histology of endometrial
Reading File
Finding Sources
Finding Sources
Searching Images
endometrium histology microscopy glands stroma
Finding Sources
Finding Sources
Searching Images
proliferative endometrium histology tubular glands
Reading File
Reading File
Searching Images
secretory endometrium subnuclear vacuoles saw-tooth glands
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of endometrial histology, drawn from Junqueira's Basic Histology (17e) and Histology: A Text and Atlas (Ross & Pawlina).
Histology of the Endometrium
General Structure
The endometrium is the inner mucosal lining of the uterus. It consists of:
- Surface epithelium — simple columnar epithelium with both ciliated and secretory cells
- Lamina propria (stroma) — cellular connective tissue rich in fibroblasts, ground substance, and non-bundled type III collagen
- Uterine glands — tubular glands lined by columnar secretory epithelium that penetrate the full thickness of the endometrium
Two Concentric Layers
| Layer | Location | Characteristics |
|---|---|---|
| Stratum Basale (Basal layer) | Adjacent to myometrium | Highly cellular stroma; contains deep basal ends of glands and lower portions of spiral arteries; not shed during menstruation |
| Stratum Functionale (Functional layer) | Superficial | Spongier stroma, rich in ground substance; contains most of the gland length and surface epithelium; shed cyclically during menses |
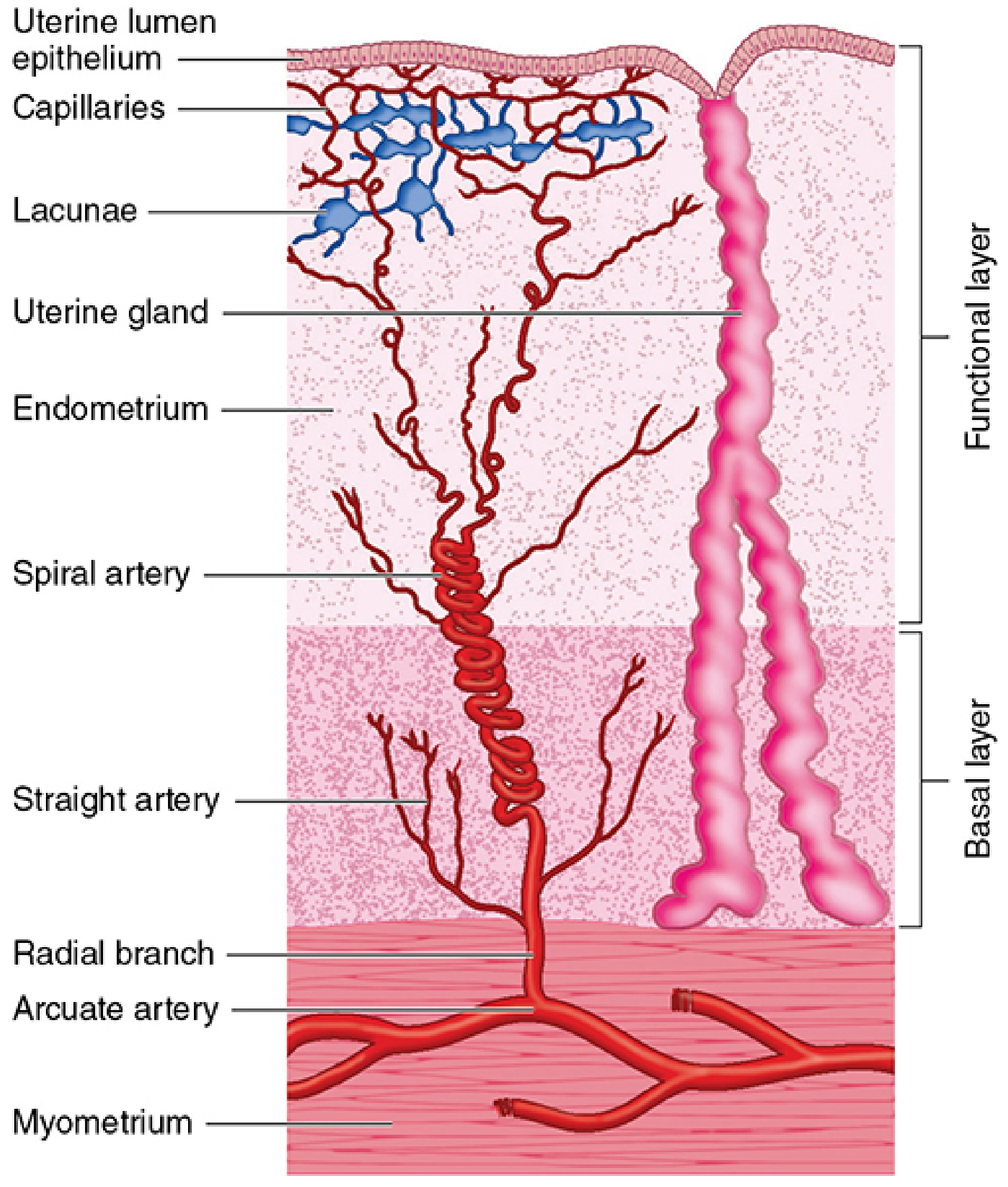
Blood Supply (Histologically Important)
Arcuate arteries in the myometrium give off radial arteries that enter the endometrium and divide into:
- Straight arteries — supply only the stratum basale
