Explane Cardiac cycle in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
cardiac cycle phases detailed physiology systole diastole pressure volume
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
I now have all the content and diagrams needed for a comprehensive answer. Let me compile the detailed explanation:
The Cardiac Cycle - A Detailed Explanation
The cardiac cycle refers to all the mechanical and electrical events that occur from the beginning of one heartbeat to the beginning of the next. At a heart rate of 75 beats/min, one complete cycle lasts 0.8 seconds (duration = 60 ÷ heart rate). Systole occupies ~300 ms and diastole ~500 ms. As heart rate increases, diastole shortens proportionally more than systole.
- Guyton and Hall Textbook of Medical Physiology, Ch. 9
- Costanzo Physiology 7th Edition, p. 160
- Medical Physiology (Boron & Boulpaep), p. 745
The Wiggers Diagram
The classic representation of the cardiac cycle (the "Wiggers diagram") plots all major cardiovascular parameters simultaneously against time:
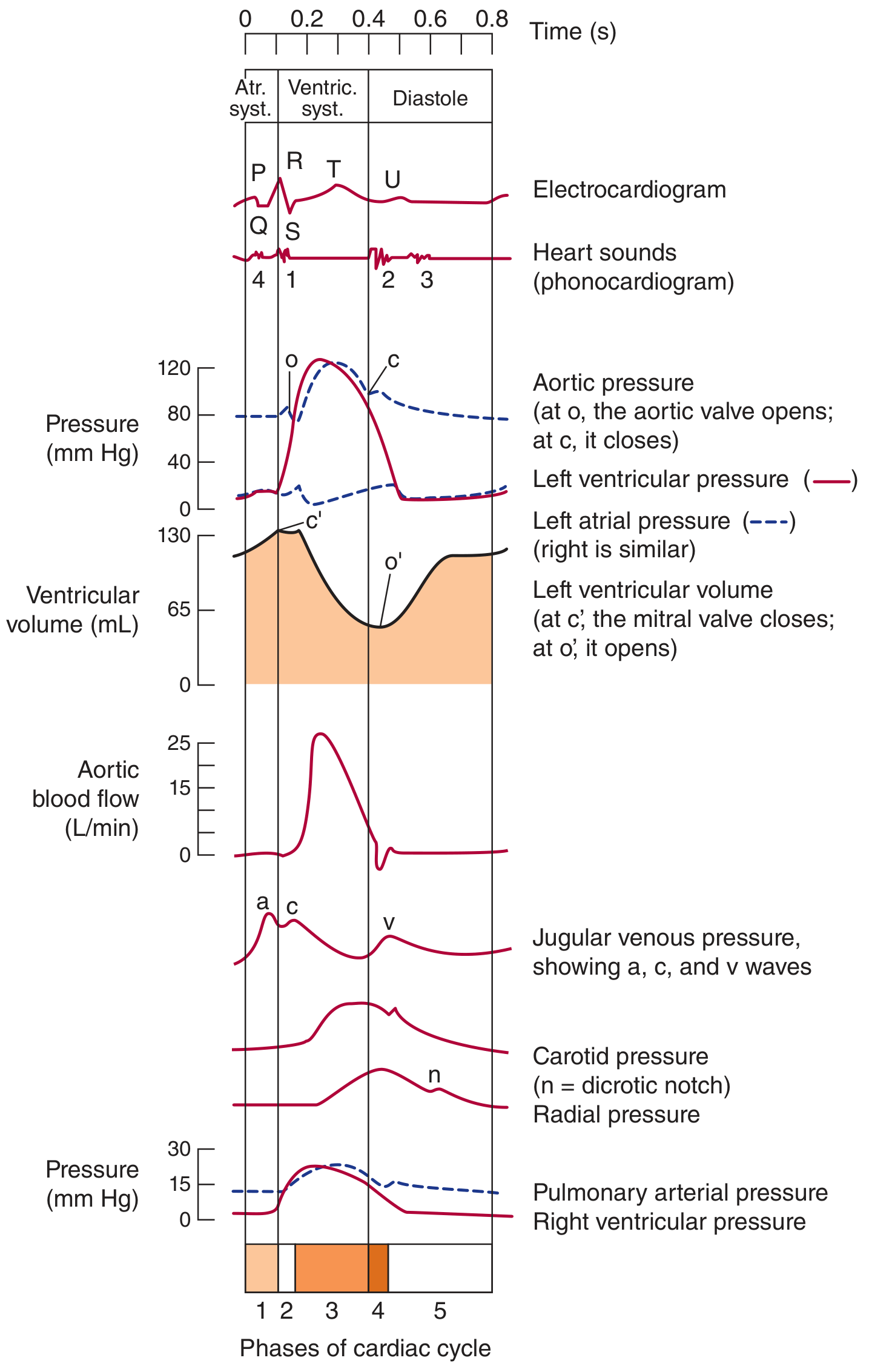
Ganong's Review of Medical Physiology - Events of the cardiac cycle at 75 beats/min. Phases: 1=atrial systole; 2=isovolumetric ventricular contraction; 3=ventricular ejection; 4=isovolumetric ventricular relaxation; 5=ventricular filling.
