Severe oesophagitis causes and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"oesophagitis" OR "esophagitis" management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive data from multiple authoritative textbooks. Here is a thorough, well-structured answer:
Severe Oesophagitis: Causes and Management
Overview
Oesophagitis is inflammation of the oesophageal mucosa with a spectrum from mild erythema to severe ulceration, haemorrhage, and stricture. Severe cases (grade 3–4 by the Savary-Miller system) carry a significant risk of upper GI bleeding, perforation, and long-term malignant transformation.
Endoscopic image — erythema and ulceration of the distal oesophagus in severe oesophagitis (GERD):
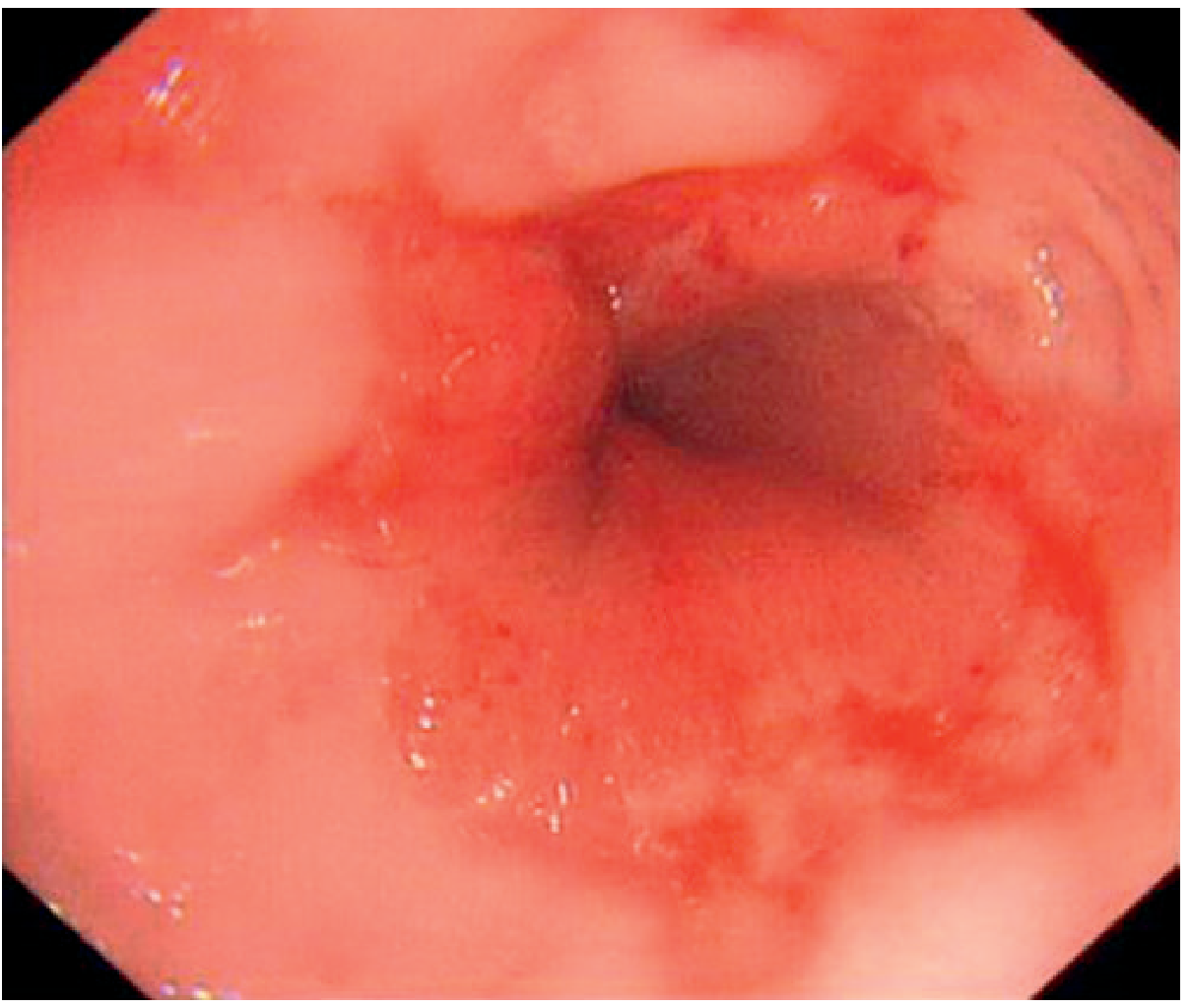
— Grainger & Allison's Diagnostic Radiology
Causes of Severe Oesophagitis
1. Gastro-oesophageal Reflux Disease (GERD) — Most Common
GERD is the most common cause of oesophagitis overall and of overt upper GI bleeding from oesophagitis. The primary mechanism is inappropriate relaxation of the lower oesophageal sphincter (LES), allowing reflux of gastric acid, pepsin, and bile acids. Factors reducing LES tone include:
- Drugs: nitrates, calcium channel blockers, anticholinergics, albuterol, progesterone
- Dietary: fatty meals, caffeine, chocolate, peppermint, alcohol
- Mechanical: obesity, pregnancy, hiatal hernia (increased intra-abdominal pressure)
- Motility disorders: achalasia, scleroderma, diabetic gastroparesis
Pathological progression: repeated acid exposure → thinning of squamous epithelium → PMN infiltration → erosions → ulceration → scarring → stricture. The most severe histological consequence is Barrett metaplasia (columnar replacement of squamous epithelium), which carries a 30-fold increased risk of adenocarcinoma. — Rosen's Emergency Medicine; Robbins & Kumar Basic Pathology
Risk factors for severe/bleeding GERD-oesophagitis: grade 3–4 Savary-Miller staging, cirrhosis, poor performance status, anticoagulant therapy. Notably, only 38% of patients with bleeding oesophagitis report heartburn. — Sleisenger & Fordtran's GI & Liver Disease
2. Infectious Oesophagitis
