Lab diagnosis for syphillis
Reading File
Finding Sources
Finding Sources
Searching the Web
syphilis laboratory diagnosis VDRL RPR TPHA FTA-ABS tests 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough answer. Let me compile the comprehensive response.
Laboratory Diagnosis of Syphilis
Syphilis is caused by Treponema pallidum, which cannot be cultured by routine laboratory methods. Diagnosis therefore relies on direct detection of the organism (microscopy, molecular methods) and indirect serologic testing (antibody detection). The approach varies by stage of disease.
1. Direct Detection Methods
A. Darkfield Microscopy
- The classic method for early-stage disease (primary and secondary syphilis, early congenital syphilis)
- Lesion fluid (chancre exudate, mucous patches, condyloma lata) is collected on a slide and examined within ~20 minutes
- Spirochetes appear as bright, motile organisms against a dark background because oblique light scatters off them
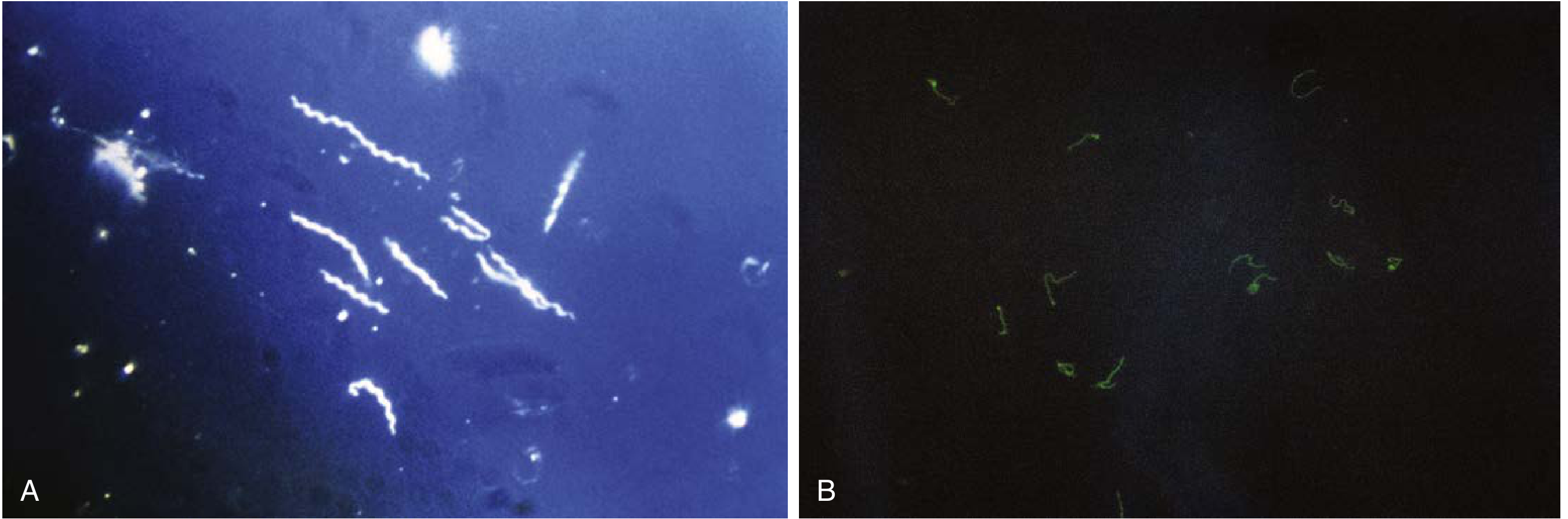
- Sensitivity: ~80% in primary syphilis
- Not recommended for oral lesions - saprophytic oral treponemes cause false positives
- Three genital commensal treponemes (T. phagedenis, T. refringens, T. minutum) can be confused with T. pallidum - careful cleaning is essential
B. Immunohistochemical Staining (Tissue Sections)
- Used by pathologists on paraffin-embedded tissue
- Primary anti-treponemal antibodies + enzyme-conjugated streptavidin complex highlight organisms
- Superior sensitivity and specificity over older silver impregnation stains
- Allows histologic localization of rare bacteria
C. PCR-Based Assays
- Detects T. pallidum DNA from lesion material, blood, CSF, or amniotic fluid
- Useful when darkfield is unavailable or lesions have healed
- Particularly valuable for: oral lesions (avoids false positives of darkfield), congenital syphilis, and neurosyphilis diagnosis
- T. pallidum cannot be continuously cultured in vitro; propagation for experimental use requires rabbit testes
2. Serologic Tests
Serologic testing is the cornerstone of diagnosis for all stages after primary lesions resolve. Two categories are used:
A. Nontreponemal (Anticardiolipin) Tests
These detect antibodies against cardiolipin-lecithin-cholesterol antigen - a lipoprotein material released from cells damaged by treponemes. They are not specific for T. pallidum but are excellent for screening and monitoring treatment.
| Test | Method | Primary Use |
|---|---|---|
| VDRL (Venereal Disease Research Laboratory) | Slide flocculation | Screening; also used for CSF in neurosyphilis |
| RPR (Rapid Plasma Reagin) | Circle card agglutination | Screening; preferred for blood samples |
| USR (Unheated Serum Reagin) | Similar to VDRL | Screening |
| TRUST (Toluidine Red Unheated Serum Test) | Similar to RPR | Screening |
Key features:
- Results are quantitative (titres e.g., 1:16, 1:32)
- Titers are highest in secondary syphilis (usually ≥1:16)
- A 4-fold rise in titre (e.g., 1:4 to 1:16) indicates active/new infection
- A 4-fold fall in titre after treatment indicates therapeutic response
- RPR/VDRL positivity falls to ~70% in late/latent syphilis; only ~70% positive in cardiovascular or late neurosyphilis
Prozone phenomenon: In high antibody excess (especially secondary syphilis), the VDRL/RPR may appear falsely negative. Diluting the serum paradoxically turns the test positive.
