
photo-1784094034365.jpg
Answers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Here are the complete answers to all questions in your notebook:
1. Extraocular Muscles - Superior Rectus
There are 6 extraocular muscles that move the eyeball:
| Muscle | Nerve Supply | Primary Action |
|---|---|---|
| Superior Rectus | CN III (Oculomotor) | Elevation, adduction, intorsion |
| Inferior Rectus | CN III | Depression, adduction, extorsion |
| Medial Rectus | CN III | Adduction |
| Lateral Rectus | CN VI (Abducens) | Abduction |
| Superior Oblique | CN IV (Trochlear) | Depression, abduction, intorsion |
| Inferior Oblique | CN III | Elevation, abduction, extorsion |
Superior Rectus specifically:
- Origin: Common tendinous ring (annulus of Zinn)
- Insertion: Anterior superior sclera
- Nerve: CN III (superior division)
- Actions: Elevates, adducts, and intorts the eye
- In primary position, the superior rectus is a pure elevator only when the eye is abducted 23°
(Source: Kanski's Clinical Ophthalmology - Anatomy of extraocular muscles)
2. Lacrimal Apparatus - Diagram & Diseases
Anatomy Diagram
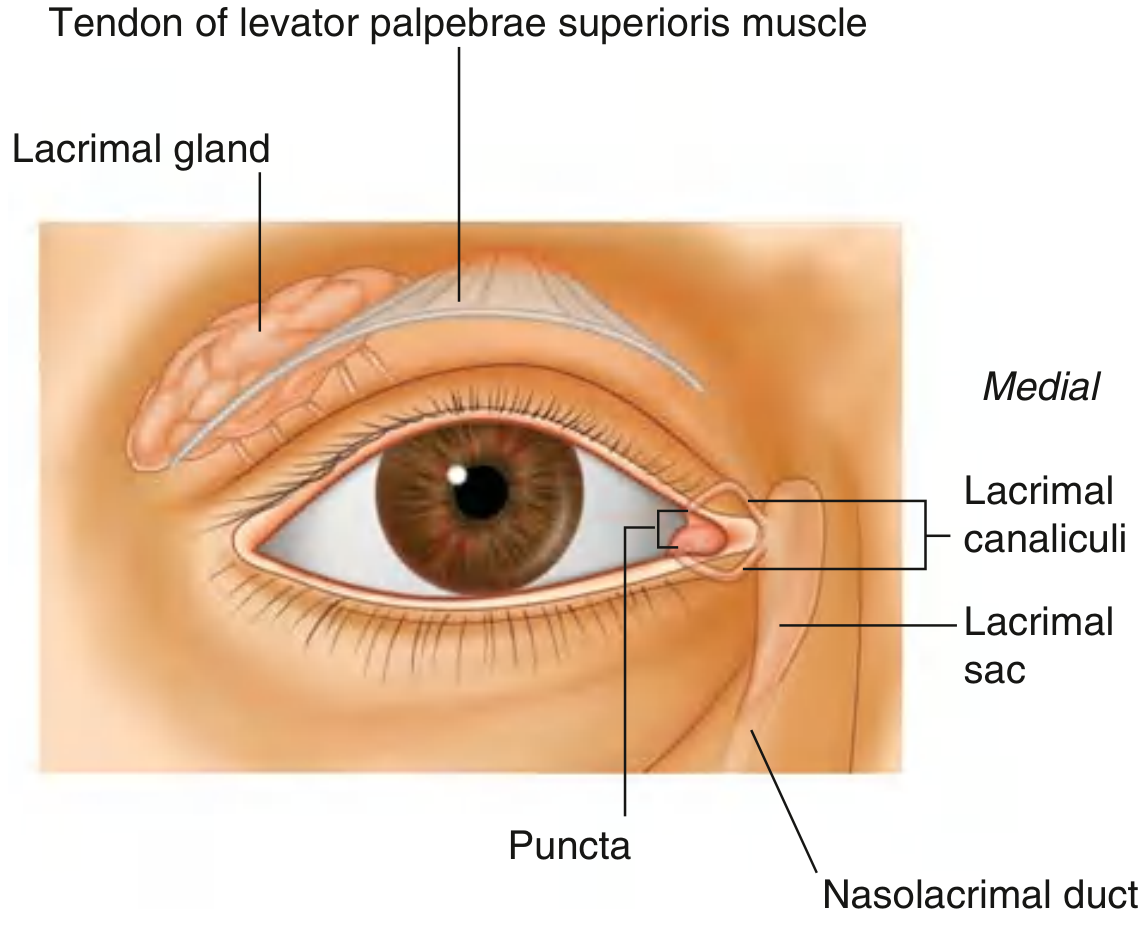
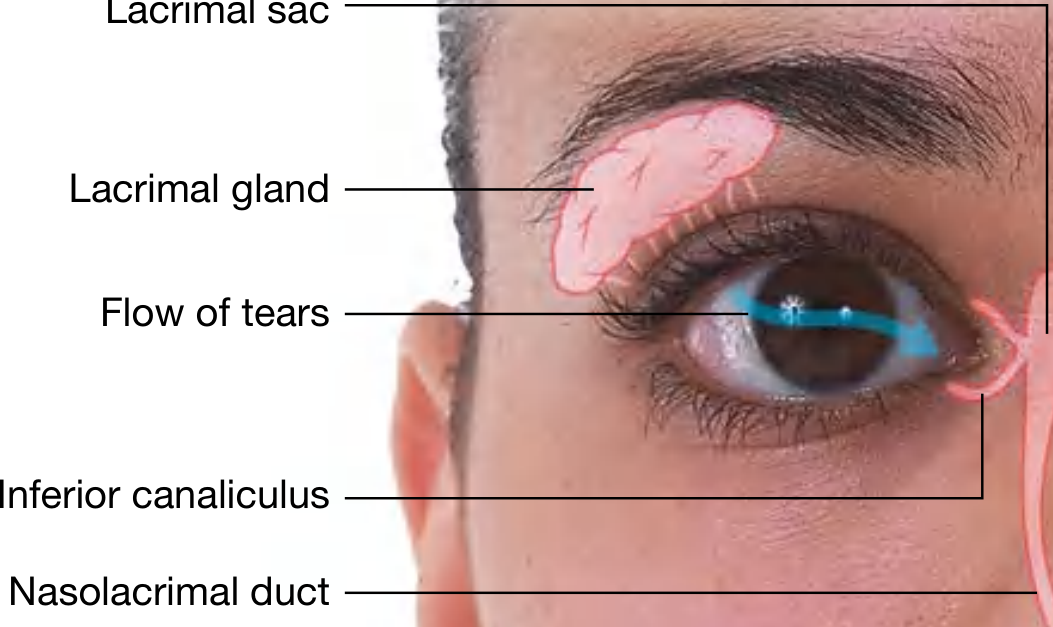
Components of the Lacrimal Apparatus
The lacrimal apparatus is involved in production, movement, and drainage of fluid from the eye surface. It consists of:
-
Lacrimal gland - located in the superolateral orbit, divided into 2 parts by the levator palpebrae superioris:
- Orbital part - larger, in the lacrimal fossa of the frontal bone
- Palpebral part - smaller, in the superolateral eyelid
- Multiple ducts drain into the lateral superior conjunctival fornix
-
Lacrimal canaliculi - one in each eyelid; tears enter via the lacrimal punctum (opening on the lacrimal papilla)
-
Lacrimal sac - lies in the lacrimal fossa on the medial orbit wall, between the anterior and posterior lacrimal crests. The orbicularis oculi (lacrimal part) dilates the sac during blinking, drawing tears in.
