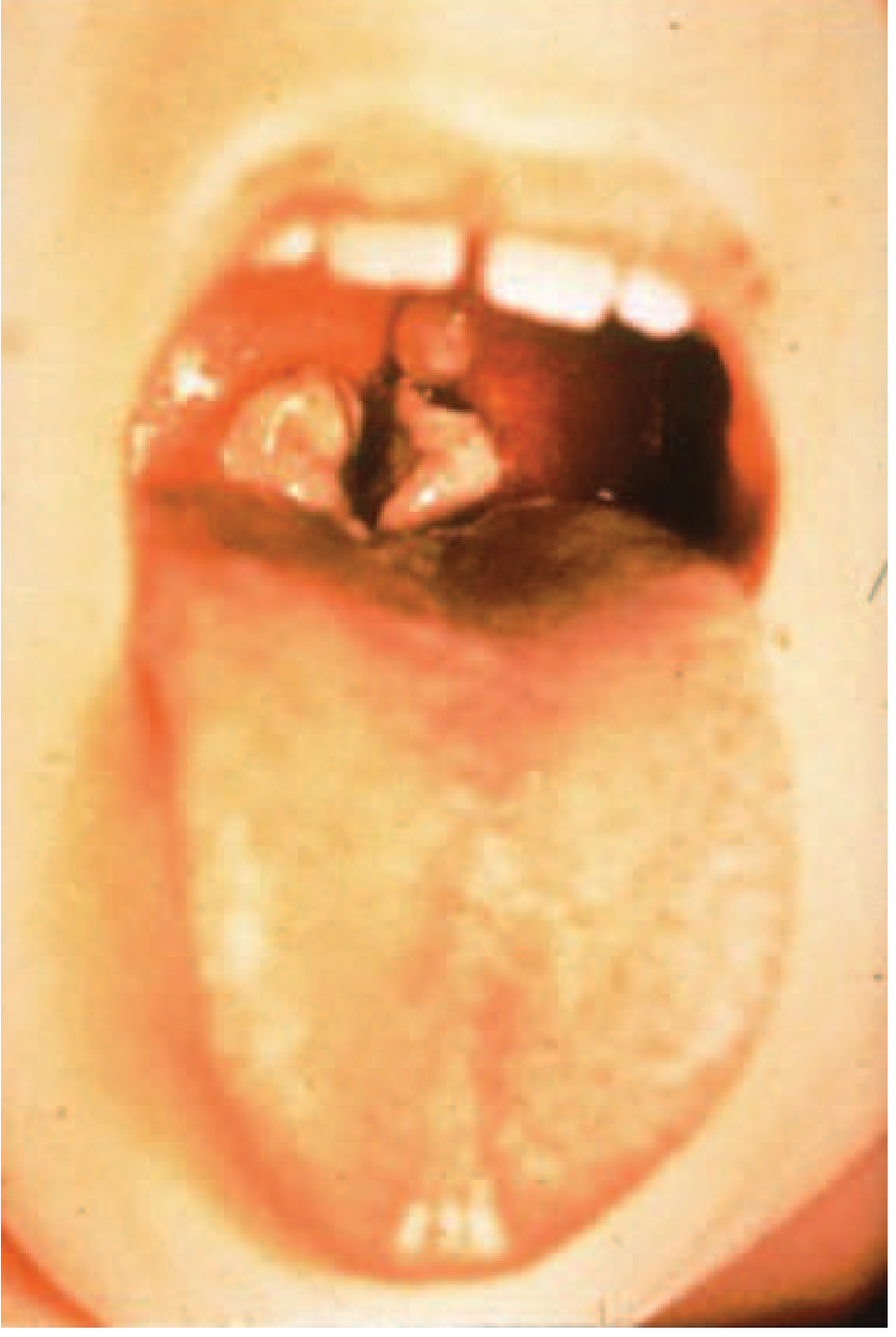
Diphtheria is an acute bacterial infectious disease caused by toxigenic strains of Corynebacterium diphtheriae. The bacilli multiply locally - usually in the throat - and elaborate a powerful exotoxin responsible for pseudomembrane formation, local tissue destruction, and systemic toxicity (myocarditis, polyneuropathy). Case fatality is 5-10% on average, rising to ~20% in children under 5 and adults over 40 in untreated cases.
