classify urgency of surgucal procedure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a thorough breakdown of the classification of surgical procedures by urgency, drawn from multiple authoritative surgical and anesthesia references.
Classification of Urgency of Surgical Procedures
There are two widely used frameworks: the ACC/AHA classification (used in anesthesia/cardiology) and the NCEPOD/CEPOD classification (used in UK surgical practice). Both are well accepted internationally.
1. ACC/AHA Classification (4 Categories)
Source: Barash Clinical Anesthesia, 9e - Table 23-2; adapted from ACC/AHA 2014 Perioperative Guideline
| Category | Description | Optimal Timing | Examples |
|---|---|---|---|
| Emergency | Life, limb, or organ-saving intervention | < 6 hours | Ruptured aortic aneurysm, major thoracoabdominal trauma, acute raised intracranial pressure |
| Urgent | Conditions that threaten life, limb, or organ | 6 - 24 hours | Perforated bowel, compound fracture, eye injury |
| Time-Sensitive | Patient is stable but requires timely intervention | Days to weeks | Tendon/nerve injuries, cancer resections |
| Elective | Procedure planned at patient or surgeon convenience | Up to 1 year | All other planned procedures |
2. NCEPOD Classification (UK National Standard)
Source: Bailey and Love's Short Practice of Surgery, 28th Ed.; Scott-Brown's Otorhinolaryngology
The National Confidential Enquiry into Patient Outcome and Death (NCEPOD) defines 4 levels of intervention urgency:
| NCEPOD Category | Timing | Description |
|---|---|---|
| Immediate | Within minutes | Life-saving; surgery proceeds alongside resuscitation (e.g., cardiac tamponade, exsanguinating hemorrhage) |
| Urgent | Within hours | Unplanned admission; resuscitation can be completed before theatre (e.g., sepsis requiring source control) |
| Expedited | Within days | Patient is stable but needs early intervention (e.g., fracture fixation, bowel obstruction without perforation) |
| Elective | Timing to suit patient, hospital, and staff | Planned procedure; no time pressure |
The older CEPOD scheme also used the term "Scheduled" - meaning admission prioritized within a few weeks of referral.
3. Key Practical Points
- In emergency surgery, the same preoperative assessment principles apply as in elective surgery, but the window for optimization is limited by time. Treatments should begin even if they cannot be completed before the procedure. (Bailey and Love's, 28th Ed.)
- Emergency theatre cases should be prioritized according to their NCEPOD category by the surgical and anesthetic teams.
- High-risk emergency patients should be assessed early for likely need of postoperative critical care (ICU/HDU).
- Some residual risks may remain despite optimization - these must be included in the consent process when possible.
- In obstetric surgery, a parallel system exists for cesarean sections (Categories 1-4), with Category 1 requiring delivery within 30 minutes for immediate maternal or fetal threat.
Summary Table
| Urgency | Timing Window | Risk Level | Decision Maker |
|---|---|---|---|
| Immediate / Emergency | Minutes to <6 h | Highest | Senior surgeon + anesthetist |
| Urgent | 6 - 24 h | High | Surgical team + ICU input |
| Expedited / Time-Sensitive | Days to weeks | Moderate | Planned but prioritized |
| Elective | Weeks to months | Lowest | Patient + surgeon preference |
Sources:
- Barash Clinical Anesthesia, 9e, Table 23-2 (ACC/AHA 2014 adaptation)
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 21 - Preoperative Assessment for Emergency Surgery
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Planning and Scheduling of Theatre Time

IMG_4060.jpeg
answer this question for dnb final theory exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have solid foundational content from the library. Let me now compose a comprehensive, exam-structured DNB Final Theory answer using all available information, supplemented by well-established anesthesia knowledge for neonatal myelomeningocele repair.
