ECG from basics to advance in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation basics to advanced complete guide 2024
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed ECG guide.
ECG: From Basics to Advanced - A Complete Guide
Sources: Medical Physiology (Boron & Boulpaep), Miller's Anesthesia 10e, Fuster & Hurst's The Heart 15e, Harrison's Principles of Internal Medicine 22e, Goldman-Cecil Medicine, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Katzung's Pharmacology
PART 1 - FUNDAMENTALS
What Is an ECG?
The electrocardiogram (ECG/EKG) is a graphical recording of the electrical activity generated by the heart, detected at the body surface. It provides direct measurement of rate, rhythm, and the time-dependent electrical vector of the heart, and gives fundamental information about the origin and conduction of cardiac action potentials.
- Medical Physiology, p. 731
The Cardiac Conduction System
Understanding the ECG starts with understanding what generates its signals:
| Structure | Function | ECG Representation |
|---|---|---|
| SA (Sinoatrial) node | Primary pacemaker; initiates impulse | Beginning of P wave |
| Atria | Depolarize after SA node fires | P wave |
| AV (Atrioventricular) node | Slows conduction intentionally | PR interval delay |
| His bundle | Bridges AV node to ventricles | Part of PR interval |
| Left & right bundle branches | Rapid conduction to both ventricles | QRS complex |
| Purkinje fibers | Spread depolarization to myocardium | QRS complex |
| Ventricular myocardium | Contracts during systole | QRS + ST segment |
| Repolarization | Electrical recovery of ventricles | T wave |
The AV node is an area of relatively slow conduction, creating a physiologic delay between atrial and ventricular contraction. This is why the PR interval exists.
- Miller's Anesthesia 10e, p. 1364
The Cardiac Cycle and ECG Correlation

Fig. 13.1 from Miller's Anesthesia - Electrical and mechanical events during a single cardiac cycle.
- P wave - Atrial depolarization; onset of atrial systole coincides with SA node firing
- PR interval - Conduction delay through AV node; onset of P wave to start of QRS
- QRS complex - Ventricular depolarization; mitral valve closes at end of R wave
- ST segment - Plateau phase of ventricular action potential (isoelectric in normal)
- T wave - Ventricular repolarization
- QT interval - Total ventricular depolarization + repolarization time; shortens as heart rate increases
PART 2 - ECG PAPER AND LEADS
ECG Paper Calibration
- Horizontal axis (time): 0.04 sec per small box (1 mm); 0.2 sec per large box (5 mm)
- Vertical axis (voltage): 0.1 mV per mm; standard calibration = 1 mV = 10 mm tall
- 5 large boxes = 1.0 second
The 12-Lead System
Limb leads (frontal plane):
| Lead | View of Heart |
|---|---|
| I | Lateral (left arm to right arm) |
| II | Inferior (right arm to left foot) |
| III | Inferior (left arm to left foot) |
| aVR | From right shoulder - looks "into" the heart |
| aVL | Lateral (left arm) |
| aVF | Inferior (left foot) |
Precordial (chest) leads (horizontal plane):
| Lead | Position | View |
|---|---|---|
| V1 | 4th intercostal space, right sternal border | Septal |
| V2 | 4th intercostal space, left sternal border | Septal |
| V3 | Between V2 and V4 | Anterior |
| V4 | 5th intercostal space, midclavicular line | Anterior |
| V5 | Anterior axillary line | Lateral |
| V6 | Midaxillary line | Lateral |
PART 3 - SYSTEMATIC ECG INTERPRETATION
A reliable approach to every ECG follows this sequence:
Step 1 - Rate
Method 1 (regular rhythm): 300 ÷ number of large boxes between R waves
| Large boxes between R waves | Rate (bpm) |
|---|---|
| 1 | 300 |
| 2 | 150 |
| 3 | 100 |
| 4 | 75 |
| 5 | 60 |
| 6 | 50 |
Method 2 (exact): 60 ÷ R-R interval in seconds
Method 3 (irregular rhythm): Count QRS complexes in a 10-second strip, multiply by 6
- Normal: 60-100 bpm
- Bradycardia: <60 bpm
- Tachycardia: >100 bpm
Medical Physiology, p. 731
Step 2 - Rhythm
Ask: Is the rhythm regular or irregular? Are P waves present? Is each P wave followed by a QRS? Is the PR interval constant?