Right vs. Left Heart - Cardiac Cycle Phases
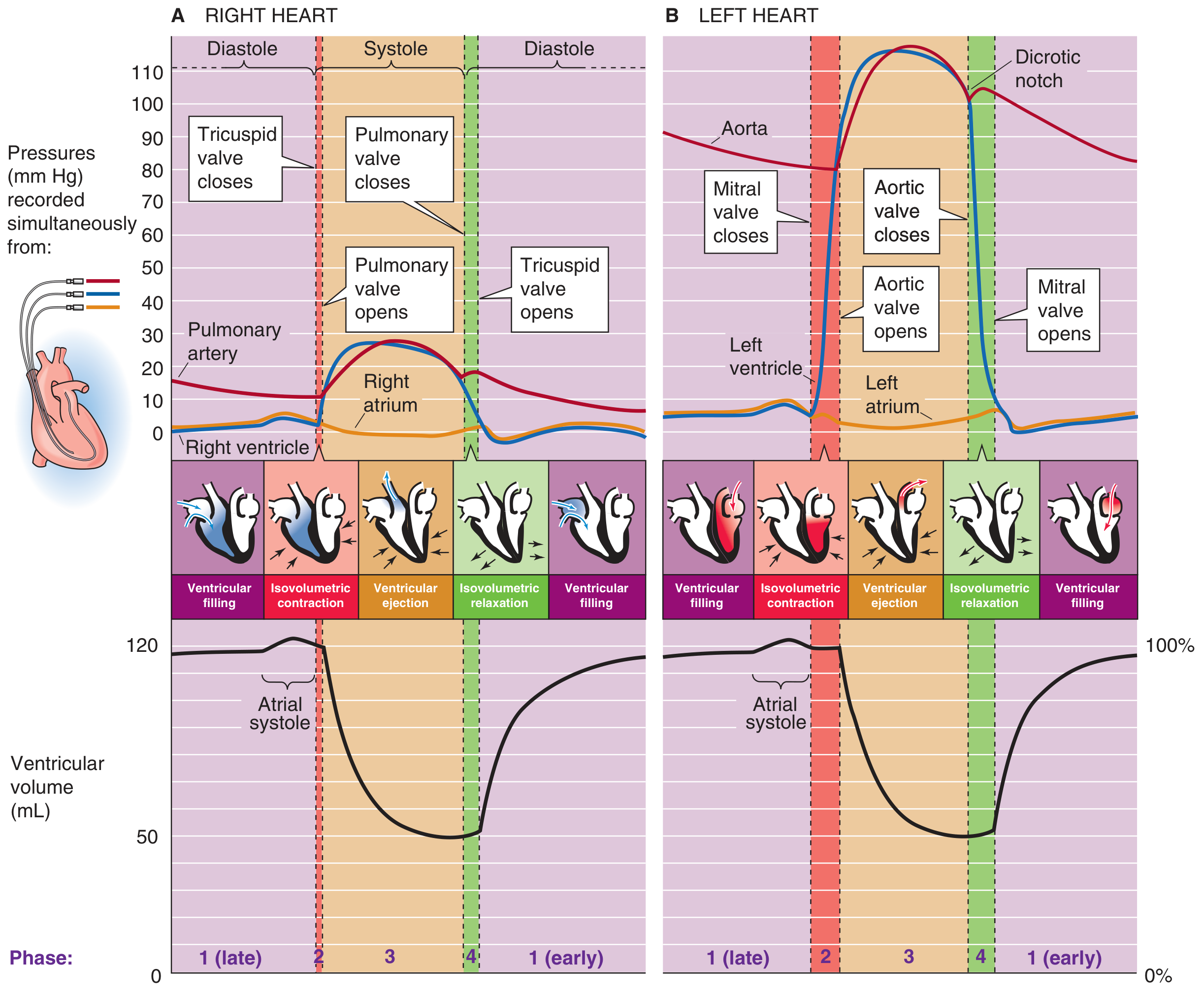
Medical Physiology - Pressures and ventricular volumes during the cardiac cycle for right heart (A) and left heart (B). The 4 numbered phases are visible with valve events and volume changes.