DNB Final Theory - Question 8
A meningomyelocele is present in a 3 kg, full term, 10-day neonate. What are your preoperative, intraoperative and postoperative concerns? (3+5+2)
PREOPERATIVE CONCERNS (3 marks)
1. Assessment of the Defect and Associated Anomalies
- Level of the lesion determines extent of neurological deficit - higher lesions (thoracic/lumbar) carry greater motor, sensory, and autonomic impairment
- Type - myelomeningocele (exposed neural tissue, no skin cover) is an open defect requiring early surgical closure, ideally within 24-72 hours to prevent meningitis and desiccation of neural tissue
- Associated anomalies must be identified:
- Chiari II malformation - present in nearly all myelomeningocele cases; causes herniation of medulla and cerebellar tonsils through foramen magnum - risk of apnea, stridor, swallowing dysfunction
- Hydrocephalus - present in ~75% of myelomeningocele patients; look for bulging fontanelle, increasing head circumference, irritability, sunset sign
- Neurogenic bladder - assess for urinary retention/overflow
2. Airway and Respiratory Assessment
- Chiari II malformation may cause central apnea, vocal cord paralysis, or stridor - critical airway concern
- Respiratory function may be compromised by high spinal cord lesion level
- Check for any signs of aspiration from bulbar dysfunction
3. Hydration, Nutrition, and Metabolic Status
- The exposed sac continuously loses fluid and heat - assess for dehydration, electrolyte imbalance
- Blood glucose monitoring is mandatory in a neonate (risk of hypoglycemia)
- IV access should be established and fluids running to compensate losses
- NPO status: neonate should be nil-by-mouth appropriately (2 hours for clear fluids, 4 hours for breast milk)
4. Infection Status
- An uncovered/leaking defect is an open wound - check for signs of meningitis (fever, irritability, neck rigidity, altered tone) or CSF leak
- Baseline investigations: CBC, CRP, blood cultures if infection suspected
- Prophylactic antibiotics should be started preoperatively
5. Sac Dressing and Positioning
- The sac must be covered with sterile, moist saline-soaked gauze and a sterile transparent dressing
- The baby must be nursed prone or in lateral decubitus at all times to prevent rupture or pressure on the sac
- This also affects IV placement - use upper limbs or scalp veins; avoid lower limbs in presence of neurological deficit
6. Latex Allergy Precautions
- Patients with myelomeningocele have a high incidence of latex allergy (up to 40-60%) due to repeated early exposure to latex-containing medical equipment
- A latex-free environment must be established from birth - use only latex-free gloves, tubing, and equipment
7. Consent and Ethics
- Parents must be counseled regarding prognosis, the selective approach to repair, and likely long-term disability
INTRAOPERATIVE CONCERNS (5 marks)
1. Positioning
- Surgery is performed in the prone position (for posterior defect closure)
- Careful padding and support required - chest rolls to allow free diaphragmatic excursion, eyes protected, no pressure on the sac
- Venous pooling in prone position can cause hypotension - pre-load with fluids
2. Temperature Regulation (Hypothermia Prevention)
- Neonates have a large surface area-to-body weight ratio, immature thermoregulation, and minimal subcutaneous fat
- Risk is amplified by the open sac (evaporative heat loss) and the prone position
- Use: warm OR, warming mattress, forced-air warming blanket, warm IV fluids, humidified circuit gases, wrap extremities
- Monitor temperature continuously - maintain 36.5-37.5°C
3. Airway Management and Anesthesia
- General anesthesia with endotracheal intubation is required
- Patient is intubated awake or in lateral position to avoid pressure on the sac during induction
- Induction in lateral position or with the baby prone with the sac well-supported
- Succinylcholine is generally avoided in the first 24-48 hours post-denervation due to risk of hyperkalemia (use rocuronium instead; though in a neonate this needs careful consideration)
- MAC requirements may be reduced in neonates - use volatile agents (sevoflurane) titrated carefully
- Chiari II may cause difficult airway due to brainstem herniation - have difficult airway equipment ready
4. Venous Access and Fluid Management
- Two secure IV lines essential - upper limb or scalp veins preferred
- Maintain normoglycemia with glucose-containing fluids alongside normal saline/Ringer's lactate
- Estimated blood volume (EBV) in a neonate = ~85 ml/kg = ~255 ml in a 3 kg baby
- Allowable blood loss is very small - meticulous surgical hemostasis and blood conservation critical
- Have packed red cells cross-matched and available (transfuse if >10% EBV loss)
5. Latex-Free Environment
- Strict latex-free protocol intraoperatively - all gloves, catheters, syringes, IV tubing must be latex-free