Epidemiological Determinants
1. Agent Factors
| Property | Detail |
|---|---|
| Organism | C. diphtheriae - gram-positive, non-motile, non-spore-forming, pleomorphic bacillus |
| Biotypes | Gravis, mitis, intermedius, belfanti - all pathogenic; gravis causes more severe disease |
| Toxigenicity | Not all strains are toxigenic. A non-toxigenic strain becomes toxigenic when lysogenized by corynebacteriophage beta (beta-phage), which carries the structural tox gene |
| Toxin mechanism | ADP-ribosylase toxin - inhibits protein synthesis (EF-2 inactivation) in all cells, especially myocardial, renal, and peripheral nerve cells |
| Viability | Killed readily by heat and chemical agents; may survive for short periods in dust and fomites |
| Iron regulation | Toxin expression is optimized under iron-limiting conditions during infection |
Related species: Corynebacterium ulcerans and C. pseudotuberculosis can express the same toxin and cause diphtheria-like illness.
2. Source of Infection
(a) Cases:
- Ranges from subclinical to overt clinical illness
- Mild or silent cases (inapparent infection) play a more important epidemiological role than frank clinical cases because they are undetected yet shed organisms
(b) Carriers:
- Very important source; carrier types include:
- Nasal carriers - more dangerous because of frequent and copious shedding into the environment
- Throat carriers - less dangerous
- Temporary carriers - last ~1 month
- Chronic carriers - persist for a year or more if untreated
- Immunization does NOT prevent the carrier state - this is an important epidemiological implication
3. Reservoir
Humans are the sole reservoir of C. diphtheriae. There are no significant animal or environmental reservoirs.
4. Mode of Transmission
| Route | Details |
|---|---|
| Droplet/aerosol (primary) | Respiratory droplets during close contact with a case or carrier - this is the predominant route |
| Direct contact | Contact with discharges from cutaneous diphtheria lesions |
| Indirect/fomites | Cups, thermometers, toys, pencils contaminated with nasopharyngeal secretions - possible but only for short periods |
| Contaminated milk | Rare vehicle of transmission (historically documented) |
| Travelers | People traveling to or from endemic areas are at increased risk |
5. Infective Material
- Nasopharyngeal secretions
- Discharges from skin lesions
- Contaminated fomites
- Infected dust (limited survival)
6. Period of Infectivity / Incubation
| Parameter | Value |
|---|---|
| Incubation period | Usually 2-5 days (range 1-10 days); mean ~1.4 days for respiratory diphtheria |
| Period of communicability | 14-28 days from onset if untreated; chronic carriers may be infective for months to a year |
| After treatment | Patients on appropriate antibiotics are usually non-infectious within 48 hours |
| Termination of isolation | At least 2 consecutive negative cultures from nose and throat, 24 hours apart |
| R0 (basic reproduction number) | 1.7-4.3 for respiratory diphtheria |
7. Host Factors
(a) Age:
- Primarily affects children aged 1-5 years in unvaccinated populations
- With widespread immunization, a shift in age incidence is observed from preschool children to older children and adults (waning immunity in adults)
- Infants born of immune mothers are protected by maternal IgG antibodies for the first few weeks to months of life, then become susceptible after ~6 months
(b) Sex: Both sexes are equally affected.