Primarily in immunocompromised patients (HIV/AIDS, haematological malignancies, transplant recipients, high-dose steroid/chemotherapy users). Occasionally in immunocompetent individuals with underlying oesophageal disease or inhaled steroid use.
| Organism | Features | Endoscopic/Histo appearance |
|---|---|---|
| Candida | Most common infectious cause; also in oesophageal stasis (e.g. achalasia) | Adherent grey-white pseudomembranes; large/linear mural plaques on fluoroscopy |
| Herpes simplex (HSV) | Punched-out ulcers; multinucleate cells with nuclear inclusions at ulcer edge | Punched-out distal ulcers |
| Cytomegalovirus (CMV) | Shallower ulcers; nuclear + cytoplasmic inclusions in endothelial/stromal cells | Large ovoid/diamond-shaped ulcers |
| HIV | Idiopathic giant ulcers | Large ulcers |
Classic symptom: odynophagia localised to a discrete substernal area. Pain may be so severe patients refuse oral intake. — Goldman-Cecil Medicine; Robbins & Kumar
Endoscopic and histological appearances of HSV and CMV oesophagitis:
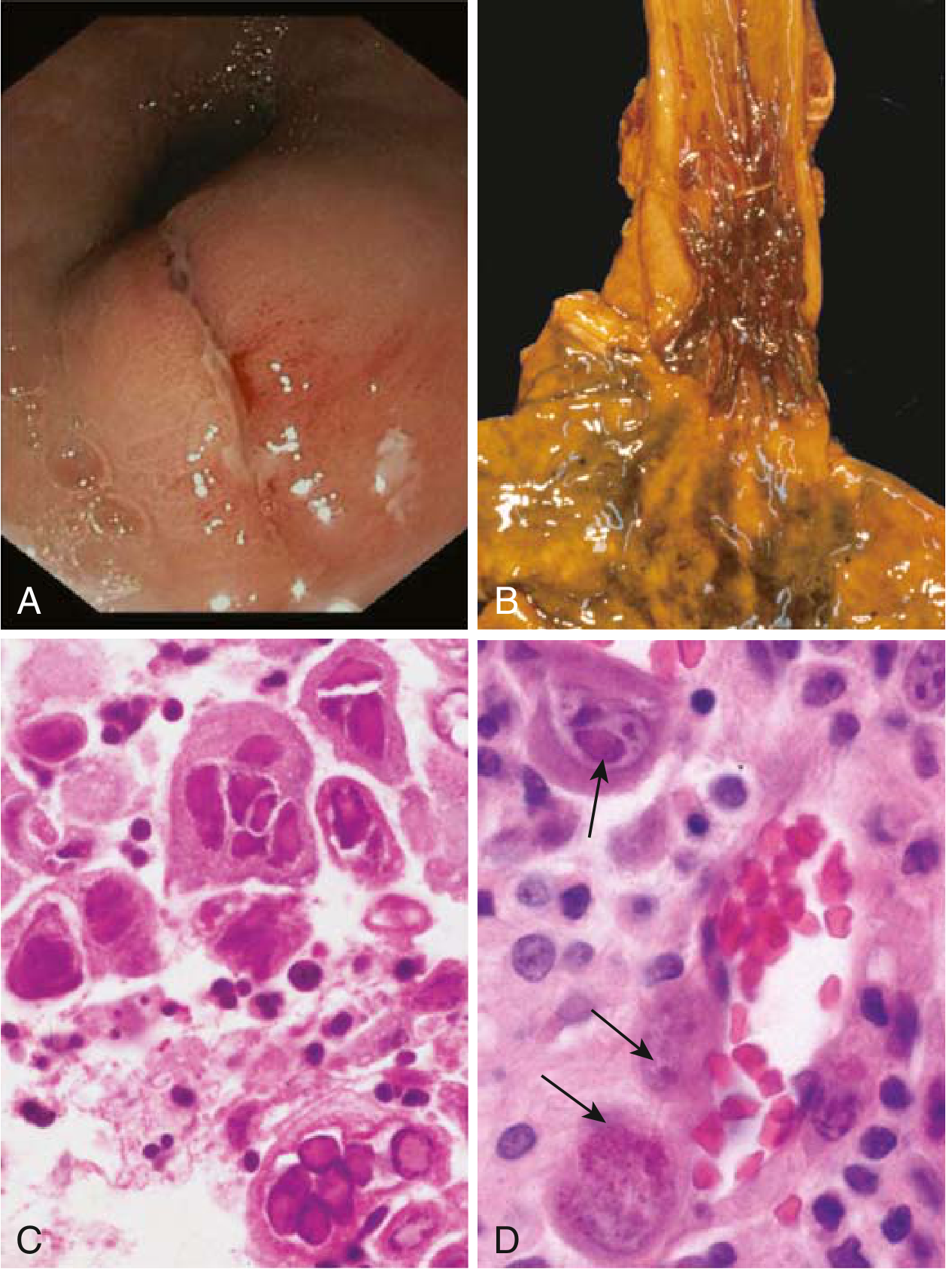
A: Herpetic white exudates endoscopically. B: Multiple herpetic ulcers (post-mortem). C: HSV multinucleate squamous cells with nuclear inclusions. D: CMV inclusions in endothelial cells (arrows). — Robbins & Kumar Basic Pathology
3. Eosinophilic Oesophagitis (EoE)
An immune/allergic condition driven by food and aeroallergens triggering chronic eosinophilic infiltration. Prevalence ~0.5–1 per 1,000. >50% of patients have atopic co-morbidities (asthma, eczema). Genetic predisposition in ~50% of affected children.
- Adults: solid food dysphagia, food impaction, chest pain, risk of Boerhaave syndrome
- Children: failure to thrive, vomiting, abdominal pain
- Endoscopy: linear furrowing, white exudates, multiple rings (corrugated/ringed appearance)
- Diagnosis: ≥15 eosinophils per high-power field on biopsy, after excluding other causes of eosinophilia — Goldman-Cecil Medicine; Rosen's EM
4. Pill-Induced Oesophagitis
Occurs when medications dissolve at the oesophageal wall rather than passing into the stomach (taking pills without adequate water, while recumbent, in anatomically narrowed oesophagi). Common culprits:
- Doxycycline, tetracycline → small shallow ulcers
- NSAIDs, aspirin
- Potassium chloride, alendronate (bisphosphonates) → large ulcers and strictures (more damaging)
- Iron salts
