I now have comprehensive information from Gray's Anatomy for Students and other authoritative textbooks. Let me compile a thorough, well-structured lesson for you.
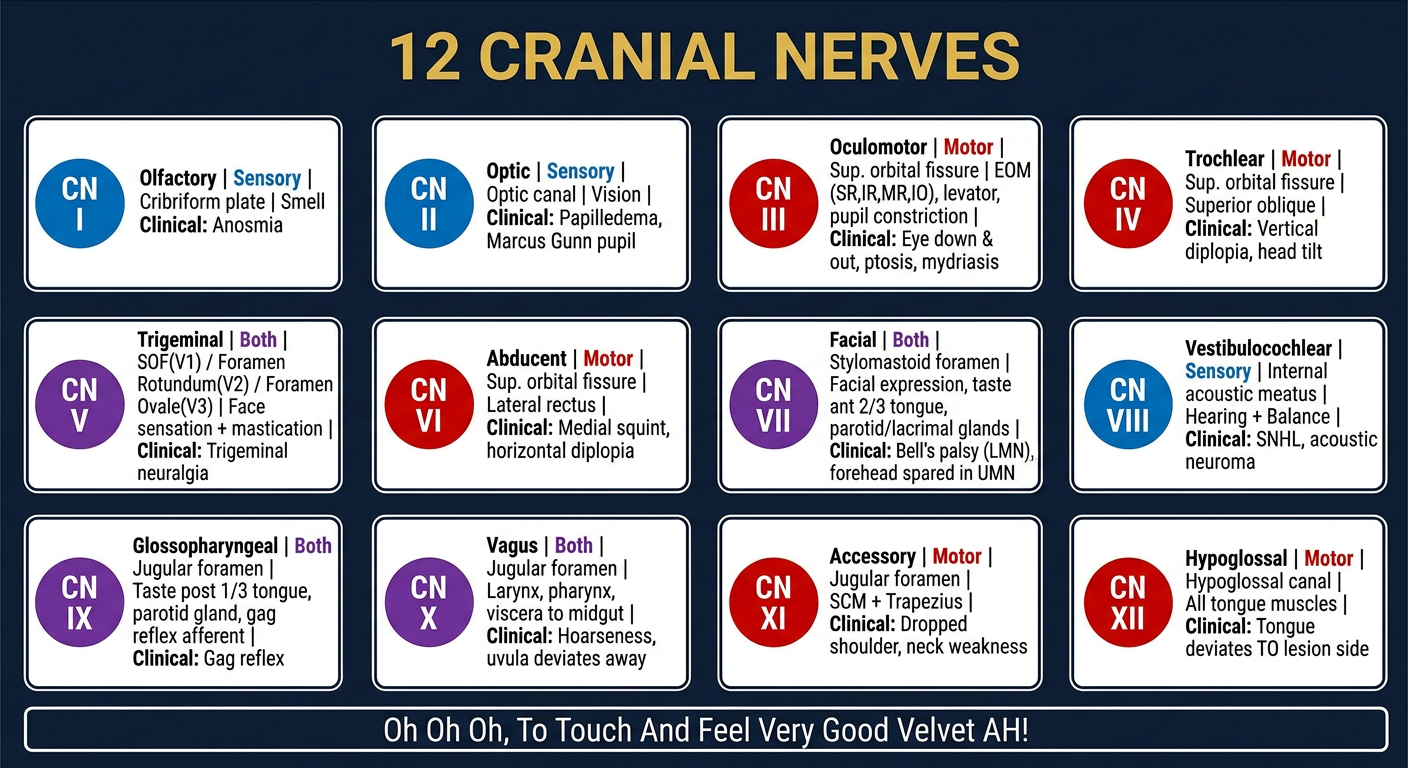
The 12 Cranial Nerves - Complete Guide for MBBS
Quick Memory Aid
Mnemonic for Names (in order):
"Oh Oh Oh, To Touch And Feel Very Good Velvet AH!"
I - Olfactory, II - Optic, III - Oculomotor, IV - Trochlear, V - Trigeminal, VI - Abducent, VII - Facial, VIII - Vestibulocochlear, IX - Glossopharyngeal, X - Vagus, XI - Accessory, XII - Hypoglossal
Mnemonic for Type (Sensory/Motor/Both):
"Some Say Money Matters But My Brother Says Big Brains Matter More"
S = Sensory, M = Motor, B = Both
Overview
All 12 pairs of cranial nerves are part of the peripheral nervous system (PNS) and exit the skull through foramina or fissures. All except CN XI (accessory nerve) originate directly from the brain.
