Give easy ways to understand cns in pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, easy-to-understand guide to CNS pharmacology, built from Katzung's Basic & Clinical Pharmacology (16th ed.).
CNS Pharmacology - A Simple, Structured Guide
The Big Idea: One Mental Model to Rule Them All
Every CNS drug does one (or more) of these things at a synapse:
- Mimics a neurotransmitter (agonist)
- Blocks a neurotransmitter receptor (antagonist)
- Increases neurotransmitter availability (blocks reuptake, blocks breakdown, stimulates release)
- Decreases neurotransmitter availability (blocks synthesis, blocks release, depletes stores)
- Modulates downstream signaling (second messengers, ion channels)
If you always ask "which transmitter, and what is the drug doing to it?" - you can figure out almost any CNS drug's effects and side effects.
Step 1: Understand the Basic Wiring
The Neuron and Synapse
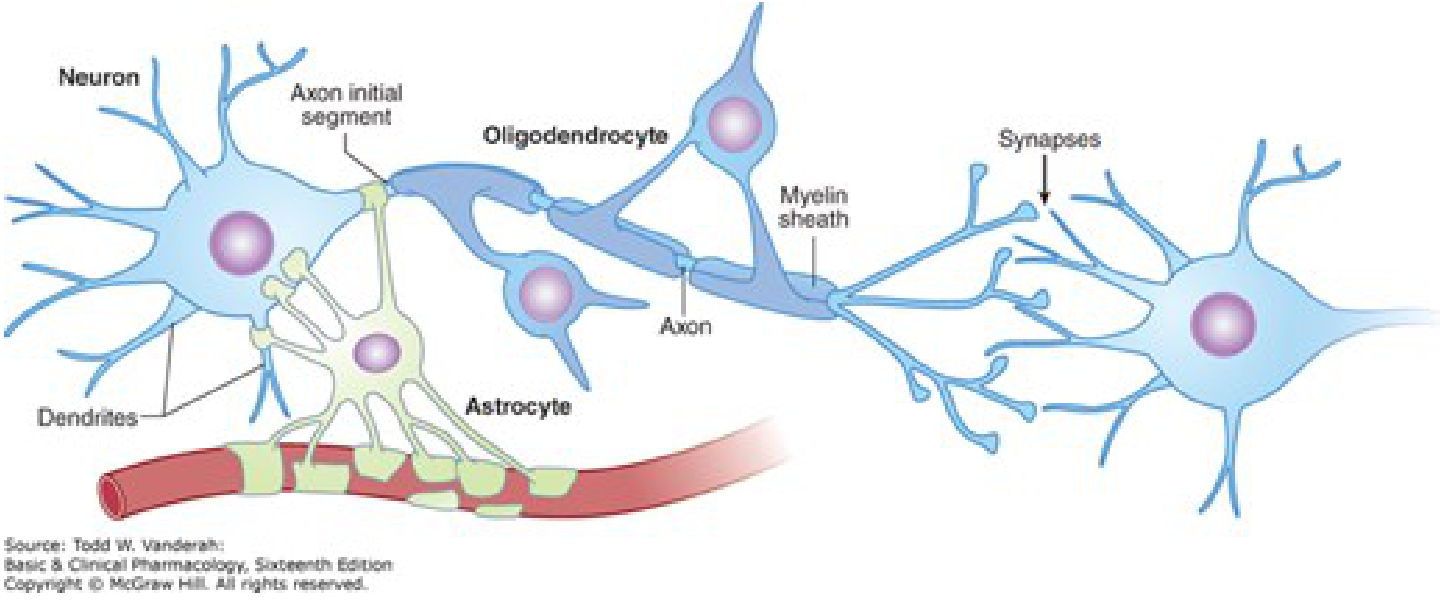
A neuron has dendrites (receive signals), a cell body, and an axon (sends signals). The axon is wrapped in myelin (made by oligodendrocytes). At the synapse, the signal is chemical:
- Action potential arrives at axon terminal
- Voltage-gated Ca²+ channels open → Ca²+ flows in
- Vesicles fuse, releasing neurotransmitter into the synaptic cleft
- Neurotransmitter binds postsynaptic receptor
- Signal is terminated by reuptake or enzymatic degradation
Why this matters for drugs: Drugs can interfere at every single one of these steps.