(c) Immunity:
- Resistance depends on the presence of specific neutralizing antitoxin in the bloodstream
- Protective threshold: serum antitoxin ≥ 0.01 IU/mL (Lf unit/mL)
- Before vaccination, natural immunity was acquired through inapparent skin infections with C. diphtheriae - by age 6-8 years, ~75% of children in tropical/developing countries had protective antitoxin levels
- Vaccine-induced immunity wanes over time; adults in developed countries may lose protection
8. Environmental Factors
- Cases occur year-round
- Winter months favor spread in temperate regions (indoor crowding, droplet transmission)
- Summer epidemics can occur in warm climates where cutaneous diphtheria is prevalent
- Overcrowded living conditions and poor socioeconomic status increase risk
Cutaneous vs. Respiratory Diphtheria (Epidemiological Distinction)
| Feature | Respiratory | Cutaneous |
|---|---|---|
| Predominant region | Temperate zones | Tropical zones (more common than respiratory form) |
| Toxigenicity | Usually toxigenic strains | Usually non-toxigenic strains |
| Significance | Primary cause of mortality | Secondary infection on pre-existing skin lesions; acts as a reservoir and source for transmission |
| High-risk groups | Unimmunized children, waning-immunity adults | Homeless urban populations, travelers to endemic areas |
Global Epidemiology
- Diphtheria is rare in developed countries due to routine childhood vaccination
- Remains endemic in parts of Africa, Asia, Latin America, Middle East, and parts of Europe where immunization coverage is suboptimal
- Post-Soviet states (1990s): Major epidemic driven by declining immunization coverage, waning adult immunity, and population movement - a textbook example of resurgent diphtheria
- Recent large outbreaks: Indonesia, Laos, Haiti, Venezuela, Yemen, Bangladesh (since 2011); Nigeria and Yemen (2022-2023)
- WHO reported 8,819 global cases in 2017; ~7,097 in 2016
- In India (2018): 11,720 cases and ~180 deaths; major burden in Assam, Delhi, Rajasthan, West Bengal
Key Epidemiological Implications
- Herd immunity gap - since the vaccine is a toxoid (not directed against the organism), it prevents disease but not the carrier state; therefore, very high immunization rates must be maintained to protect non-immune individuals
- Adult susceptibility - waning immunity after childhood vaccination creates a growing pool of susceptible adults; booster doses every 10 years are recommended
- Epidemiological shift - improved socioeconomic conditions reduce natural immunity acquired through subclinical skin infections, changing the epidemiology in transitioning countries
- Carriers as hidden sources - especially nasal carriers, who are not clinically apparent
Control Measures (Epidemiological)
| Target | Measure |
|---|---|
| Cases | Isolation (hospital, ≥14 days or until 2 negative cultures); antitoxin + penicillin/erythromycin |
| Carriers | Erythromycin for 10 days; two negative cultures before clearance |
| Contacts | Throat swab + immunity assessment; booster if >5 years since last dose; prophylactic antibiotics for unimmunized contacts; surveillance for ≥1 week |
| Community | Active immunization with diphtheria toxoid - DPT/DTPw/DTPa in infancy; dT boosters in adults; pentavalent vaccine in national immunization programs |
Sources:
- Park's Textbook of Preventive and Social Medicine, pp. 180-182
- Harrison's Principles of Internal Medicine, 22nd Ed., 2025, pp. 1265+
- Red Book 2021 (AAP Committee on Infectious Diseases), pp. 304-307
Why is Tuberculin sensitivity test avoided for 4 weeks after getting measels containing vaccine
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
This is the key paragraph from Harrison's. Now I have everything needed for a complete, mechanistically thorough answer.
Why the Tuberculin Test is Avoided for 4 Weeks After a Measles-Containing Vaccine
The Short Answer
The measles vaccine (a live attenuated virus) replicates in the recipient and induces a state of transient immunosuppression - specifically suppressing cell-mediated (Type IV / delayed-type hypersensitivity) immunity. Since the Tuberculin Skin Test (TST/Mantoux) depends entirely on an intact cell-mediated response, this suppression produces a false-negative tuberculin result. The effect lasts at least 4-6 weeks.
Step-by-Step Mechanism
1. How the TST Works (The Baseline)
The tuberculin (PPD) test is a Type IV (delayed-type) hypersensitivity reaction:
- PPD antigen is injected intradermally
- Pre-sensitized CD4+ T lymphocytes (T-helper cells) recognize the antigen via antigen-presenting cells
- Activated T cells release cytokines (IFN-γ, IL-2) that recruit macrophages and cause local induration
- This takes 48-72 hours to develop
- The entire reaction depends on functional T-lymphocyte-mediated immunity
If T-cell function is suppressed for any reason, the TST returns a false-negative - even in a person who truly has latent TB infection.