They have 6 functional fiber types:
| Type | Abbreviation | Function |
|---|
| General somatic afferent | GSA | Touch, pain, temperature |
| General visceral afferent | GVA | Sensory from viscera |
| Special afferent | SA | Smell, taste, vision, hearing, balance |
| General somatic efferent | GSE | Motor to voluntary skeletal muscles |
| General visceral efferent | GVE | Motor to smooth muscle, glands |
| Branchial efferent | BE | Motor to pharyngeal arch-derived muscles |
CN I - Olfactory Nerve
| Feature | Detail |
|---|
| Type | Purely Sensory (Special Afferent - SA) |
| Function | Smell (olfaction) |
| Origin | Olfactory mucosa in nasal roof |
| Foramen | Cribriform plate of ethmoid bone |
| Nucleus | No nucleus in brainstem - fibers go directly to olfactory bulb |
Clinical point: Anosmia (loss of smell) - common after head injury (cribriform plate fracture) or with frontal lobe tumors. Test by asking patient to identify common smells (coffee, vanilla) - one nostril at a time.
CN II - Optic Nerve
| Feature | Detail |
|---|
| Type | Purely Sensory (Special Afferent - SA) |
| Function | Vision |
| Origin | Retinal ganglion cells |
| Foramen | Optic canal |
| Note | Technically an extension of the brain (not a true peripheral nerve) - surrounded by meninges |
Clinical point: Optic neuritis (demyelination - often in MS), papilledema (raised ICP), afferent pupillary defect (Marcus Gunn pupil). Test with Snellen chart and pupillary light reflex.
CN III - Oculomotor Nerve
| Feature | Detail |
|---|
| Type | Motor (GSE + GVE - parasympathetic) |
| Function | Most extraocular movements + pupil constriction + eyelid elevation |
| Origin | Midbrain (at level of superior colliculus) |
| Foramen | Superior orbital fissure |
| Muscles | Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae superioris |
| Parasympathetic | Via ciliary ganglion → constricts pupil (sphincter pupillae) + accommodation (ciliary muscle) |
Clinical point - CN III palsy:
- Eye looks "down and out" (unopposed action of SO and LR)
- Ptosis (drooping eyelid)
- Mydriasis (dilated, fixed pupil) - if compressive lesion (e.g., posterior communicating artery aneurysm)
- Surgical (compressive) CN III = pupil involved (the parasympathetic fibers run on the outside of the nerve)
- Medical (diabetic/hypertensive) CN III = pupil SPARED (ischemia affects core fibers first)
CN IV - Trochlear Nerve
| Feature | Detail |
|---|
| Type | Motor (GSE) |
| Function | Superior oblique muscle (intorsion, depression, abduction of eye) |
| Origin | Midbrain (just caudal to CN III complex) |
| Foramen | Superior orbital fissure (above common tendinous ring) |
| Special feature | Only cranial nerve that exits dorsally from the brainstem and crosses to the opposite side |
Clinical point: CN IV palsy causes vertical diplopia. Patient tilts head away from the affected side to compensate (Bielschowsky head tilt test). Most common cause is head trauma.
CN V - Trigeminal Nerve
| Feature | Detail |
|---|
| Type | Both (Sensory + Motor) - largest cranial nerve |
| Function | Sensation of face + Motor to muscles of mastication |
| Origin | Pons |
| 3 Divisions | V1 (Ophthalmic), V2 (Maxillary), V3 (Mandibular) |
| Division | Foramen | Sensory Area |
|---|
| V1 - Ophthalmic | Superior orbital fissure | Forehead, scalp, upper eyelid, cornea, nose tip |
| V2 - Maxillary | Foramen rotundum → infraorbital foramen | Cheek, lower eyelid, upper lip, upper teeth |
| V3 - Mandibular | Foramen ovale | Lower lip, lower teeth, chin, anterior 2/3 tongue (general sensation), auricle |
- Motor fibers only in V3 - innervate muscles of mastication (masseter, temporalis, medial and lateral pterygoids) + tensor tympani, tensor veli palatini, mylohyoid, anterior belly of digastric
Clinical points:
- Trigeminal neuralgia - severe lancinating pain in V2/V3 distribution
- Corneal reflex - afferent via V1 (ophthalmic), efferent via CN VII
- Jaw deviation toward the weak side in V3 palsy (pterygoids open the jaw)
CN VI - Abducent Nerve
| Feature | Detail |
|---|
| Type | Motor (GSE) |
| Function | Lateral rectus muscle (abduction of eye) |
| Origin | Pons (at pontomedullary junction) |
| Foramen | Superior orbital fissure |
| Note | Longest intracranial course - very vulnerable to raised ICP |
Clinical point: CN VI palsy causes medial deviation of the eye (convergent squint/esotropia) and horizontal diplopia - worse on looking toward the affected side. Commonly a false localizing sign in raised ICP.