- Spiral arteries — coiled, progesterone-sensitive; supply the stratum functionale; their vasoconstriction triggers menstrual shedding
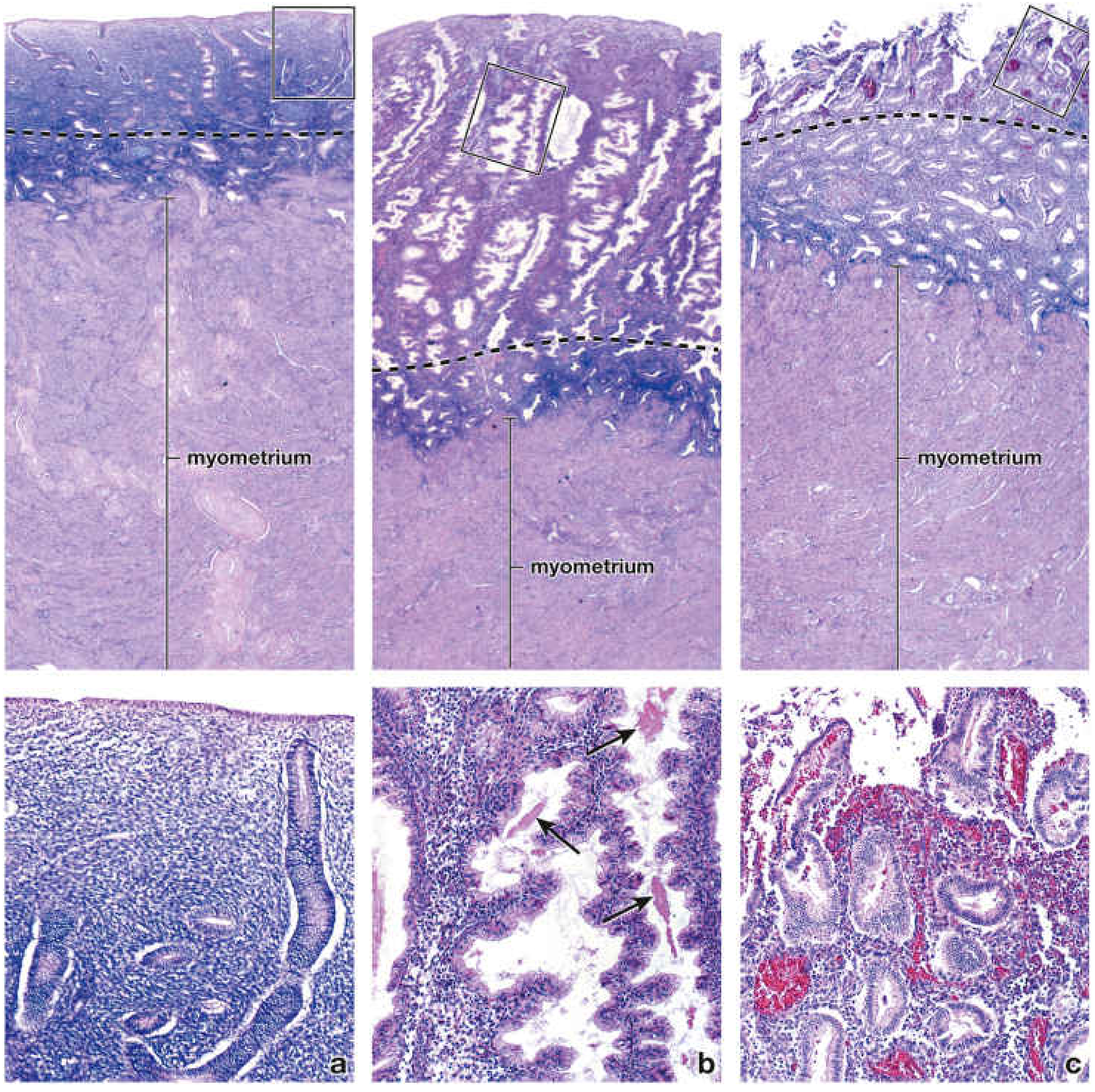
Cyclic Histological Changes
The endometrium undergoes three cyclic phases driven by ovarian hormones:
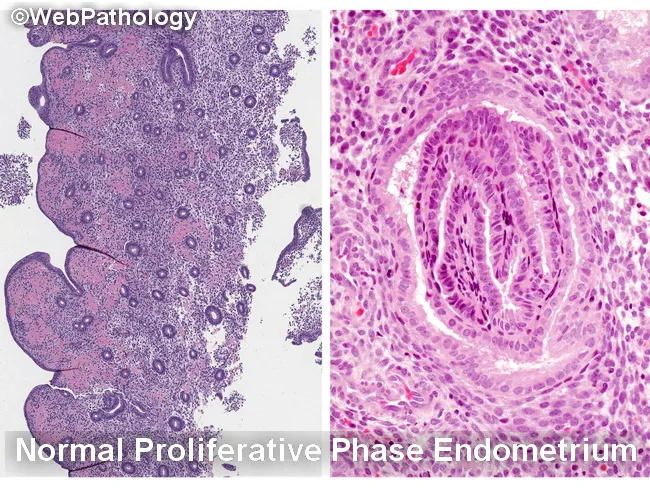
1. Proliferative Phase (Days 5–14)
Driven by estrogen from growing follicles
- Endometrial thickness: ~3 mm
- Glands: straight to slightly wavy, narrow lumina, pseudostratified columnar epithelium with mitoses
- Stroma: compact, cellular with active mitoses
- Spiral arteries: only mildly coiled, do not reach upper third of endometrium
- Glycogen accumulates in basal cytoplasm of gland cells (appears empty on H&E after fixation)
2. Secretory Phase (Days 15–28)
Driven by progesterone from corpus luteum
- Endometrial thickness: up to 5–6 mm
- Glands: corkscrew/saw-tooth shaped with sacculated, dilated lumina filled with glycogen-rich mucoid secretion
- Subnuclear vacuoles appear early (day 17–18) — hallmark of early secretory phase
- Stroma: edematous; later undergoes predecidual change (enlarged pale stromal cells rich in glycogen)
- Spiral arteries: markedly elongated, tightly coiled, extend nearly to surface
- Mitoses are rare

3. Menstrual Phase (Days 1–4)
Triggered by decline in estrogen and progesterone
- Spiral artery vasoconstriction → ischemia of stratum functionale
- Glands stop secreting; stroma loses edema
- Rupture of blood vessels → extravasation, necrosis, and sloughing of the functional layer
- Only the stratum basale persists
- Average blood loss: 35–50 mL over ~5 days
Comparative Histology at a Glance