Normal Sinus Rhythm (NSR):
- Rate 60-100 bpm
- Regular R-R intervals
- Upright P waves in leads I, II, aVF
- Constant PR interval (0.12-0.20 sec)
- Each P followed by a QRS
Step 3 - Intervals and Durations
| Measurement | Normal Range | Significance if Abnormal |
|---|---|---|
| P wave duration | <0.12 sec (3 small boxes) | >0.12 sec = atrial enlargement/conduction delay |
| PR interval | 0.12-0.20 sec (3-5 small boxes) | Short = preexcitation; Long = AV block |
| QRS duration | <0.12 sec (<3 small boxes) | >0.12 sec = bundle branch block or ventricular rhythm |
| QT interval | Varies with rate; QTc <0.44 sec men, <0.46 sec women | Prolonged = risk of torsades de pointes |
| ST segment | Isoelectric (no elevation/depression) | Elevation = injury/STEMI; Depression = ischemia |
The QT interval shortens as heart rate increases. Use the corrected QT (QTc) using Bazett's formula: QTc = QT ÷ √(R-R interval in seconds).
Step 4 - Electrical Axis
The normal QRS axis in the frontal plane is -30° to +90°.
Quick method: Check leads I and aVF.
| Lead I | aVF | Axis |
|---|---|---|
| Positive | Positive | Normal (0° to +90°) |
| Positive | Negative | Left axis deviation (-30° to -90°) |
| Negative | Positive | Right axis deviation (+90° to +180°) |
| Negative | Negative | Extreme/northwest axis |
Causes of Left Axis Deviation (LAD): Left anterior fascicular block (most common), LVH, inferior MI, LBBB
Causes of Right Axis Deviation (RAD): RVH, RBBB, left posterior fascicular block, pulmonary embolism, dextrocardia
Causes of Right Axis Deviation (RAD): RVH, RBBB, left posterior fascicular block, pulmonary embolism, dextrocardia
Step 5 - P Wave Morphology
- P pulmonale: Tall, peaked P waves >2.5 mm in lead II - right atrial enlargement
- P mitrale: Broad, notched P wave >0.12 sec in lead II with biphasic P in V1 - left atrial enlargement
Step 6 - QRS Morphology
Look for: Q waves (normal vs. pathologic), R wave progression across precordial leads, bundle branch blocks.
Normal R wave progression: R wave grows from V1 to V5, with transition (R = S) around V3-V4.
Pathologic Q waves:
- Width >0.04 sec (1 small box) OR
- Depth >1/4 of following R wave
- Indicate prior myocardial infarction
Step 7 - ST Segment and T Wave
- ST elevation (>1 mm limb leads, >2 mm precordial leads): STEMI, pericarditis, Brugada, early repolarization
- ST depression: Subendocardial ischemia, digoxin effect, LVH strain
- T wave inversion: Ischemia, PE (right-sided), RBBB, LVH, normal in aVR and V1
PART 4 - BUNDLE BRANCH BLOCKS
When QRS duration is >0.12 sec (3 small boxes), suspect a bundle branch block (BBB). Use the WILLIAM MARROW mnemonic or the pattern in V1 and V6.
Right Bundle Branch Block (RBBB)
Criteria:
- QRS ≥ 0.12 sec
- RSR' ("M" or "rabbit ears") pattern in V1 (rSR')
- Wide, slurred S wave in leads I and V6
- T wave inversion in V1-V3 (appropriate discordance)
Causes: Normal variant, RVH, pulmonary embolism, ASD, ischemia, myocarditis
Left Bundle Branch Block (LBBB)
Criteria:
- QRS ≥ 0.12 sec
- Broad, notched R wave in V5, V6, I, aVL (no S wave)
- Deep, wide QS complex in V1
- No septal Q waves in lateral leads
- Discordant ST changes (opposite to QRS deflection)
Causes: IHD, cardiomyopathy, hypertension, aortic stenosis - LBBB is almost always pathological.
