
Answers
Reading File
Finding Sources
Searching the Web
acute epiglottitis AETCOM patient counselling intubation tracheostomy conservative management
Reading File
Reading File
The image shows a question asking about AETCOM (Attitudes, Ethics and Communication) — specifically, what to explain to a patient with Acute Epiglottitis regarding three points. Here is a complete model answer:
AETCOM – Patient Counselling in Acute Epiglottitis (5 marks)
What to Explain to the Patient/Guardian
1. Necessity of Conservative Management
- Acute epiglottitis is a serious, potentially life-threatening infection causing swelling of the epiglottis (the flap of tissue that covers the windpipe).
- Initial conservative management includes IV antibiotics (commonly ceftriaxone or augmentin), corticosteroids to reduce swelling, humidified oxygen, and keeping the patient calm and upright (sitting, leaning forward — the "tripod" position).
- The patient must remain strictly monitored in a hospital setting, ideally in an ICU or high-dependency unit, because the airway can deteriorate without warning.
- Explain that disturbing the patient (blood draws, lying flat, throat examination without preparation) can trigger total airway obstruction — so full cooperation is essential.
2. Necessity of Intubation / Tracheostomy if Conservative Management Fails
- If breathing worsens despite medical treatment, securing the airway becomes mandatory — this is not optional.
- Endotracheal intubation is the first-line airway intervention and is performed in the operating theatre under inhalation anaesthesia with a surgeon on standby.
- If intubation is not possible (due to severe supraglottic swelling and distorted anatomy), an emergency tracheostomy (surgical airway through the neck) will be performed to bypass the obstruction and save the patient's life.
- The family/patient must give informed consent for both procedures in advance, as there may be no time to obtain consent once deterioration begins.
- These procedures carry their own risks (bleeding, infection, voice change, tracheal injury), which must be disclosed.
3. Possibility of Worsening — Even Death — Before, During, or After the Procedure
- Acute epiglottitis carries a real risk of sudden, fatal airway obstruction even in patients who appear stable.
- The patient or family must understand that deterioration can be rapid and unpredictable — from mild stridor to complete obstruction within minutes.
- Even with the best care, death can occur:
- Before the procedure — if the airway closes before the team can act
- During the procedure — due to laryngospasm, failed intubation, or cardiac arrest under anaesthesia
- After the procedure — due to complications like aspiration, secondary pneumonia, or sepsis
- This honest disclosure is essential for informed consent and allows the family to prepare.
- Reassure them that the medical team will make every effort, and that outcomes are generally good when treatment begins early.
Communication Approach (AETCOM Principles)
| Principle | Application |
|---|---|
| Empathy | Acknowledge fear; use simple, non-technical language |
| Honesty | Disclose real risks including death without causing panic |
| Autonomy | Obtain informed consent for all procedures in advance |
| Non-maleficence | Explain why certain actions (e.g. throat exam without preparation) are avoided |
| Beneficence | Emphasise that all decisions are made in the patient's best interest |
— Barash Clinical Anesthesia 9e; Rosen's Emergency Medicine 10e
Diagnosed
Asking for Preferences
Finding Sources
Searching the Web
acute epiglottitis clinical features diagnosis signs symptoms 4D drooling dysphonia dysphagia dyspnoea
Reading File
Reading File
Clinical Features / Diagnosis of Acute Epiglottitis
Classic Presentation — The "4 D's"
| D | Feature |
|---|---|
| Drooling | Cannot swallow due to severe pain and swelling |
| Dysphagia | Painful, difficult swallowing |
| Dysphonia | Muffled, "hot-potato" voice (NOT hoarse) |
| Dyspnoea | Respiratory distress, inspiratory stridor |
A 5th is sometimes added: Distress (anxiety, agitation, toxic appearance).
History
- Acute, rapid onset — hours, not days
- High fever (typically >38.5°C)
- Severe sore throat out of proportion to pharyngeal findings on exam
- No cough (important distinguishing feature from croup)
- Preceding upper respiratory symptoms usually absent
Clinical Signs on Examination
- Tripod / sniffing position — patient sits upright, leans forward, jaw jutted out, neck extended — this maximises airway patency and is almost pathognomonic
- Drooling (cannot swallow secretions)
- Toxic, anxious appearance
- Inspiratory stridor (may be absent early)
- Suprasternal / intercostal retractions in severe cases
- Cyanosis — late, pre-terminal sign
- No cough, no hoarseness (unlike croup/laryngitis)
⚠️ Do NOT attempt direct throat examination in the ED or clinic without full airway readiness — stimulating the hypopharynx can trigger total laryngospasm and death.