- Even a single latex exposure can trigger anaphylaxis in a sensitized neonate
6. Monitoring
- Standard: SpO2, ETCO2, ECG, NIBP (cycling on upper limb), temperature probe
- Consider precordial stethoscope for breath sounds
- Urinary catheter (latex-free) for urine output monitoring (~1 ml/kg/hr)
- Neuromuscular monitoring if NMBAs used
7. Hemodynamic Stability
- Neonates are exquisitely sensitive to blood loss and volatile agent-induced hypotension
- Maintain MAP appropriate for age; have vasopressors (dopamine, epinephrine) available
- Avoid air bubbles in IV lines - neonates may have patent foramen ovale and are at risk for paradoxical air embolism (prone position elevates venous air embolism risk)
8. Analgesia
- Intraoperative: opioids (fentanyl 1-2 mcg/kg) supplemented by local infiltration by surgeon (bupivacaine 0.25% with max dose ~2 mg/kg)
- Paracetamol IV/rectal as part of multimodal analgesia
POSTOPERATIVE CONCERNS (2 marks)
1. Respiratory and Airway
- Extubation readiness must be carefully assessed - Chiari II malformation may cause postoperative apnea, stridor, or vocal cord dysfunction
- High index of suspicion for central apnea - continuous SpO2 monitoring in NICU mandatory
- Some neonates may require elective postoperative ventilation
2. Positioning and Wound Care
- Continue nursing prone or lateral to protect the surgical repair
- Wound must be observed for CSF leak, dehiscence, or infection
3. Neurological Monitoring
- Monitor for worsening of neurological function compared to baseline
- Check head circumference daily - watch for progressive hydrocephalus requiring VP shunt placement
- Chiari-related symptoms: stridor, apnea, poor feeding, neck retraction
4. Fluid Balance and Nutrition
- Continue IV fluids with glucose maintenance; transition to enteral feeds as tolerated
- Urine output monitoring; catheterize as needed for neurogenic bladder
- Avoid hypernatremia or hyponatremia (neonates have immature renal handling)
5. Pain Management
- IV paracetamol, opioids with strict respiratory monitoring in NICU
- Avoid NSAIDs in neonates <28 days
6. Infection Prophylaxis
- Continue antibiotics perioperatively
- Monitor for signs of meningitis or wound infection
7. Latex Precautions Continued
- All postoperative care to remain latex-free
Summary Table for Quick Revision
| Phase | Key Concerns |
|---|---|
| Preoperative | Assess defect level + type; Chiari II + hydrocephalus; latex-free setup; sac protection; infection; fluid/glucose status; consent |
| Intraoperative | Prone positioning; hypothermia prevention; intubation in lateral/prone; latex-free; blood conservation; monitoring; venous air embolism |
| Postoperative | Apnea monitoring in NICU; hydrocephalus; wound/CSF leak; neurogenic bladder; nutrition; latex-free |
Sources:
- Miller's Anesthesia, 10e - Spina Bifida, Pediatric Neuroanesthesia
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Spina Bifida
- Barash Clinical Anesthesia, 9e - Classification and Neonatal Anesthesia
- ACC/AHA Perioperative Guideline 2014
anesthetic concern in hypertensive and diabetic patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from the library. Here is the full, structured answer suitable for DNB/MD exam preparation.
Anesthetic Concerns in a Hypertensive and Diabetic Patient
PART A: HYPERTENSIVE PATIENT
Preoperative Concerns
1. Assessment and Optimization
- Determine duration, severity, and end-organ damage from hypertension
- Classify using BP values: Stage 1 (130-139/80-89), Stage 2 (≥140/90), or hypertensive crisis (>180/120)
- Evaluate for target organ damage:
- Cardiac: LVH, IHD, CCF (ECG, Echo if indicated)
- Renal: proteinuria, elevated creatinine (urine albumin, S. creatinine)
- Neurological: history of TIA or stroke
- Vascular: peripheral vascular disease, retinopathy
2. Should Surgery Be Postponed?
- Elective surgery should be deferred if diastolic BP >110 mmHg or systolic >180 mmHg until adequate control is achieved
- Mild-to-moderate hypertension (BP <180/110) is NOT an independent indication to cancel or delay surgery
- Document baseline BP and optimize antihypertensive medications preoperatively
3. Antihypertensive Medications - Perioperative Management
| Drug Class | Perioperative Action |
|---|---|
| Beta-blockers | Continue - sudden withdrawal causes rebound tachycardia and hypertension |
| ACE inhibitors / ARBs | Controversy - generally held on morning of surgery (risk of refractory hypotension on induction); restart postoperatively |
| Calcium channel blockers | Continue |
| Diuretics | Omit morning dose to avoid hypovolemia and electrolyte disturbance |
| Alpha-2 agonists (clonidine) | Continue - withdrawal causes rebound hypertension |
4. Investigations
- ECG, Chest X-ray, Serum electrolytes (especially if on diuretics - check K+), S. creatinine, urine albumin
Intraoperative Concerns
1. Hemodynamic Lability