Clinical note: New LBBB in the context of chest pain was historically treated as STEMI equivalent. Current guidelines are more nuanced (use Sgarbossa criteria to assess for true STEMI in LBBB).
PART 5 - ARRHYTHMIAS
Bradyarrhythmias
Sinus Bradycardia
- Rate <60 bpm, normal P waves, regular rhythm
- Causes: Athletes, vagal tone, hypothyroidism, beta-blockers, sick sinus syndrome
AV Blocks:
| Type | ECG Features | Location | Progression Risk |
|---|---|---|---|
| 1st degree | PR > 0.20 sec, all P waves conduct | AV node | Benign |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR lengthening until P wave drops; then resets | AV node | Rarely progresses |
| 2nd degree Mobitz II | Constant PR, sudden dropped QRS without warning | Below AV node (His-Purkinje) | High - may progress to CHB |
| 3rd degree (Complete heart block) | P waves and QRS completely dissociated; atrial rate > ventricular rate | Any level | Emergency |
Diagnosis of complete AV block: P waves are dissociated from QRS complexes, with the atrial rate faster than the ventricular escape rate. Ventricular escape rate is typically 20-40 bpm if the escape pacemaker is in the ventricles (wide QRS) or 40-60 bpm if in the AV junction (narrow QRS).
- Goldman-Cecil Medicine, p. 1764
Supraventricular Tachyarrhythmias
Atrial Fibrillation (AF):
- Irregularly irregular rhythm
- No visible P waves - replaced by chaotic fibrillatory baseline (best seen in V1)
- Narrow QRS (unless aberrant conduction)
- Rate: Usually 100-170 bpm (ventricular response)
Atrial Flutter:
- Regular "sawtooth" flutter waves at 300 bpm (F waves)
- Typically 2:1 AV block giving ventricular rate of 150 bpm
- Flutter waves best seen in inferior leads (II, III, aVF) and V1
- Unlike AF, flutter waves are organized and regular
AVNRT (AV Nodal Reentrant Tachycardia) - most common SVT:
- Rate 150-250 bpm, regular
- Narrow QRS
- P waves buried in or just after QRS (retrograde P waves)
- Responds to vagal maneuvers and adenosine
AVRT (AV Reentrant Tachycardia - WPW related):
- May be narrow (orthodromic) or wide (antidromic)
- Short PR (<0.12 sec) + delta wave on baseline ECG = WPW pattern
- During tachycardia, typically narrow QRS (conduction goes normal route down His and back via accessory pathway)