Initiation of the Cardiac Cycle
Each cycle begins with a spontaneous action potential in the sinoatrial (SA) node, located in the superior lateral wall of the right atrium near the superior vena cava opening. The impulse travels through both atria and then through the AV node and bundle of His into the ventricles. There is a built-in delay of >0.1 second at the AV node, which allows the atria to contract and "prime" the ventricles before ventricular contraction begins. This is why the atria are called "primer pumps."
The 7 Phases of the Cardiac Cycle (Costanzo Classification)
Costanzo Physiology divides the cycle into 7 distinct phases (A through G):
| Phase | Name | ECG Event | Valves | Heart Sounds | Key Events |
|---|---|---|---|---|---|
| A | Atrial Systole | P wave / PR interval | Mitral open | S4 (if present) | Atria contract; final ventricular filling |
| B | Isovolumetric Ventricular Contraction | QRS complex | Mitral closes | S1 | Ventricles contract; all valves closed; pressure rises at constant volume |
| C | Rapid Ventricular Ejection | ST segment | Aortic valve opens | - | Max ventricular and aortic pressure; rapid volume decrease |
| D | Reduced Ventricular Ejection | T wave | - | - | Slower ejection; volume reaches minimum (ESV) |
| E | Isovolumetric Ventricular Relaxation | - | Aortic valve closes | S2 | All valves closed; pressure falls at constant volume; dicrotic notch |
| F | Rapid Ventricular Filling | - | Mitral valve opens | S3 (if present) | Passive filling from atria; volume rises rapidly |
| G | Reduced Ventricular Filling (Diastasis) | - | - | - | Slow filling; prepares for atrial systole |
Phase-by-Phase Detail
Phase 1 - Diastole / Ventricular Filling
Diastasis (reduced filling): The mitral valve is open, but little blood flows. Ventricular volume slowly rises as pulmonary venous pressure drives blood across the open AV valve. Atrial and ventricular pressures are nearly equal.
Atrial Contraction (Atrial Systole): The P wave on the ECG signals atrial depolarization. Atrial contraction raises left atrial pressure, producing the "a" wave of the jugular venous pulse (JVP). Blood is actively ejected from the atrium into the relaxed ventricle through the open mitral valve. This "atrial kick" contributes less than 20% of total stroke volume at rest, but up to 40% during heavy exercise. This is why loss of atrial contraction (e.g., in atrial fibrillation) is usually asymptomatic in healthy hearts but can precipitate heart failure in compromised ones.
At the end of ventricular filling, the end-diastolic volume (EDV) is approximately 120-130 mL.
Phase 2 - Isovolumetric Contraction (Systole begins)
Following the QRS complex on the ECG, the ventricles depolarize and begin contracting. Left ventricular pressure rises sharply. The moment LV pressure exceeds left atrial pressure, the mitral valve closes - this produces the first heart sound (S1), the "lub."
With both the mitral and aortic valves now closed, the ventricle is a closed chamber. Ventricular pressure rises rapidly without any change in volume - this is why it is called "isovolumetric" (iso = same, volumetric = volume). During this period:
- Left ventricular pressure rises from ~5-10 mmHg up to ~80 mmHg
- No blood enters or leaves the ventricle
- This phase lasts approximately 50 ms
The "c" wave of the JVP corresponds to bulging of the tricuspid valve back toward the right atrium during this phase.
Phase 3 - Ventricular Ejection (Systole continues)
Once left ventricular pressure exceeds aortic pressure (~80 mmHg), the aortic valve opens and ejection begins. This phase has two sub-stages:
Rapid ejection: Ventricular pressure continues rising (reaching ~120 mmHg), closely followed by aortic pressure. Ventricular volume drops steeply as blood flows rapidly into the aorta. Both aortic and ventricular pressure peak during this phase.
Reduced ejection: The rate of ejection slows. Both aortic and ventricular pressures begin to fall. Importantly, aortic pressure eventually exceeds left ventricular pressure just before both reach their minimum - yet ejection continues briefly because of the inertia (momentum) of blood flow. The ventricle ultimately ejects about 70 mL (the stroke volume), leaving behind approximately 40-50 mL - the end-systolic volume (ESV).
- Stroke Volume (SV) = EDV - ESV = 130 - 50 = ~70 mL
- Ejection Fraction (EF) = SV/EDV = 70/130 = ~55-65% (normal ≥55%)
- Cardiac Output = SV × Heart Rate = 70 mL × 75 bpm ≈ 5.25 L/min
Phase 4 - Isovolumetric Relaxation (Diastole begins)
Blood flow across the aortic valve reverses direction (retrograde). This slams the aortic valve shut, generating the second heart sound (S2), the "dub." Aortic valve closure produces the characteristic dicrotic notch (incisura) visible on aortic pressure tracings - a brief upward deflection followed by a secondary dicrotic wave.