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 577-584
The Blood-Brain Barrier (BBB) - The Gatekeeper
A key reason CNS drugs are hard to design. Tight junctions between brain capillary endothelial cells, surrounded by astrocyte end-feet, block most drugs. To get into the CNS a drug must be:
- Highly lipid-soluble (lipophilic), OR
- Use a specific transporter
Classic example: Dopamine can't cross the BBB, but L-DOPA can (uses an amino acid transporter). So L-DOPA is given in Parkinson's disease, not dopamine itself.
Step 2: Understand the Two Receptor Types
| Feature | Ionotropic (Ligand-gated) | Metabotropic (GPCRs) |
|---|---|---|
| Speed | Fast (milliseconds) | Slow (seconds-minutes) |
| Mechanism | NT binds → ion channel opens directly | NT binds → G-protein → 2nd messengers |
| Examples | GABA-A, NMDA, nicotinic ACh | GABA-B, dopamine, serotonin (most), mAChR |
| Drug targets | Benzodiazepines, ketamine | Antipsychotics, antidepressants, opioids |
Easy trick: Ionotropic = "Instant." Metabotropic = "Meandering (slow)."
Step 3: Learn the 6 Key Neurotransmitter Systems
This is the heart of CNS pharmacology. Each system = a cluster of drugs.
1. GABA - The Brain's Brake Pedal
- Role: Main inhibitory transmitter. When GABA is active, the neuron is less likely to fire.
- Receptor: GABA-A (ionotropic, Cl⁻ channel) | GABA-B (metabotropic)
- Drugs:
- Benzodiazepines (diazepam, lorazepam): Enhance GABA-A → more Cl⁻ enters → more inhibition → sedation/anxiolysis/anticonvulsant
- Barbiturates (phenobarbital): Similar, but higher overdose risk
- Alcohol: Also enhances GABA-A
- Vigabatrin: Blocks GABA breakdown → more GABA available (anticonvulsant)
- Memory hook: "GABA = Calm down. Drugs that boost GABA = calm/sedate. Drugs that block GABA = seizures."