Goldman-Cecil Medicine, p. 1753-1762
Differentiating SVT from VT in wide-complex tachycardia:
- AV dissociation = VT (P waves march through at own rate, independent of QRS)
- Fusion beats = VT (hybrid complexes where normal conduction fuses with ventricular focus)
- Capture beats = VT
- Concordance in precordial leads (all positive or all negative) = VT
Ventricular Arrhythmias
Premature Ventricular Complexes (PVCs):
- Wide (>0.12 sec), bizarre QRS
- No preceding P wave
- Followed by compensatory pause
- Isolated PVCs in structurally normal hearts are generally benign
Ventricular Tachycardia (VT):
- ≥3 consecutive PVCs at rate >100 bpm
- Wide QRS (>0.12 sec), regular
- AV dissociation, fusion beats, capture beats confirm VT
- Monomorphic VT: all QRS complexes look alike - often from a fixed scar (post-MI)
- Polymorphic VT: changing QRS morphology
Ventricular Fibrillation (VF):
- Chaotic, disorganized electrical activity
- No identifiable QRS complexes
- No cardiac output - immediately fatal without defibrillation
PART 6 - ISCHEMIA AND INFARCTION
The Progression of ECG Changes in MI
Myocardial ischemia and infarction produce characteristic, time-dependent ECG changes:
| Time | ECG Change | Mechanism |
|---|---|---|
| Minutes (hyperacute) | Tall, peaked (hyperacute) T waves | Early ischemia |
| Hours | ST elevation (STEMI) | Transmural injury current |
| Hours-days | Q wave development | Electrically dead tissue |
| Days-weeks | T wave inversion | Repolarization abnormality |
| Weeks-months | Persistent Q waves, T wave normalization | Scarring |
STEMI Localization by Leads
| Territory | Leads with ST Elevation | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD (Left Anterior Descending) |
| Anterolateral | V1-V6, I, aVL | Proximal LAD or LCx |
| Inferior | II, III, aVF | RCA (Right Coronary Artery) |
| Lateral | I, aVL, V5, V6 | LCx (Left Circumflex) |
| Posterior | ST depression V1-V3 + tall R in V1 | RCA or LCx |
| Right ventricular | ST elevation in V4R | Proximal RCA |
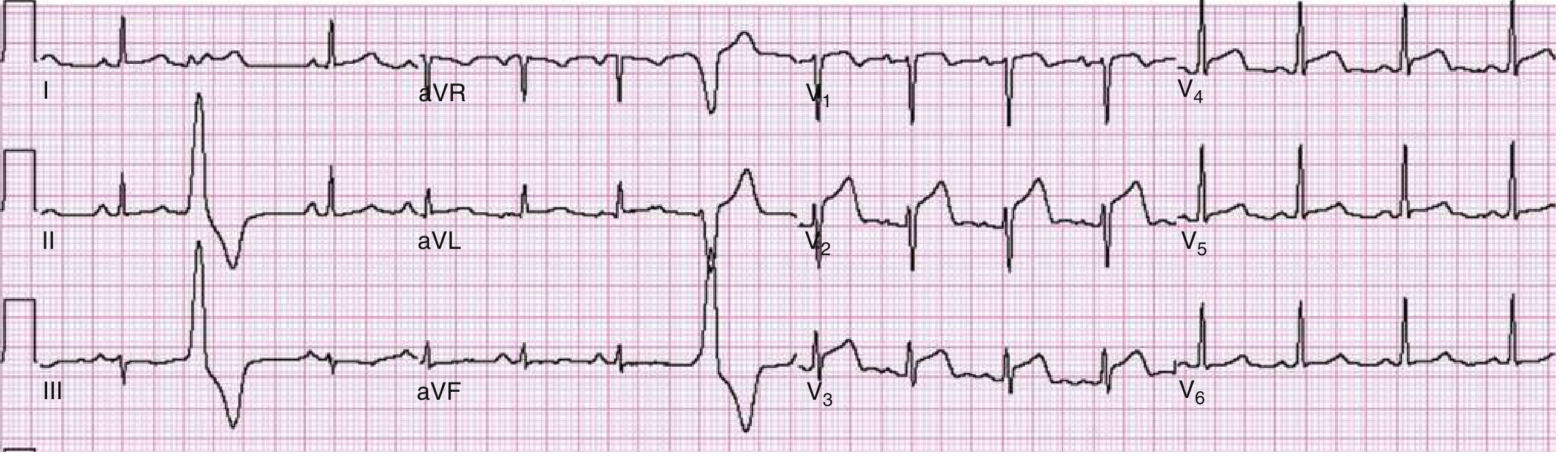
Fig. 64.6 from Rosen's Emergency Medicine - Anterior wall STEMI with ST elevation in V1-V4. LAD 90% stenosis confirmed on catheterization.