-
Nasolacrimal duct - drains tears from the sac into the inferior meatus of the nasal cavity
Flow of tears: Lacrimal gland → Superior conjunctival fornix → Across corneal surface (lateral to medial via blinking) → Lacrimal lake → Lacrimal puncta → Canaliculi → Lacrimal sac → Nasolacrimal duct → Nasal cavity
Diseases of the Lacrimal Apparatus
| Disease | Key Features |
|---|---|
| Dacryoadenitis | Inflammation of the lacrimal gland; causes: viral (EBV, mumps), bacterial, sarcoidosis; presents with superolateral swelling, S-shaped ptosis |
| Dry eye (Keratoconjunctivitis sicca) | Reduced tear secretion; Schirmer's test < 5 mm/5 min; associated with Sjögren's syndrome |
| Dacryocystitis | Infection of the lacrimal sac; usually due to nasolacrimal duct obstruction; presents with medial canthal swelling, epiphora, mucopurulent discharge; most common organism: Staphylococcus aureus (adults), Haemophilus influenzae (children) |
| Nasolacrimal duct obstruction (NLDO) | In neonates: usually due to imperforate Hasner valve; presents as epiphora with discharge from birth; treated with massage initially, probing if persistent |
| Canaliculitis | Chronic inflammation of canaliculus; often due to Actinomyces israelii; "pouting punctum" sign; treated with canaliculotomy + curettage |
| Epiphora | Overflow of tears; due to excess production OR obstruction to drainage |
| Lacrimal gland tumors | Benign pleomorphic adenoma (most common), adenoid cystic carcinoma (malignant, worst prognosis) |
(Source: Gray's Anatomy for Students, p. 1072; Kanski's Clinical Ophthalmology 10th ed.)
3. Examination of Eyelids & Diseases of the Eyelid
Examination of the Eyelid
Systematic inspection includes:
- Position - ptosis, lid retraction, entropion, ectropion
- Lid margin - look for scaling, crusting, lash abnormalities (trichiasis, madarosis)
- Meibomian gland orifices - blocked or inspissated?
- Eversion of upper lid - to examine tarsal conjunctiva for papillae, follicles, foreign bodies
- Palpation - for nodules (chalazion, cyst), pre-auricular lymph nodes in infection
Diseases of the Eyelid
| Disease | Key Features |
|---|---|
| Blepharitis | Most common eyelid disease; anterior (staphylococcal/seborrhoeic - affects lash base) vs posterior (meibomian gland dysfunction); chronic, bilateral; managed with lid hygiene, warm compresses |
| Chalazion (Meibomian cyst) | Chronic lipogranuloma of meibomian gland; painless, firm lid nodule; treated with warm compresses, incision and curettage |
| Hordeolum (Stye) | Acute abscess; external (Zeis gland) or internal (meibomian gland); painful, red, localized; treated with warm compresses, topical antibiotics |
| Entropion | Inward turning of lid margin; causes corneal abrasion/ulceration; involutional (senile) is most common type |
| Ectropion | Outward turning of lid; causes exposure keratopathy and epiphora; involutional most common |
| Ptosis | Drooping of upper eyelid; classified as myogenic, neurogenic (CN III palsy, Horner's), aponeurotic (senile), mechanical |
| Trichiasis | Misdirected lashes irritating the cornea; causes: trachoma, blepharitis; treated with epilation, electrolysis |
| Xanthelasma | Yellow plaques at medial canthus; associated with hyperlipidaemia |
| Basal cell carcinoma (BCC) | Most common malignant eyelid tumor; lower lid most common; rodent ulcer appearance; treated with surgical excision |
| Squamous cell carcinoma (SCC) | Less common; metastasizes via lymphatics |
| Sebaceous gland carcinoma | Arises from meibomian glands; can masquerade as chalazion; high mortality |
| Molluscum contagiosum | Pearly umbilicated nodule; can cause toxic follicular conjunctivitis |
(Source: Kanski's Clinical Ophthalmology 10th ed.; Cummings Otolaryngology)
4. Examination of Conjunctiva & Diseases of the Conjunctiva
Anatomy of the Conjunctiva
The conjunctiva is a transparent mucous membrane divided into:
- Palpebral conjunctiva - lines inner eyelids, firmly attached to tarsal plate; tarsal vessels are vertically oriented
- Fornical conjunctiva - loose and redundant (upper and lower fornices)
- Bulbar conjunctiva - covers anterior sclera, continuous with corneal epithelium at the limbus
The palisades of Vogt are radial ridges at the limbus - the reservoir of corneal stem cells.