2. Glutamate - The Gas Pedal
- Role: Main excitatory transmitter. Fires neurons.
- Receptors: AMPA (fast, Na+), NMDA (slow, Ca²+, needs glycine co-agonist), metabotropic
- Drugs:
- Ketamine/Memantine: Block NMDA channel pore → anesthesia/anti-Alzheimer
- Lamotrigine: Blocks Na+ channels, reduces glutamate release → anticonvulsant
- Memory hook: "Glutamate = Go. Block it = less excitation = fewer seizures, less pain, anesthesia."
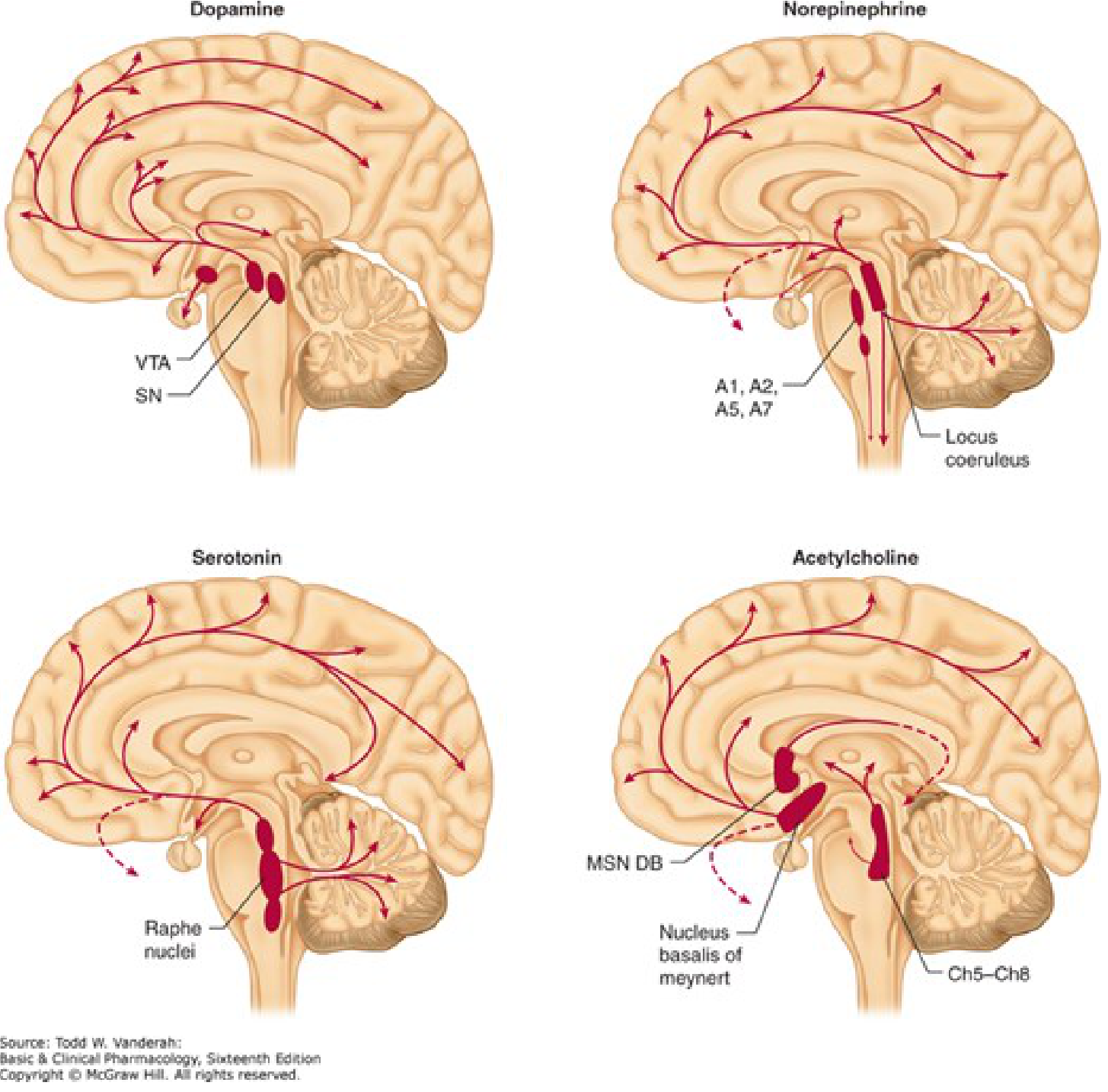
3. Dopamine - The Reward & Movement System
- Pathways:
- Nigrostriatal (SN → striatum): movement - loss causes Parkinson's
- Mesolimbic (VTA → limbic system): reward/pleasure - excess = psychosis
- Mesocortical (VTA → prefrontal cortex): cognition/motivation
- Tuberoinfundibular (hypothalamus → pituitary): prolactin regulation
- Drugs:
- L-DOPA: Dopamine precursor for Parkinson's (restores nigrostriatal dopamine)
- Antipsychotics (haloperidol, risperidone): Block D2 receptors → reduces psychosis. Block nigrostriatal D2 → extrapyramidal side effects. Block tuberoinfundibular D2 → hyperprolactinemia.
- Amphetamine/cocaine: Increase dopamine → euphoria, addiction
- Memory hook: "Dopamine - the 4 pathways decide all antipsychotic side effects."
4. Serotonin (5-HT) - Mood, Sleep, Appetite
- Origin: Raphe nuclei in brainstem → projects almost everywhere
- Drugs:
- SSRIs (fluoxetine, sertraline): Block serotonin reuptake transporter → more 5-HT at synapse → treats depression/anxiety
- SNRIs (venlafaxine): Block both serotonin AND norepinephrine reuptake
- Triptans (sumatriptan): 5-HT1B/1D agonists → treat migraine
- Ondansetron: 5-HT3 antagonist → antiemetic
- Buspirone: 5-HT1A partial agonist → anxiolytic
- Memory hook: "Serotonin runs from the raphe to everywhere. SSRIs block its reuptake = more available."