Presentation: sudden onset retrosternal pain + odynophagia, often without prior oesophageal disease, hours after tablet ingestion. — Rosen's EM; Robbins & Kumar
5. Chemical/Caustic and Other Causes
- Caustic ingestion: corrosive acids or alkalis can cause severe transmural necrosis
- Radiation oesophagitis: cytotoxic chemotherapy, radiotherapy, graft-versus-host disease — causes ulceration + ischaemic injury via blood vessel damage
- Alcohol and heavy smoking
- Immune checkpoint inhibitor therapy — increasingly recognised in oncology patients
- Stress-related mucosal injury in critically ill patients (ICU, mechanical ventilation >48 hours, severe coagulopathy)
Management of Severe Oesophagitis
1. GERD / Reflux Oesophagitis
Lifestyle modification (adjunctive, not sufficient alone):
- Avoid precipitants: caffeine, alcohol, chocolate, fatty/acidic/spicy foods
- Weight loss and head-of-bed elevation (only two lifestyle measures with strong evidence)
- Smoking cessation; avoid recumbent position for several hours post-meal
Medical therapy (mainstay):
| Agent | Dose | Role |
|---|---|---|
| PPIs (first-line) | Esomeprazole/Omeprazole 20–40 mg qd; Lansoprazole 30 mg qd; Pantoprazole 40 mg qd | Superior to H2 blockers for healing mucosal damage and symptom resolution |
| H2 receptor antagonists | Famotidine 20–40 mg bid; Cimetidine 800 mg bid | Acceptable for mild–moderate GERD; less effective for severe disease |
| Sucralfate | 1 g every 6 hours | Mucosal protectant; adjunct in refractory cases; safe in pregnancy |
For severe erosive oesophagitis (grade 3–4, or bleeding):
- High-dose PPI is the mainstay of treatment
- Treat for 8–12 weeks (daily PPI), then repeat endoscopy to exclude Barrett's oesophagus
- EGD is essential for diagnosis but endoscopic haemostasis is generally not indicated unless a focal ulcer with stigmata of recent haemorrhage (SRH) is found — Sleisenger & Fordtran; Mulholland & Greenfield's Surgery
For Barrett's oesophagus identified at follow-up: continuous PPI; surveillance endoscopy every 2 years. — Grainger & Allison's Diagnostic Radiology
Surgical management (anti-reflux surgery, e.g. Nissen fundoplication): considered for refractory or recurrent severe disease, or in patients intolerant of long-term PPIs.