- Hypertensive patients have an exaggerated pressor response to laryngoscopy and intubation - heart rate and BP rise significantly
- Hypertensive patients also respond more dramatically to:
- Induction agents (hypotension from reduced vascular tone)
- Surgical stimulation (hypertension)
- Blood loss (hypotension)
- Target: maintain BP within 20% of preoperative baseline; avoid extremes
2. Blunting the Laryngoscopy Response
Strategies to attenuate pressor response to intubation:
- IV lignocaine 1.5 mg/kg, 90 seconds before laryngoscopy
- Fentanyl 2-3 mcg/kg at induction
- Esmolol 0.5-1 mg/kg (short-acting beta-blocker)
- Nitroglycerin sublingual/IV
- Deep anesthesia before instrumentation
- Use of video laryngoscopy to reduce time of laryngoscopy
3. Choice of Agents
- Induction: Thiopentone or propofol both acceptable; propofol causes greater hypotension - titrate carefully; etomidate is most hemodynamically stable
- Maintenance: Volatile agents (sevoflurane, isoflurane) are acceptable; they reduce SVR and can be used for BP control
- Avoid ketamine for induction (stimulates sympathetic system, raises BP)
4. Managing Intraoperative Hypertension
- Deepen anesthesia first
- IV vasodilators available (Box 50.9, Miller's Anesthesia):
- Labetalol (alpha + beta blockade)
- Hydralazine (direct arteriolar dilator)
- Nicardipine / Clevidipine (dihydropyridine CCBs - preferred, titratable)
- Sodium nitroprusside (most potent, risk of cyanide toxicity)
- Nitroglycerin (mainly venodilator, useful in IHD)
- Esmolol (short-acting, for tachycardia-driven hypertension)
5. Managing Intraoperative Hypotension
- More likely due to hypovolemia (diuretic use), impaired baroreflex, or blunted vasomotor responses
- Treat with IV fluids, vasopressors (phenylephrine, norepinephrine)
- ACE inhibitor/ARB preoperatively predisposes to refractory hypotension at induction
6. Monitoring
- NIBP every 2-5 min (or invasive arterial line for major surgery or severe hypertension)
- Continuous ECG (lead II + V5) for ischemia detection
- Urine output (maintain ≥0.5 ml/kg/hr)
Postoperative Concerns
- Hypertension is common postoperatively due to pain, agitation, hypercarbia, urinary retention
- Treat the cause first (analgesia, oxygen, catheterize)
- Anti-hypertensives: IV labetalol, hydralazine, or nicardipine if BP uncontrolled
- Restart oral antihypertensives as soon as patient can swallow
- Monitor for new neurological deficits, chest pain (perioperative MI), or renal function deterioration
PART B: DIABETIC PATIENT
Preoperative Concerns
1. Type of Diabetes and Baseline Control
- Determine: Type 1 vs. Type 2, current medications, insulin regimen
- HbA1c is the best marker of long-term glycemic control:
- HbA1c >8% (Type 1) or >7% (Type 2): consider delaying elective surgery for optimization
- Blood glucose on the morning of surgery
2. End-Organ Assessment
Diabetics have multisystem disease that must be assessed:
| System | Complication | Assessment |
|---|---|---|
| Cardiovascular | Silent IHD, CAD, CCF | ECG, Echo if indicated |
| Renal | Diabetic nephropathy | S. creatinine, eGFR, urine albumin |
| Neurological | Peripheral + autonomic neuropathy | Document existing deficits |
| Airway | Stiff joint syndrome (Type 1 DM) | "Prayer sign" test, atlanto-occipital mobility |
| GI | Gastroparesis | History of nausea, bloating, early satiety |
- Autonomic neuropathy predisposes to hemodynamic instability, orthostatic hypotension, and impaired baroreflex
- Peripheral neuropathy increases susceptibility to positioning injuries
- Stiff joint syndrome - glycosylation of temporomandibular, atlanto-occipital, and cervical spine joints in longstanding Type 1 DM can cause difficult intubation - perform thorough airway assessment and "prayer sign" test
3. Medication Management
| Drug | Perioperative Action |
|---|---|
| Oral hypoglycemics (sulfonylureas, glipizide) | Stop on day of surgery - risk of hypoglycemia |
| Metformin | Hold on day of surgery - risk of lactic acidosis (especially if contrast or hypoperfusion) |
| SGLT2 inhibitors (empagliflozin, dapagliflozin) | Stop 3-4 days before surgery - risk of euglycemic DKA |
| GLP-1 agonists (semaglutide) | Hold day of surgery - gastroparesis risk |
| Insulin (long-acting, basal) | Reduce by 20% the night before; continue basal at 80% on morning of surgery for Type 1 to prevent DKA |
| Insulin (short-acting) | Hold on morning of surgery unless glucose elevated |
4. Investigations
- Blood glucose, HbA1c, S. electrolytes (Na+, K+), S. creatinine, urine for ketones/albumin, ECG
5. Scheduling
- Schedule as first case of the day to minimize fasting time and metabolic stress
6. Aspiration Risk
- Gastroparesis (from autonomic neuropathy) - delayed gastric emptying → full stomach risk
- Consider RSI (rapid sequence induction) if gastroparesis suspected
- Premedicate with metoclopramide, H2 blocker, sodium citrate