5. Norepinephrine (NE) - Arousal & Attention
- Origin: Locus coeruleus → projects broadly
- Drugs:
- SNRIs/TCAs: Block NE reuptake → antidepressant
- Atomoxetine: Selective NE reuptake inhibitor → ADHD
- Clonidine: Alpha-2 agonist → reduces NE release → lowers BP, treats ADHD/withdrawal
- Beta-blockers (propranolol): Block peripheral beta receptors → reduce performance anxiety
6. Acetylcholine (ACh) - Memory, Arousal, Muscle Control
- Receptors:
- Muscarinic (mAChR): CNS (memory, arousal), autonomic
- Nicotinic (nAChR): Neuromuscular junction, autonomic ganglia, CNS reward
- Drugs:
- Donepezil/Rivastigmine: Block acetylcholinesterase → more ACh → treats Alzheimer's
- Atropine: Muscarinic antagonist → blocks CNS and peripheral ACh
- Nicotine: nAChR agonist → stimulant, addiction
- Memory hook: "ACh = Memory. Block ACh in brain = confused/forgetful (anticholinergic side effects in elderly)."
Step 4: Where Drugs Act - Presynaptic vs Postsynaptic
| Location | Mechanism | Example |
|---|---|---|
| Presynaptic - synthesis block | Reduces transmitter made | AMPT (blocks catecholamine synthesis) |
| Presynaptic - storage block | Depletes vesicles | Reserpine (depletes monoamines) |
| Presynaptic - release block | Stops exocytosis | Tetanus toxin |
| Presynaptic - release stimulation | Floods synapse | Amphetamine (releases catecholamines) |
| Presynaptic - reuptake block | More NT in cleft | Cocaine, SSRIs, TCAs |
| Presynaptic - enzyme block | More NT in terminal | MAO inhibitors (more monoamines) |
| Postsynaptic - agonist | Mimics NT | Opioids (mimic enkephalin), L-DOPA |
| Postsynaptic - antagonist | Blocks NT action | Antipsychotics (block D2) |
| Ion channel - direct block | Blocks channel pore | Ketamine (NMDA), phenytoin (Na+) |
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 583-584
Step 5: Quick Disease-Drug Mapping
| Disease | Main Transmitter Imbalance | Drug Approach |
|---|---|---|
| Depression | Low serotonin + NE | SSRI, SNRI, TCA, MAOI |
| Anxiety | Low GABA | Benzodiazepines, buspirone, SSRIs |
| Schizophrenia | Excess dopamine (mesolimbic) | D2 blockers (antipsychotics) |
| Parkinson's | Low dopamine (nigrostriatal) | L-DOPA, dopamine agonists |
| Alzheimer's | Low ACh | Acetylcholinesterase inhibitors |
| Epilepsy | Excess glutamate OR low GABA | Enhance GABA (benzos, valproate) / Block Na+ (phenytoin) / Block glutamate (NMDA block) |
| ADHD | Low dopamine + NE (prefrontal) | Methylphenidate, amphetamine, atomoxetine |
| Pain (opioid) | Opioid receptors (MOR, KOR) | Morphine, codeine |
Study Tips for CNS Pharmacology
-
Draw the synapse once - label every step (synthesis → storage → release → receptor → reuptake → degradation). Then place drugs at each step. This one diagram explains 80% of CNS drug mechanisms.
-
Group by transmitter, not by drug class - Don't study "antidepressants" as a list. Study "what happens when you increase serotonin?" and the drug names follow naturally.
-
Learn side effects from mechanism - Antipsychotics block D2 everywhere, so: nigrostriatal = EPS, tuberoinfundibular = elevated prolactin, mesolimbic = antipsychotic effect. No memorization needed.
-
Use the BBB as a filter - Always ask "can this drug enter the brain?" Lipophilic = yes. Polar = no. Second-generation antihistamines are polar on purpose to avoid sedation.
-
Ionotropic = fast drugs (acute use), Metabotropic = slow drugs (chronic use) - Benzodiazepines (GABA-A, ionotropic) work in minutes. SSRIs (metabotropic pathway changes) take 2-4 weeks. This explains clinical timing.
-
Retrograde signaling - Remember endocannabinoids go backwards (postsynaptic → presynaptic), which is why cannabis has unique effects. This is pharmacologically distinct from all other transmitters.
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 21 - Introduction to the Pharmacology of CNS Drugs (p. 577-590)
This is a shared conversation. Sign in to Orris to start your own chat.