CN VII - Facial Nerve
| Feature | Detail |
|---|
| Type | Both (Most complex cranial nerve!) |
| Origin | Pons |
| Exit | Stylomastoid foramen (after traversing facial canal in temporal bone) |
Fiber components:
- BE (Branchial Efferent): Muscles of facial expression, stapedius, posterior belly of digastric, stylohyoid
- GVE (Parasympathetic): Lacrimal gland (via pterygopalatine ganglion), submandibular and sublingual glands (via submandibular ganglion)
- SA (Special Afferent): Taste from anterior 2/3 of tongue (via chorda tympani)
- GSA: Skin of external acoustic meatus
Key branch - Chorda tympani: Carries taste from anterior 2/3 tongue + preganglionic parasympathetic to submandibular/sublingual glands.
Clinical points - Bell's Palsy (LMN CN VII palsy):
- All ipsilateral facial muscles paralyzed - including forehead (forehead sparing = UMN lesion)
- Loss of corneal reflex (efferent)
- Hyperacusis (stapedius paralysis)
- Loss of taste anterior 2/3 tongue (if lesion above chorda tympani)
- Inability to close eye → exposure keratitis
UMN vs LMN CN VII palsy:
| Feature | UMN | LMN |
|---|
| Forehead | Spared | Involved |
| Cause | Stroke, tumor | Bell's palsy, parotid tumor |
| Eye closure | Normal | Impaired |
CN VIII - Vestibulocochlear Nerve
| Feature | Detail |
|---|
| Type | Purely Sensory (Special Afferent - SA) |
| Function | Hearing (cochlear division) + Balance (vestibular division) |
| Origin | Cochlea + semicircular canals / otolith organs |
| Foramen | Internal acoustic meatus |
Clinical points:
- Sensorineural hearing loss - cochlear/CN VIII lesion
- Rinne positive (AC > BC) in sensorineural loss; Rinne negative (BC > AC) in conductive loss
- Weber lateralizes to good ear in sensorineural loss, bad ear in conductive loss
- Acoustic neuroma (vestibular schwannoma) - affects CN VIII in internal acoustic meatus, also compresses CN VII
CN IX - Glossopharyngeal Nerve
| Feature | Detail |
|---|
| Type | Both (Sensory + Motor) |
| Origin | Medulla oblongata |
| Foramen | Jugular foramen |
Fiber components:
- GVA: Carotid body (chemoreceptors) and carotid sinus (baroreceptors) + posterior 1/3 tongue, palatine tonsils, oropharynx, middle ear, pharyngotympanic tube
- SA (taste): Posterior 1/3 of tongue
- GVE (Parasympathetic): Parotid gland (via otic ganglion)
- BE (Motor): Stylopharyngeus muscle only