Histology: Non-keratinizing epithelium with mucus-secreting goblet cells (most dense in fornices). Stroma contains accessory lacrimal glands of Krause (fornix) and Wolfring (upper border of tarsus). Conjunctiva-associated lymphoid tissue (CALT) mediates ocular surface immunity.
Examination of Conjunctiva
- Inspection - redness pattern: conjunctival injection (bacterial) vs ciliary injection (iridocyclitis)
- Discharge type - watery (viral/allergic), mucoid (chronic allergic/dry eye), mucopurulent (bacterial), purulent (gonococcal)
- Papillae - vascular tufts with fibrovascular core; seen in bacterial, allergic conjunctivitis; giant papillae in VKC
- Follicles - lymphoid aggregates without vascular core; seen in viral, chlamydial conjunctivitis
- Chemosis - conjunctival oedema (translucent swelling)
- Membranes/pseudomembranes - in severe conjunctivitis (Stevens-Johnson syndrome, diphtheria)
- Subconjunctival hemorrhage - petechial (viral) vs diffuse (bacterial)
Diseases of the Conjunctiva
Infective
| Disease | Cause | Features |
|---|---|---|
| Bacterial conjunctivitis | Staphylococcus, Streptococcus, H. influenzae | Mucopurulent discharge, conjunctival hyperemia |
| Hyperacute bacterial (gonococcal) | Neisseria gonorrhoeae | Profuse purulent discharge, rapid onset, corneal perforation risk |
| Viral conjunctivitis | Adenovirus (most common), Herpes simplex | Watery discharge, follicles, preauricular lymphadenopathy |
| Chlamydial (trachoma) | Chlamydia trachomatis | Leading infectious cause of blindness worldwide; follicles → scarring → pannus → blindness |
| Inclusion conjunctivitis | Chlamydia trachomatis (serotypes D-K) | Chronic follicular conjunctivitis in sexually active adults |
Allergic
| Disease | Features |
|---|---|
| Seasonal allergic conjunctivitis | IgE-mediated; itching, watery discharge, hyperemia |
| Vernal keratoconjunctivitis (VKC) | Young males; shield ulcer, cobblestone giant papillae on upper tarsal plate, Horner-Trantas dots at limbus |
| Atopic keratoconjunctivitis (AKC) | Adults with atopic dermatitis; chronic, can cause scarring |
| Giant papillary conjunctivitis | Contact lens-related; giant papillae on upper tarsus |
Cicatrizing
| Disease | Features |
|---|---|
| Ocular cicatricial pemphigoid | Autoimmune; progressive subconjunctival fibrosis, symblepharon (adhesion between bulbar and palpebral conjunctiva), dry eye, corneal scarring |
| Stevens-Johnson syndrome/TEN | Drug-induced; pseudomembranes, symblepharon, severe ocular surface disease |
| Trachoma | Chronic scarring; entropion, trichiasis, corneal opacification (blinding trachoma) |
Degenerative
| Disease | Features |
|---|---|
| Pinguecula | Yellowish-white deposit on bulbar conjunctiva at 3 or 9 o'clock; elastotic degeneration of stroma |
| Pterygium | Triangular fibrovascular tissue growing from conjunctiva onto cornea (nasal side); associated with UV exposure; Stocker's line (iron deposit at leading edge) |
| Concretions | Calcium deposits in palpebral conjunctiva; can cause foreign body sensation |
| Conjunctivochalasis | Redundant bulbar conjunctiva; causes epiphora and foreign body sensation |
| Subconjunctival hemorrhage | Spontaneous or traumatic; usually resolves in 2-3 weeks |
(Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th edition; Gray's Anatomy for Students)
Summary of the notebook topics answered:
- Extraocular muscles (6 muscles, actions, nerve supply) - Superior Rectus: CN III, elevation/adduction/intorsion
- Lacrimal apparatus diagram and diseases (dacryoadenitis, dacryocystitis, NLDO, canaliculitis, dry eye)
- Eyelid diseases (blepharitis, chalazion, stye, entropion, ectropion, ptosis, lid tumors)
- Conjunctiva examination and diseases (infective, allergic, cicatrizing, degenerative)
This is a shared conversation. Sign in to Orris to start your own chat.