Intraoperative Concerns
1. Glucose Monitoring - The Core Priority
- Check blood glucose on arrival, and every 1-2 hours intraoperatively
- Target glucose: 140-180 mg/dL (ADA recommendation); <200 mg/dL as minimum acceptable upper limit
- Hypoglycemia is more dangerous than hyperglycemia during anesthesia - symptoms are masked by the anesthetic state
- If BG <70 mg/dL: give IV dextrose immediately
2. IV Fluid and Insulin Management
- Avoid dextrose-containing fluids routinely (worsens hyperglycemia)
- Use Ringer's Lactate or Normal Saline for maintenance
- For major surgery: use GIK (Glucose-Insulin-Potassium) infusion or a separate insulin infusion with glucose monitoring every 1-2 hours
- Type 1 diabetics must always have some basal insulin running - never completely stop insulin in Type 1 DM (risk of DKA)
3. Hemodynamic Instability
- Autonomic neuropathy blunts the compensatory responses to blood loss, hypotension, and position changes
- Hypotension at induction is more common and more profound
- Monitor BP closely; vasopressors may be needed
4. Airway Concerns
- Stiff joint syndrome → difficult laryngoscopy/intubation
- Have video laryngoscope, bougie, and difficult airway trolley ready
- Gastroparesis → RSI if indicated
5. Temperature
- Diabetics have impaired temperature regulation - active warming measures required
6. Regional Anesthesia Considerations
- Regional anesthesia is often preferred in diabetics as it:
- Blunts the stress hormone response better
- Provides better postoperative analgesia
- Reduces hyperglycemia from surgical stress
- Caution: document pre-existing neuropathy; avoid regional if severe peripheral neuropathy (medico-legal)
Postoperative Concerns
- Continue glucose monitoring every 2-4 hours until eating normally
- Restart oral hypoglycemics only once the patient is tolerating oral intake
- Monitor for hypoglycemia - common when insulin regimens are continued but caloric intake is reduced
- Watch for PONV - common, delays resumption of oral intake and insulin regimen; use routine PONV prophylaxis
- Monitor wound healing - diabetics have impaired immunity and healing; wound infections are more common
- Assess for perioperative MI - silent ischemia is more common in diabetics (autonomic neuropathy)
- Adequate analgesia to reduce the stress response (which worsens hyperglycemia)
Coexistent Hypertension + Diabetes (Combined Concerns)
These conditions frequently occur together and share important implications:
- Cardiovascular risk is multiplicative - combined hypertension and DM dramatically increases CAD, perioperative MI, and stroke risk. Formal cardiac risk stratification (RCRI, ACC/AHA algorithm) is mandatory.
- Renal protection - both damage the kidneys; avoid nephrotoxic drugs (NSAIDs, aminoglycosides, contrast); maintain adequate renal perfusion intraoperatively
- Autonomic dysfunction - worsened in combined disease; hemodynamic instability is more pronounced
- Metformin + ACE inhibitor/ARB combination - both held on day of surgery; hold ACE/ARB to prevent refractory hypotension, hold metformin to prevent lactic acidosis
- Retinopathy + glaucoma - both can be present; avoid prone positioning if risk of IOP elevation
Summary: Key Points for Exam
| Issue | Hypertension | Diabetes |
|---|---|---|
| Postpone if | BP >180/110 (diastolic >110) | HbA1c >8%, ketoacidosis, BG >400 |
| Key preop drug | Continue beta-blockers; hold ACE/ARB | Stop OHAs; reduce insulin; stop SGLT2i 3-4 days pre-op |
| Major intraop risk | Pressor response to intubation; lability | Hypoglycemia, gastroparesis, difficult airway |
| Target | BP within 20% of baseline | BG 140-180 mg/dL |
| Key monitoring | Arterial line if severe | Blood glucose q1-2h |
| Feared complication | Perioperative MI/stroke | Silent hypoglycemia under anesthesia |
Sources:
- Barash Clinical Anesthesia, 9e - Diabetes Mellitus, Perioperative Glucose Management
- Miller's Anesthesia, 10e - Perioperative Hypertension, Box 50.9
- Mulholland & Greenfield's Surgery, 7e - Diabetes Mellitus
- ACC/AHA 2014 Perioperative Cardiovascular Guideline
Uptake and distribution of inhaled anesthetic agents for 5 marks dnb exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a complete, DNB Final Theory-level answer for 5 marks, drawn directly from authoritative anesthesia textbooks.
Uptake and Distribution of Inhaled Anesthetic Agents
Core Concept
The goal of inhalation anesthesia is to achieve an adequate partial pressure of anesthetic in the brain (Pbr). Since this cannot be measured directly, the alveolar partial pressure (FA) is used as a surrogate, because at equilibrium:
P(inspired) → P(alveolar) → P(arterial blood) → P(brain)
The rate at which FA approaches FI (inspired concentration) - expressed as the FA/FI ratio - determines the speed of induction. The faster FA/FI rises, the faster the induction.