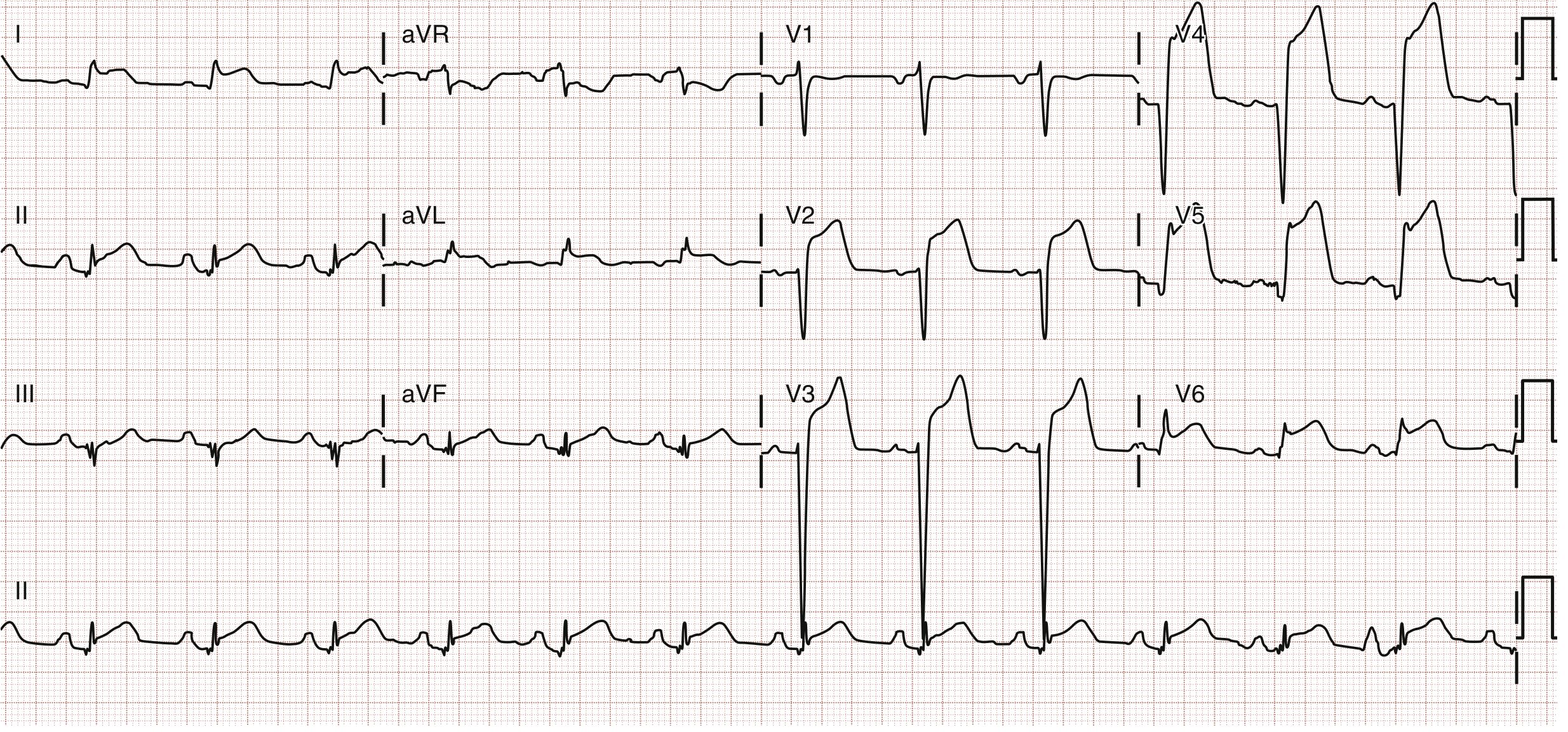
Fig. 64.7 from Rosen's Emergency Medicine - Anterolateral STEMI with STE in V2-V6, I, and aVL. In-stent thrombosis of LAD stent.
Special STEMI Patterns
aVR ST Elevation: >0.5 mV elevation in aVR is ~78% sensitive and 83% specific for left main coronary artery (LMCA) disease. Also consider proximal LAD occlusion or multivessel disease. If aVR elevation > V1 elevation, favors LMCA; if V1 > aVR, favors proximal LAD.