Clinical points:
- Gag reflex: Afferent = CN IX, Efferent = CN X
- Carotid sinus syncope
- Glossopharyngeal neuralgia (rare - pain in throat, tonsil, ear)
CN X - Vagus Nerve
| Feature | Detail |
|---|
| Type | Both (most widespread cranial nerve) |
| Origin | Medulla oblongata |
| Foramen | Jugular foramen |
Fiber components:
- GSA: Larynx, laryngopharynx, external ear, dura in posterior cranial fossa
- GVA: Aortic body/arch baroreceptors, esophagus, bronchi, lungs, heart, abdominal viscera (foregut + midgut)
- SA (taste): Epiglottis and pharynx
- GVE (Parasympathetic): Smooth muscle and glands in pharynx, larynx, thoracic viscera, abdominal viscera (foregut + midgut)
- BE (Motor): Palatoglossus (tongue), soft palate (except tensor veli palatini), pharynx (except stylopharyngeus), all laryngeal muscles
Key branches:
- Recurrent laryngeal nerve (RLN): All laryngeal muscles except cricothyroid; left RLN hooks around aortic arch - vulnerable in mediastinal/thyroid surgery
- Superior laryngeal nerve: External branch = cricothyroid (pitch); Internal branch = sensory to larynx above vocal cords
Clinical points:
- Hoarseness - RLN palsy (e.g., thyroid surgery, lung/mediastinal mass)
- Uvula deviates away from affected side
- Vasovagal syncope (excessive vagal tone)
CN XI - Accessory Nerve
| Feature | Detail |
|---|
| Type | Purely Motor (Branchial Efferent) |
| Function | Sternocleidomastoid (SCM) + Trapezius muscles |
| Origin | Unique - arises from C1-C5 spinal cord segments (spinal root) and exits through foramen magnum, then jugular foramen |
| Foramen | Jugular foramen |
Clinical points:
- SCM palsy: weakness turning head to contralateral side
- Trapezius palsy: drooping shoulder, winging of scapula, weakness of arm abduction above 90 degrees
- Commonly injured during posterior triangle neck surgery (lymph node biopsy)
CN XII - Hypoglossal Nerve
| Feature | Detail |
|---|
| Type | Purely Motor (GSE) |
| Function | All intrinsic and most extrinsic tongue muscles (hyoglossus, genioglossus, styloglossus) |
| Origin | Medulla oblongata |
| Foramen | Hypoglossal canal |
Clinical points:
- LMN CN XII lesion: Tongue deviates toward the side of the lesion (on protrusion), ipsilateral wasting and fasciculations
- UMN CN XII lesion: Tongue deviates away from side of lesion (no wasting/fasciculation)