2. How Wild-Type Measles Virus Causes Immunosuppression
Harrison's (22nd Ed.) explains this directly:
"The intense immune responses induced by measles virus infection are paradoxically associated with depressed responses to unrelated (non-measles virus) antigens. This state of immunosuppression persists for at least several weeks to months beyond resolution of the acute illness... Delayed-type hypersensitivity responses to recall antigens, such as tuberculin, are suppressed, and cellular and humoral responses to new antigens are impaired."
The key mechanisms behind measles-induced immunosuppression include:
| Mechanism | Detail |
|---|---|
| Lymphocyte depletion | Measles virus infects and causes apoptosis of lymphocytes, reducing T-cell numbers |
| T-cell signaling disruption | The measles hemagglutinin protein binds CD46 and SLAM (signaling lymphocytic activation molecule) on T cells, interfering with activation signaling |
| Cytokine dysregulation | Measles shifts the immune response, impairing the IFN-γ-driven TH1 arm that is necessary for DTH reactions |
| Dendritic cell dysfunction | Measles virus infects dendritic cells, impairing antigen presentation to T cells |
| Immunologic amnesia | Measles causes reductions in the magnitude and diversity of antibodies against previously encountered antigens, impairing immunologic memory broadly |
This immunosuppression is also why wild-type measles disease can reactivate latent tuberculosis and has historically been associated with increased susceptibility to secondary bacterial and viral infections for months afterward.
3. The Vaccine Replicates the Same Effect (to a Lesser Degree)
The live attenuated measles vaccine replicates in the host (that is how it generates immunity). During this replication - even though attenuated - it induces the same pattern of transient immune modulation seen with wild-type measles, albeit milder:
- The vaccine virus replicates for approximately 1-2 weeks post-administration
- During this period and shortly after, cell-mediated immunity to unrelated antigens (like tuberculin) is transiently suppressed
- This suppression lasts at least 4-6 weeks after vaccination
Jawetz Microbiology confirms:
"It [the tuberculin test] may be negative in the presence of tuberculous infection when 'anergy' develops because of overwhelming tuberculosis, measles, Hodgkin disease, sarcoidosis, AIDS, or immunosuppression."
The same phenomenon occurs with other live virus vaccines: varicella vaccine and yellow fever vaccine have similar (though less well-characterized) suppressive effects on TST reactivity.
4. The Practical Rule (from Red Book 2021)
The Red Book (AAP) provides the practical clinical guidance:
"Live attenuated measles, mumps, and rubella vaccines temporarily can suppress tuberculin reactivity for at least 4 to 6 weeks... If indicated, a TST can be performed or blood drawn for an IGRA at the same visit during which these vaccines are administered (i.e., before substantial replication of the vaccine virus)."
| Timing | What to do |
|---|---|
| Same day as vaccine | TST is acceptable - virus hasn't replicated yet, no suppression |
| After vaccine given (any day) | Wait ≥4 weeks before performing TST to avoid false-negative |
| If TST is needed urgently | Perform it first, before or simultaneously with the vaccine |
5. Does This Apply to IGRA (QuantiFERON/T-SPOT)?
The same precaution is recommended for IGRAs (Interferon-Gamma Release Assays) as a precaution:
"The effects of live-virus vaccination on IGRA characteristics have not been determined; the same precautions as for TST should be followed."
- Red Book 2021, p. 1221
Summary
The 4-week delay is necessary because the live attenuated measles virus replicates in the host after vaccination and - mirroring wild-type measles disease - transiently suppresses cell-mediated (T-lymphocyte) immunity. Since the tuberculin test is entirely dependent on a functioning delayed-type hypersensitivity (Type IV) response, performing it within this window yields a false-negative result, potentially missing latent TB infection. The suppression lasts at least 4-6 weeks, hence the recommended waiting period.
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Section on Measles - Immune Responses
- Red Book 2021 (AAP), pp. 1220-1221 - Tuberculosis, Testing Considerations
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed. - Reactions to Tuberculin
This is a shared conversation. Sign in to Orris to start your own chat.