- Rosen's Emergency Medicine, p. 1004
de Winter Pattern (STEMI equivalent):
- Prominent tall T waves with J-point depression (ST depression) in precordial leads
- ST elevation in aVR
- Indicates proximal LAD occlusion; must be treated as STEMI
Wellens Syndrome:
- Deep symmetric T-wave inversions or biphasic T waves in V2-V3
- Occurs during pain-free period
- Indicates critical proximal LAD stenosis - do NOT stress test; needs urgent cath
PART 7 - ADVANCED PATTERNS
LVH (Left Ventricular Hypertrophy)
Most used criteria:
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥ 35 mm (sensitivity low ~40-60% in middle-age adults)
- Cornell: R in aVL + S in V3 > 28 mm (men) or >20 mm (women)
- Associated with ST-T changes in lateral leads ("strain pattern")
RVH (Right Ventricular Hypertrophy)
- Right axis deviation
- R > S in V1 (dominant R in V1)
- Deep S waves in V5-V6
- ST depression and T inversion in V1-V3
Pericarditis
- Diffuse ST elevation in multiple leads (not restricted to one territory)
- ST elevation is concave (saddle-shaped) upward
- PR depression (a key distinguishing feature from STEMI)
- No reciprocal ST depression (unlike STEMI)
- T wave inversion occurs after ST returns to baseline
Pulmonary Embolism (PE) - S1Q3T3 pattern
- S wave in lead I
- Q wave in lead III
- T wave inversion in lead III
- Also: sinus tachycardia (most common), new RBBB, right heart strain pattern (T inversion V1-V4), right axis deviation
- S1Q3T3 is specific but not sensitive - present in <20% of PE cases
Hyperkalemia - Progressive ECG Changes
- Peaked (tall, narrow) T waves - earliest sign
- Prolonged PR interval
- Widened QRS (loss of P waves)
- Sine wave pattern (merged QRS and T)
- Ventricular fibrillation / asystole
Hypokalemia
- Flattened T waves
- Prominent U waves (after T wave, best in V2-V3)
- Prolonged QU interval
- ST depression
Brugada Syndrome
- Type 1 (diagnostic): Coved-type (downsloping) ST elevation ≥2 mm in ≥1 of V1-V2, followed by negative T wave
- Can cause sudden cardiac death from polymorphic VT/VF
- ECG may be dynamic (appears and disappears)
Long QT Syndrome
- Congenital (mutations in ion channel genes) or acquired (drugs, electrolyte disturbances)
- QTc > 0.44 sec (men) or >0.46 sec (women)
- Risk of Torsades de Pointes - polymorphic VT with "twisting" QRS around the isoelectric line
- Acquired causes: hypokalemia, hypomagnesemia, antiarrhythmics (class Ia, III), antipsychotics, azole antifungals, fluoroquinolones
Wolff-Parkinson-White (WPW) Syndrome
- Accessory pathway (Bundle of Kent) bypasses AV node
- ECG features: short PR interval (<0.12 sec) + delta wave (slurred upstroke of QRS) + wide QRS
- Risk: AF with rapid accessory pathway conduction can lead to VF
- Never give AV nodal blocking agents (adenosine, verapamil, digoxin) in AF with WPW - can accelerate conduction down accessory pathway
PART 8 - STEP-BY-STEP SYSTEMATIC APPROACH (Summary Checklist)
When reading any ECG, use this structured sequence:
1. RATE - Calculate bpm (regular: 300/large boxes; irregular: count x6)
2. RHYTHM - Regular or irregular? P before every QRS?
3. P WAVES - Present? Morphology? Axis (upright in II)?
4. PR INTERVAL - 0.12-0.20 sec? Short (preexcitation)? Long (AV block)?
5. QRS - Width <0.12 sec? Morphology? Pathologic Q waves?
6. AXIS - Check leads I and aVF; Normal / LAD / RAD?
7. ST SEGMENT - Elevation or depression? Which leads?
8. T WAVES - Upright? Inverted? Hyperacute? Location?
9. QT INTERVAL - Calculate QTc; prolonged?
10. OVERALL - Clinical context + synthesize findings
Quick Reference: Key Normal Values
| Parameter | Normal Value |
|---|---|
| Heart rate | 60-100 bpm |
| PR interval | 0.12-0.20 sec |
| QRS duration | <0.12 sec |
| QTc | <0.44 sec (men), <0.46 sec (women) |
| QRS axis | -30° to +90° |
| R wave transition | V3-V4 |
| ST elevation threshold | <1 mm limb leads, <2 mm precordial leads |
Sources: Medical Physiology (Boron & Boulpaep); Miller's Anesthesia 10e; Fuster and Hurst's The Heart 15e; Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine International Edition; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Katzung's Basic and Clinical Pharmacology 16e; The Washington Manual of Medical Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.