| Feature | Proliferative | Secretory | Menstrual |
|---|---|---|---|
| Thickness | ~3 mm | 5–6 mm | Thinning |
| Gland shape | Straight/wavy | Corkscrew/sacculated | Degenerating |
| Gland lumen | Narrow | Wide, filled with secretion | Collapsing |
| Epithelium | Tall, pseudostratified, mitoses | Secretory, vacuolated, no mitoses | Necrotic |
| Stroma | Compact, mitotic | Edematous → predecidual | Necrotic/hemorrhagic |
| Spiral arteries | Mildly coiled | Tightly coiled | Constricted → rupture |
| Hormone driver | Estrogen | Progesterone | Withdrawal of both |
Clinical Correlations
- Anovulatory cycles: No corpus luteum → no progesterone → endometrium stays in prolonged proliferative phase → can lead to endometrial hyperplasia
- Endometrial dating: Histological appearance of the glands and stroma can be used to assess cycle day and diagnose luteal phase defects
- Endometriosis: Viable endometrial cells reflux through the tubes and implant on pelvic structures, responding to cyclic hormonal changes
- Decidualization: If implantation occurs, stromal cells transform into large, pale decidual cells rich in glycogen under sustained progesterone stimulation
Sources: Junqueira's Basic Histology, 17e, p. 1133–1135 | Histology: A Text and Atlas (Ross & Pawlina), pp. 2246–2249
Histological features of Squamous cell carcinoma
Finding Sources
Finding Sources
Searching Images
squamous cell carcinoma histology keratin pearls H&E
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Searching Images
squamous cell carcinoma well differentiated moderately poorly differentiated grading comparison
Loading Image
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.