- Common cause: stroke, neck dissection, nasopharyngeal carcinoma
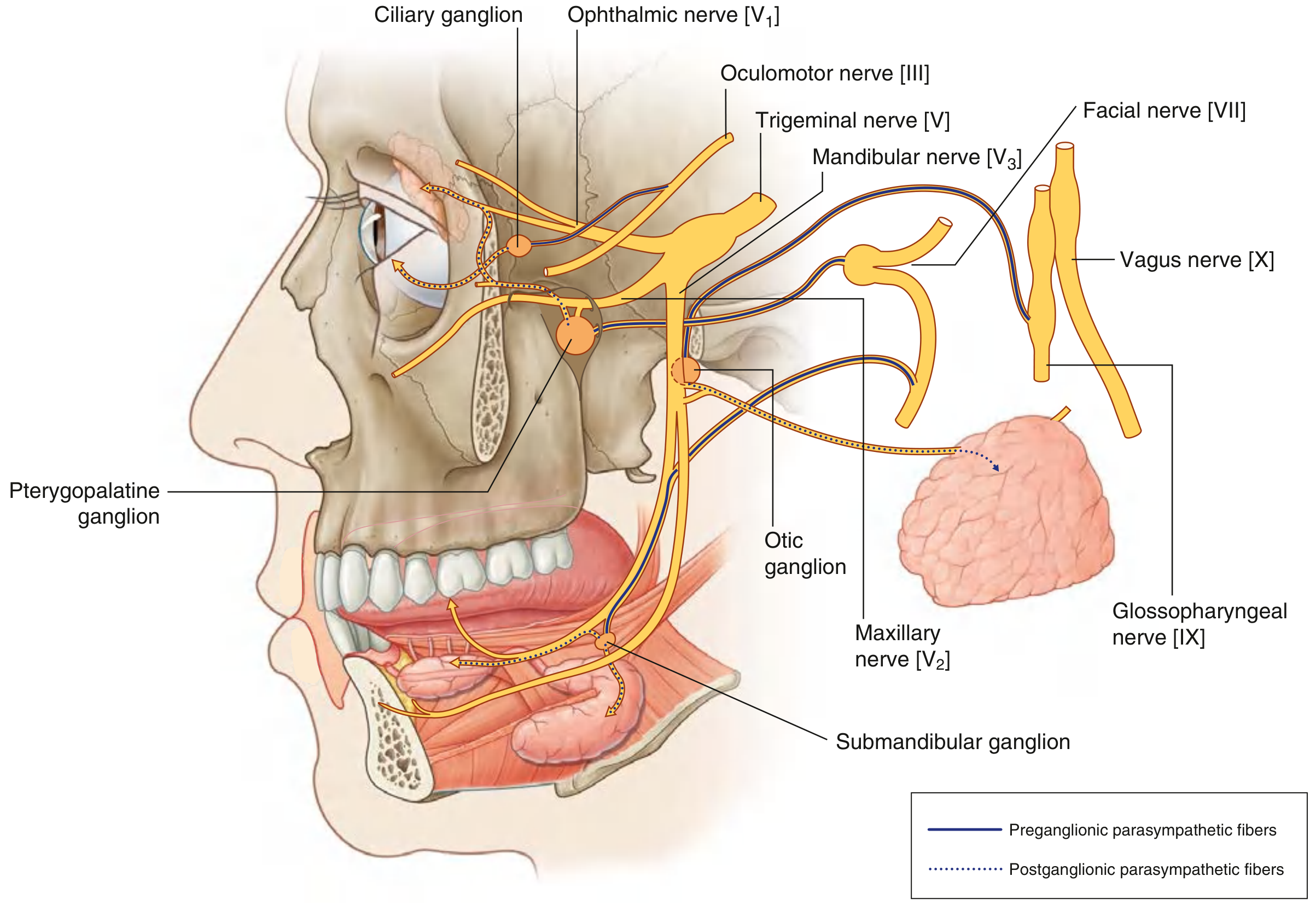
Parasympathetic Cranial Nerves (High Yield!)
Only 4 cranial nerves carry parasympathetic fibers - 3, 7, 9, 10 (remember: "3-7-9-10"):
| CN | Ganglion | Target |
|---|
| III | Ciliary ganglion | Sphincter pupillae (miosis), ciliary muscle (accommodation) |
| VII | Pterygopalatine ganglion | Lacrimal gland, nasal/palatal mucosa |
| VII | Submandibular ganglion | Submandibular + sublingual glands |
| IX | Otic ganglion | Parotid gland |
| X | Intramural ganglia | Heart, lungs, GI tract (foregut + midgut) |
Cranial Nerve Foramina - High Yield Summary
| Foramen | Cranial Nerves |
|---|
| Cribriform plate | CN I |
| Optic canal | CN II |
| Superior orbital fissure | CN III, IV, V1, VI |
| Foramen rotundum | CN V2 |
| Foramen ovale | CN V3 |
| Stylomastoid foramen | CN VII (exits here) |
| Internal acoustic meatus | CN VII (enters), CN VIII |
| Jugular foramen | CN IX, X, XI |
| Hypoglossal canal | CN XII |
Brainstem Levels - Quick Reference
| Brainstem Level | Cranial Nerves |
|---|
| Midbrain | CN III, IV |
| Pons | CN V, VI, VII, VIII |
| Medulla | CN IX, X, XI (partly), XII |
| Spinal cord (C1-C5) | CN XI (spinal root) |
Exam High-Yield Points
- CN IV is the only CN to exit dorsally and cross to innervate the contralateral muscle
- CN II is the only CN surrounded by meninges (it is technically brain tissue)
- CN XI is the only CN that partly originates from the spinal cord
- Pupil in CN III palsy: Surgical (compressive) = pupil involved; Medical (ischemic) = pupil spared
- Bell's palsy vs stroke: Bell's = forehead involved (LMN); Stroke = forehead spared (UMN)
- Tongue deviation: Always toward the lesion side in LMN CN XII palsy
- Uvula deviation: Away from the lesion side in CN X palsy
- Gag reflex: Afferent = IX, Efferent = X
- Corneal reflex: Afferent = V1, Efferent = VII
- Taste: Anterior 2/3 = CN VII (chorda tympani); Posterior 1/3 = CN IX; Epiglottis = CN X
Sources: Gray's Anatomy for Students; Bradley and Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22E
This covers everything you need for your MBBS exams, Praveen! Would you like me to go deeper on any specific nerve, cover brainstem syndromes involving cranial nerves, or do a clinical case involving cranial nerve examination?