False positives (biological false positives - BFP):
Non-treponemal tests:
- Infections: infectious mononucleosis, malaria, viral hepatitis, HIV, leprosy, tuberculosis
- Autoimmune: SLE, antiphospholipid syndrome
- Physiologic: pregnancy, aging
- Hepatic cirrhosis, drug use
B. Treponemal (Specific) Tests
These detect antibodies directly against T. pallidum antigens. They are used to confirm a reactive nontreponemal test. Once positive, they usually remain reactive for life regardless of treatment, so they cannot be used to monitor therapeutic response.
| Test | Method | Notes |
|---|---|---|
| FTA-ABS (Fluorescent Treponemal Antibody Absorption) | Immunofluorescence with absorbed serum | Gold standard confirmatory test; reported as reactive/non-reactive |
| TP-PA (T. pallidum Particle Agglutination) | Microhemagglutination | Can be quantified and automated; similar performance to FTA-ABS |
| MHA-TP (Microhemagglutination - T. pallidum) | Microhemagglutination | Older version of TP-PA |
| EIA/CIA (Enzyme/Chemiluminescence Immunoassay) | Automated immunoassay | Increasingly used for primary screening (reverse algorithm) |
| FTA-ABS-19S-IgM | IgM-specific immunofluorescence | Special use: congenital syphilis, differentiating relapse from reinfection |
| IgM ELISA / SPHA | ELISA or solid-phase hemadsorption | Congenital syphilis, neurosyphilis, reinfection |
Key features:
- Approximately 1% of normal individuals have false-positive treponemal test results
- Cannot distinguish between syphilis and other treponematoses (yaws, pinta, bejel)
- Remain reactive for life even after successful treatment - unsuitable for monitoring
False positives (treponemal tests):
- Autoimmune diseases, HIV infection, hypergammaglobulinemia
- Other endemic treponematoses and borreliosis
3. Sensitivity by Stage
| Stage | VDRL (%) | FTA-ABS (%) | TP-PA (%) |
|---|---|---|---|
| Primary | 70 | 85 | 50-60 |
| Secondary | 99 | 100 | 100 |
| Latent or Late | 70 | 98 | 98 |
(Source: Goldman-Cecil Medicine, Table 295-3)
4. Testing Algorithms
Traditional (Classic) Algorithm
- Screen with nontreponemal test (RPR or VDRL)
- If reactive → confirm with treponemal test (FTA-ABS or TP-PA)
Reverse Algorithm (Increasingly Used)
- Screen with automated treponemal EIA or CIA
- If reactive → reflex to quantitative RPR or VDRL
- If nontreponemal is non-reactive but treponemal is reactive → a second treponemal test (e.g., TP-PA) resolves the discrepancy
The reverse algorithm allows high-throughput automated screening and may detect very early infection before RPR/VDRL turns positive, or detect previously treated long-standing syphilis.
5. Neurosyphilis Diagnosis (CSF)
CSF examination is indicated when neurologic symptoms are present:
- CSF-VDRL: highly specific but insensitive (~30-70%); a positive result is diagnostic
- CSF FTA-ABS: more sensitive; a negative result helps rule out neurosyphilis
- CSF pleocytosis (>5 WBC/mm³) and elevated protein support the diagnosis
- Serum RPR/VDRL may be negative in up to 30% of late neurosyphilis cases
6. Congenital Syphilis Diagnosis
- A nontreponemal titre ≥4-fold higher in the neonate than the mother is suggestive of infection
- IgG antibodies may be passively acquired from mother (transplacental) - makes interpretation tricky
- Detection of IgM antibodies (by FTA-ABS-19S-IgM or IgM ELISA) in the neonate is more specific, as IgM does not cross the placenta
- PCR on cord blood or neonatal samples
- Darkfield microscopy of skin lesions or body fluids in symptomatic neonates
7. Point-of-Care (Rapid) Tests
- Available for field settings and resource-limited contexts
- Can detect treponemal antibodies, nontreponemal antibodies, or both
- Sensitivity up to 98.5%, specificity up to 96%
- Positive results still require confirmatory testing
Summary: Test Selection by Clinical Scenario
| Scenario | Preferred Test(s) |
|---|---|
| Early primary (lesion present) | Darkfield microscopy; PCR |
| Primary/Secondary screening | RPR or VDRL |
| Confirmation of positive screen | FTA-ABS or TP-PA |
| Monitoring treatment response | Quantitative RPR or VDRL titres |
| Neurosyphilis | CSF-VDRL; CSF-FTA-ABS |
| Congenital syphilis | IgM ELISA; PCR; compare infant/maternal RPR titres |
| Oral lesions | PCR preferred (darkfield unreliable) |
| High-throughput screening | Automated CIA/EIA (reverse algorithm) |
All patients diagnosed with syphilis should be tested for HIV as well.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine 2-vol set (Table 295-2, 295-3); Dermatology 2-Volume Set 5e
This is a shared conversation. Sign in to Orris to start your own chat.