I. Factors Affecting the Inspired Concentration (FI)
The concentration delivered to the patient depends on:
- Fresh gas flow rate - higher flow = FI closer to vaporizer setting
- Volume of the breathing circuit - smaller circuit = faster equilibration
- Circuit absorption - minimal with modern circuits
II. Factors Affecting Alveolar Concentration (FA) - Uptake
If there were no uptake by the body, FA would instantly equal FI. Because the pulmonary circulation removes anesthetic from alveoli during induction, FA lags behind FI (FA/FI <1.0). Three factors govern uptake:
1. Solubility in Blood - Blood:Gas Partition Coefficient (λb/g)
This is the single most important determinant of uptake and induction speed.
Definition: The ratio of anesthetic concentration in blood to that in gas phase at equilibrium (at 37°C).
- High λb/g = highly soluble = blood acts as a large reservoir = more anesthetic "disappears" into blood = alveolar partial pressure rises slowly = slow induction
- Low λb/g = poorly soluble = blood quickly saturated = alveolar partial pressure rises rapidly = fast induction
Blood:Gas Partition Coefficients (at 37°C):
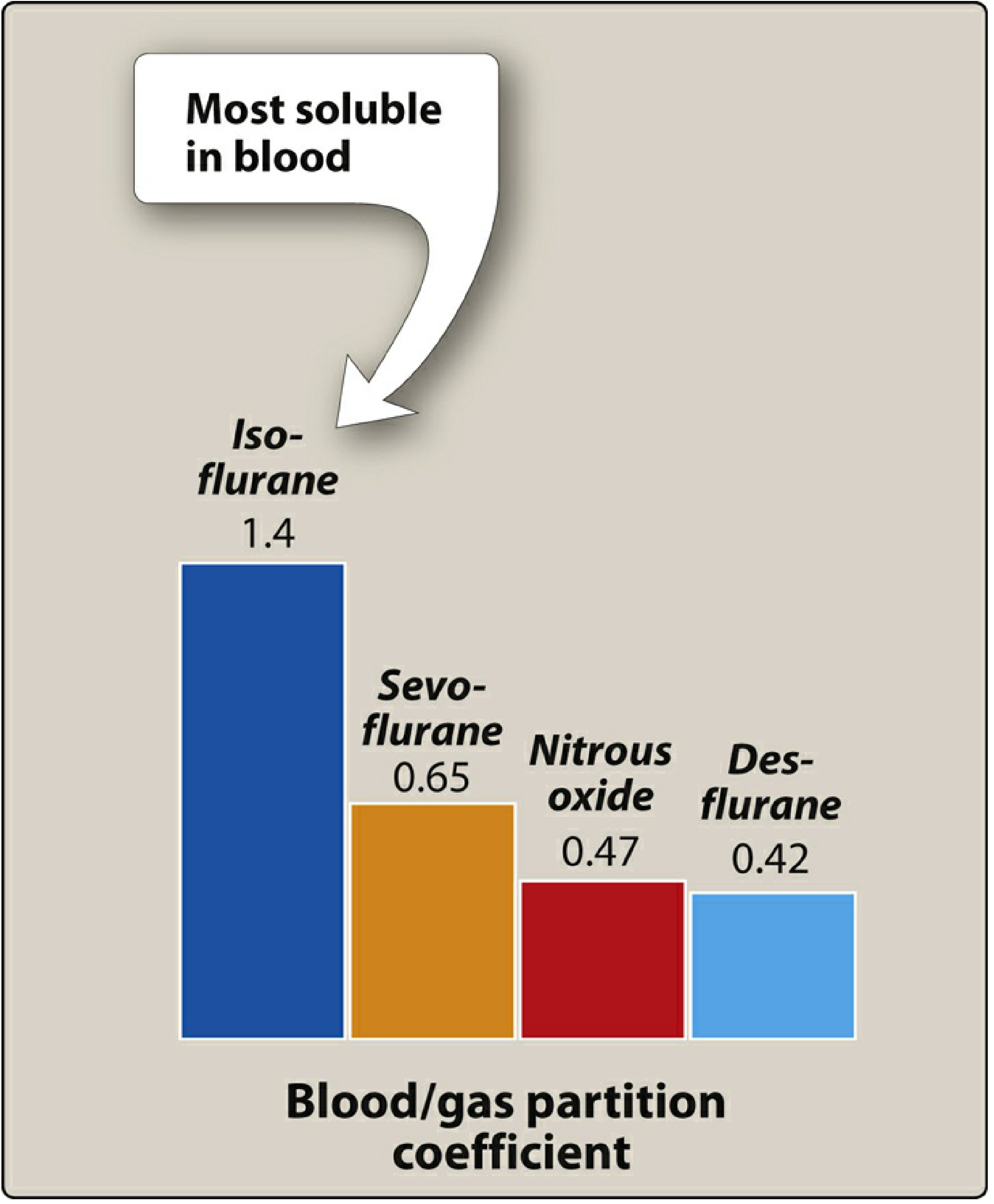
| Agent | Blood:Gas λ | Speed of Induction |
|---|---|---|
| Desflurane | 0.42 | Fastest |
| Nitrous oxide | 0.47 | Very fast |
| Sevoflurane | 0.65 | Fast |
| Isoflurane | 1.4 | Slower |
| Halothane | 2.4 | Slow |
2. Alveolar Blood Flow (Cardiac Output)
- Uptake = Solubility × Cardiac Output × (Palv - Pven)
- High cardiac output → more blood passing through alveoli → more anesthetic absorbed → FA rises slowly → slower induction
- Low cardiac output (e.g., shock) → less uptake → FA rises rapidly → faster induction, risk of overdose (especially with soluble agents like halothane)
- The cardiac output effect is less pronounced for insoluble agents (desflurane, N2O) because so little is taken up regardless of flow
3. Alveolar-to-Venous Partial Pressure Gradient (PA - Pv)
- Driven by tissue uptake in the periphery
- When tissues are unsaturated (start of induction), the returning venous blood has very low anesthetic partial pressure → large gradient → large pulmonary uptake → FA rises slowly
- As tissues saturate over time, venous partial pressure rises, the gradient narrows, and uptake decreases → FA approaches FI
III. Factors Affecting Alveolar Ventilation - Supply Side
These speed up the rise of FA/FI by delivering more anesthetic to the alveoli:
- Increased minute ventilation speeds induction - especially important for highly soluble agents (because uptake can match the faster delivery). For poorly soluble agents, the effect is minimal since they equilibrate quickly regardless.
- Decreased FRC (e.g., obese patients, children) → smaller volume to wash in → faster FA rise
- Children have a lower FRC relative to alveolar ventilation (VA/FRC ratio is higher) → faster induction by inhalation than adults
IV. The Concentration Effect and Second Gas Effect
Concentration Effect
- Increasing the inspired concentration (FI) not only raises FA but also accelerates the rate of rise of FA/FI
- Mechanism: When a large fraction of gas is absorbed, the remaining gas in the alveolus is "concentrated" (less total volume but proportionally more anesthetic)
- A secondary augmented inflow effect: absorbed gas volume is replaced by fresh gas inflow, further raising alveolar concentration
- Most clinically relevant with nitrous oxide (used at high concentrations, e.g., 70%)
Second Gas Effect
- High-concentration N2O uptake concentrates simultaneously administered volatile agents in the alveolus
- This accelerates the rise of FA/FI for the second gas (e.g., sevoflurane)
- Clinically significant at the start of induction when N2O uptake is greatest
V. Distribution - Tissue Compartments
Once absorbed into blood, anesthetic distributes to tissues. The rate of equilibration of each tissue depends on:
- Blood flow to the tissue
- Tissue:blood partition coefficient (storage capacity)
- Arterial-tissue partial pressure gradient
Tissues are classified into 4 groups (Morgan and Mikhail):
| Group | Tissues | % Body Weight | % Cardiac Output | Time to Equilibrium |
|---|---|---|---|---|
| Vessel-rich (VRG) | Brain, heart, liver, kidney, endocrine | 10% | 75% | Minutes |
| Muscle group | Skeletal muscle, skin | 50% | 19% | Hours |
| Fat group | Adipose tissue | 20% | ~6% | Days |
| Vessel-poor (VPG) | Bone, cartilage, ligaments, teeth, hair | 20% | <1% | Negligible |
- VRG saturates first - this is why brain equilibration is rapid at induction
- Muscle has moderate perfusion but large volume → sustained uptake for hours → relevant to context of prolonged surgery
- Fat is poorly perfused but has an enormous capacity for lipophilic volatile agents (fat:blood partition coefficients: halothane 60, isoflurane 45, sevoflurane 48) → takes days to reach steady state → prolonged anesthesia leads to accumulation in fat, delaying emergence