With both aortic and mitral valves closed, and the ventricle now relaxing, ventricular pressure falls rapidly while volume remains constant (isovolumetric). This continues until ventricular pressure drops below left atrial pressure.
Rapid Ventricular Filling (Early Diastole)
When LV pressure drops below atrial pressure, the mitral valve opens and blood rushes rapidly into the relaxed ventricle from the atria (which have been filling during systole). This rapid inflow can generate a third heart sound (S3), which is normal in children and young adults but pathological in older patients (indicates impaired ventricular compliance, as in heart failure).
Heart Sounds Summary
| Sound | Timing | Cause | Clinical Note |
|---|---|---|---|
| S1 ("lub") | Start of systole | Mitral + tricuspid valve closure | Heard best at apex |
| S2 ("dub") | End of systole | Aortic + pulmonic valve closure | Heard best at base |
| S3 | Early diastole | Rapid ventricular filling | Normal in young; pathological in HF if older |
| S4 | Late diastole (atrial systole) | Stiff ventricle resisting atrial filling | Always pathological; indicates reduced compliance (hypertrophy, ischemia) |
Jugular Venous Pulse (JVP) Waves
The JVP waveform reflects atrial pressure changes throughout the cycle:
| Wave | Timing | Cause |
|---|---|---|
| a wave | Atrial systole | Atrial contraction - rise in atrial pressure |
| c wave | Isovolumetric contraction | AV valve (tricuspid) bulging back toward atrium |
| x descent | Ventricular ejection | AV valve pulled downward; atria relax |
| v wave | Late systole/early diastole | Atrial filling while tricuspid is closed |
| y descent | Tricuspid valve opens | Blood rushes from atrium to ventricle |
Pressures: Left vs. Right Heart
| Parameter | Left Heart | Right Heart |
|---|---|---|
| Systolic pressure | ~120 mmHg | ~25 mmHg |
| Diastolic pressure | ~80 mmHg | ~10 mmHg |
| End-diastolic (filling) pressure | ~5-12 mmHg | ~2-6 mmHg |
| Valve events | Same timing | Same timing |
| Volume changes | Identical to right | Identical to left |
The shape of right and left heart pressure tracings is identical - the right is simply a "scaled-down version" operating at much lower pressures to serve the low-resistance pulmonary circulation.
Effect of Heart Rate on the Cardiac Cycle
When heart rate increases, the total cycle duration decreases. Diastole shortens disproportionately more than systole:
- At 75 bpm: systole = 0.27 s, diastole = 0.53 s
- At 200 bpm: systole = 0.16 s, diastole = 0.14 s
At very high heart rates, there is insufficient time for adequate ventricular filling during diastole, which reduces stroke volume and can impair cardiac output. This is the basis for the clinical concern with tachyarrhythmias.
Correlation with the ECG
| ECG Event | Cardiac Cycle Event |
|---|---|
| P wave | Atrial depolarization → atrial contraction begins |
| PR interval | AV nodal conduction delay |
| QRS complex | Ventricular depolarization → isovolumetric contraction begins |
| ST segment | Plateau of ventricular action potential; rapid ejection |
| T wave | Ventricular repolarization; reduced ejection |
| After T wave | Isovolumetric relaxation → ventricular filling |
Clinical Correlates
- Atrial fibrillation: Loss of coordinated atrial contraction removes the "atrial kick." Well-tolerated in healthy hearts but dangerous in those with stiff ventricles (hypertrophy, ischemia) where atrial filling is critical.
- Aortic stenosis: Increased resistance to outflow prolongs and intensifies the isovolumetric contraction phase. The ventricle must generate higher pressures; a harsh systolic ejection murmur results.
- Mitral regurgitation: Blood leaks backward into the atrium during systole (when the mitral valve should be tightly closed), causing a holosystolic murmur.
- Heart failure (systolic): Reduced ejection fraction; ESV increases and SV falls.
- Heart failure (diastolic): Normal EF but impaired relaxation during diastole; S4 gallop is characteristic.
Key references:
- Guyton and Hall Textbook of Medical Physiology - Ch. 9
- Costanzo Physiology 7th Edition - pp. 160-165
- Medical Physiology (Boron & Boulpaep) - pp. 744-749
- Ganong's Review of Medical Physiology, 26th Edition - pp. 540-542
This is a shared conversation. Sign in to Orris to start your own chat.