2. Infectious Oesophagitis
| Organism | Treatment |
|---|---|
| Candida | Fluconazole oral (first-line); IV antifungals (e.g. caspofungin) for severe/refractory cases |
| HSV (immunocompromised) | Acyclovir 400 mg PO 5×/day × 7–14 days; or 5–10 mg/kg IV tid × 10–14 days; famciclovir 500 mg tid; valacyclovir 1 g tid |
| CMV | Ganciclovir 5 mg/kg IV bid; or foscarnet 60 mg/kg IV tid (or 90 mg/kg IV bid) |
| HSV (immunocompetent) | Self-limiting in 1–2 weeks; antivirals optional |
Endoscopy with biopsy and brushings is critical for organism identification. Hospitalisation required if the patient cannot tolerate oral intake or the organism cannot be identified. Adjunct symptom relief: antacids, topical anaesthetics, sucralfate. — Rosen's EM; Goldman-Cecil
3. Eosinophilic Oesophagitis
Escalating approach:
- PPI trial (first step to exclude GERD-related eosinophilia)
- Dietary elimination: empiric 1–2–4–6 food elimination diet (eliminating cow's milk, soy, wheat, eggs, peanuts/tree nuts, seafood); elemental diet for severe disease
- Topical corticosteroids:
- Swallowed fluticasone 880 µg twice daily
- Budesonide orodispersible tablets 0.5 mg twice daily
- Budesonide suspension 1 mg twice daily
- Achieve remission in ~75%; relapse rate up to 95% on stopping → often requires chronic therapy
- Dupilumab 300 mg SC weekly for 12 weeks — biologic option for refractory disease
- Endoscopic dilation for established strictures — Goldman-Cecil Medicine
4. Pill-Induced Oesophagitis
- Stop offending agent
- Antacids/PPIs to reduce further mucosal damage
- Symptoms may take up to 6 weeks to resolve
- Prevention: take pills with ≥120 mL (4 oz) of water; remain upright for several minutes post-ingestion; avoid problematic drugs in patients with oesophageal disease or those who are bedridden — Rosen's EM
5. Radiation/Chemical Oesophagitis
- Primarily supportive
- Nutritional support (parenteral or enteral)
- Topical anaesthetics, sucralfate for mucosal protection
- Treat secondary infections
- In severe complications (haemorrhage, stricture, perforation): endoscopic or surgical intervention
6. Complications and When to Escalate
| Complication | Action |
|---|---|
| Significant upper GI haemorrhage | EGD for diagnosis; IV PPI; endoscopic haemostasis if focal SRH; surgery rarely needed |
| Oesophageal stricture | Endoscopic dilation |
| Barrett's oesophagus | Endoscopic surveillance; ablative therapy (RFA) for dysplasia |
| Cannot eat/drink | Admission for IV fluids; IV PPI; consider parenteral nutrition |
| Cirrhosis + severe oesophagitis bleeding | High rebleeding (17%) and mortality (33%) — intensive management required |
Key sources: — Sleisenger & Fordtran's Gastrointestinal and Liver Disease | — Rosen's Emergency Medicine | — Goldman-Cecil Medicine | — Robbins & Kumar Basic Pathology | — Mulholland & Greenfield's Surgery | — Grainger & Allison's Diagnostic Radiology
Severe oesophagitis causes and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"esophagitis" AND management
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.