- VPG - essentially irrelevant to pharmacokinetics
VI. Ventilation/Perfusion (V/Q) Mismatch
- V/Q mismatch creates an alveolar-arterial difference in anesthetic partial pressure
- Raises alveolar partial pressure (especially for soluble agents)
- Lowers arterial partial pressure (especially for insoluble agents)
- A right-to-left shunt (e.g., cyanotic CHD) slows induction more with poorly soluble agents (N2O, desflurane) than with soluble ones
VII. Elimination
Recovery from anesthesia mirrors induction - the same factors that govern uptake now govern washout:
- Ventilation drives alveolar partial pressure down
- Blood:gas solubility determines how fast equilibration reverses
- Redistribution from brain back to blood, then to lung, then exhaled
- Desflurane and N2O are eliminated fastest (low λb/g)
- Isoflurane and halothane linger longer
- Biotransformation plays a minor role in elimination (halothane: ~20% metabolized; sevoflurane ~5%; desflurane <0.02%)
- Diffusion hypoxia (Fink effect): at end of N2O anesthesia, rapid outpouring of N2O from blood into alveoli dilutes alveolar O2 → give 100% O2 for first 5-10 min after N2O discontinuation
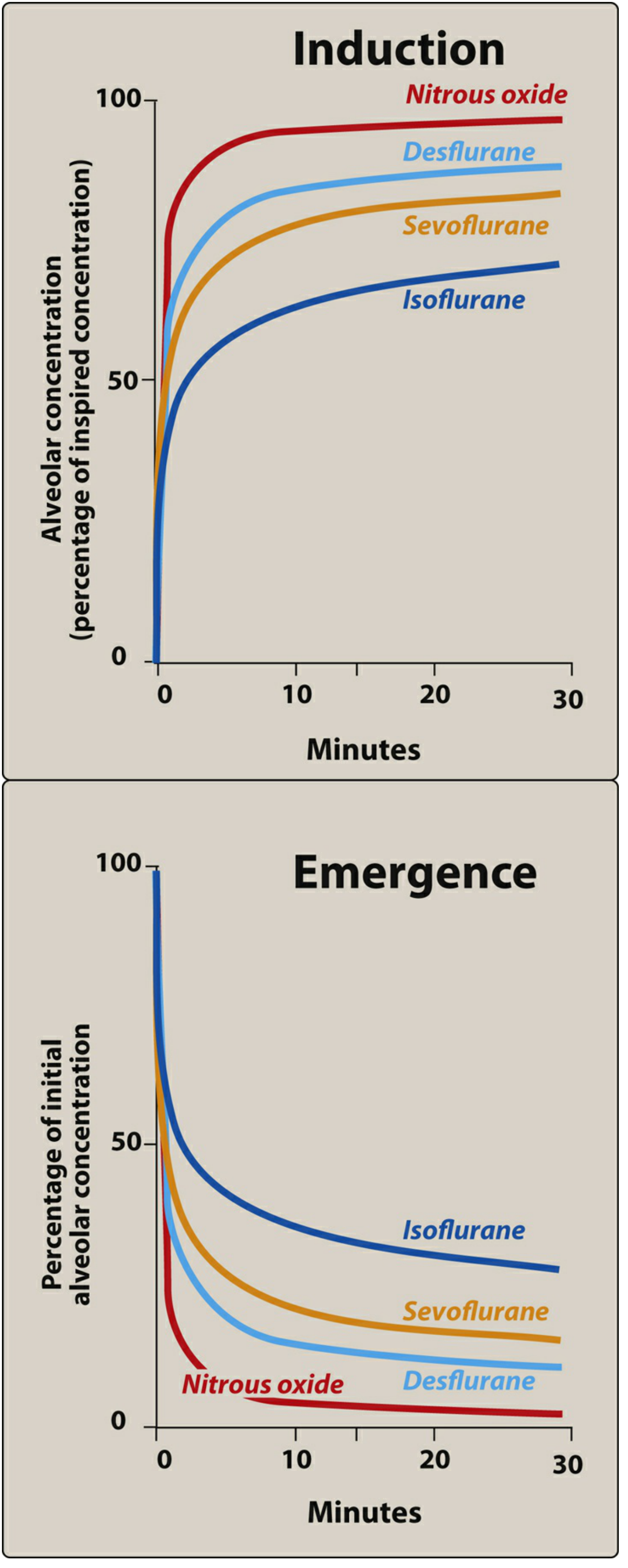
The top panel shows FA/FI rise during induction - agents with low blood:gas coefficients (N2O, desflurane) reach equilibrium fastest. The bottom panel shows washout during emergence - the same agents are eliminated most rapidly.
Summary Table - Key Exam Points
| Factor | Effect on FA/FI Rise | Clinical Implication |
|---|---|---|
| Low blood:gas λ | Faster | Desflurane/N2O - rapid induction & emergence |
| High blood:gas λ | Slower | Isoflurane/halothane - slow induction |
| High minute ventilation | Faster | Use hyperventilation to speed induction |
| High cardiac output | Slower | Sepsis, exercise - slower induction |
| Low cardiac output | Faster | Shock - overdose risk with soluble agents |
| High inspired concentration | Faster | Concentration effect |
| Right-to-left shunt | Slower (insoluble agents) | CHD patients - use soluble agents |
| Fat accumulation | Slow emergence | Obesity/prolonged surgery + soluble agents |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, Chapter 8
- Lippincott Illustrated Reviews: Pharmacology, Chapter 20
- Barash Clinical Anesthesia, 9e, Chapter 18
- Katzung Basic and Clinical Pharmacology, 16e, Chapter 25
This is a shared conversation. Sign in to Orris to start your own chat.