Investigations
| Investigation | Finding |
|---|---|
| Lateral soft tissue X-ray neck | "Thumbprint sign" — swollen epiglottis + thickened aryepiglottic folds (see image below) |
| Blood culture | Positive in ~25% (Hib, Streptococcus, Staph aureus) |
| FBC | Leukocytosis (elevated WBC) |
| Direct laryngoscopy | Swollen, cherry-red epiglottis — only in controlled OR/ICU setting |
Radiological Sign
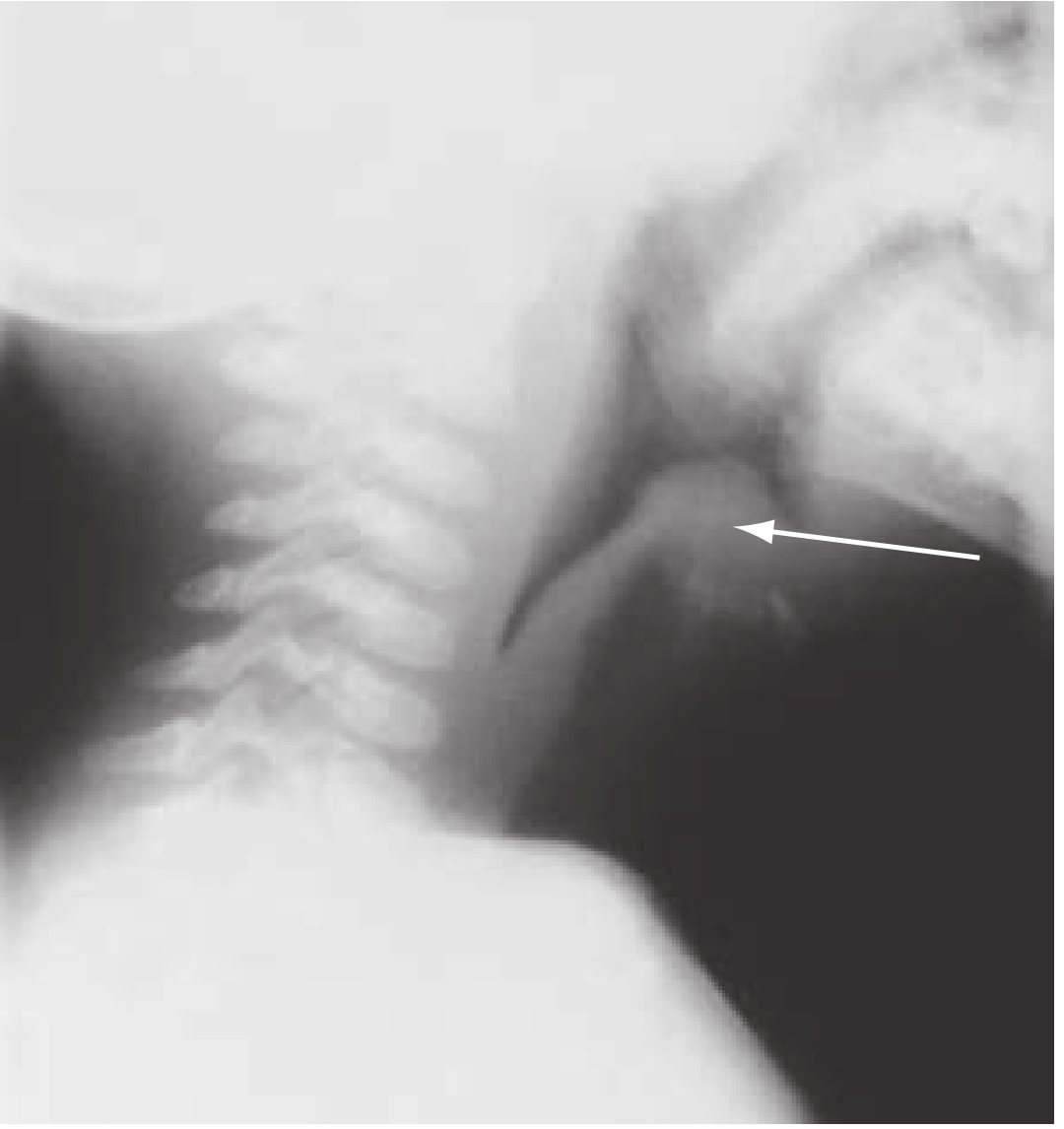
Lateral neck X-ray showing the "thumbprint sign" — the swollen epiglottis (arrow) and thickened aryepiglottic folds — Rosen's Emergency Medicine
Differential Diagnosis at a Glance
| Condition | Key Distinguishing Feature |
|---|---|
| Croup | Barky cough, steeple sign on X-ray, no drooling |
| Bacterial tracheitis | Croup that fails treatment, fever, toxicity |
| Retropharyngeal abscess | Torticollis, neck stiffness, no positional preference |
| Anaphylaxis | Trigger, urticaria, multi-system involvement |
| Peritonsillar abscess | Trismus, uvular deviation, unilateral |
— Rosen's Emergency Medicine 10e; Barash Clinical Anesthesia 9e
Medical tracheotomy
Finding Sources
Searching the Web
tracheotomy procedure steps indications complications anatomy surgical technique
Reading File
Reading File
Finding Sources
Searching Images
tracheotomy surgical technique anatomy steps
Reading File
Medical Tracheotomy — Complete Overview
Terminology
| Term | Meaning |
|---|---|
| Tracheotomy | Incision into the trachea (the act/procedure) |
| Tracheostomy | A formalised, epithelialised stoma between the trachea and the skin surface (permanent opening) |
These terms are often used interchangeably in clinical practice.
Indications
1. Airway obstruction at or above the larynx
- Acute epiglottitis, Ludwig's angina, head & neck tumours, bilateral vocal cord paralysis, severe facial/neck trauma, foreign body, anaphylaxis
2. Inability to clear secretions
- Neurological conditions — stroke, GBS, MND, cervical spine injury
- Copious pulmonary secretions requiring repeated suctioning
3. Prolonged mechanical ventilation
- When intubation is expected to last >7–10 days (reduces subglottic trauma and patient discomfort)
4. Reduction of dead space / airway resistance
- Pulmonary insufficiency — reduces anatomical dead space by ~150 mL
- Facilitates weaning from ventilator
5. Other
- Severe obstructive sleep apnoea refractory to CPAP
- Recurrent aspiration with failed conservative management
Recognising the Need — Signs of Airway Obstruction
| Stage | Signs |
|---|---|
| Early | Suprasternal, supraclavicular, intercostal retractions; inspiratory stridor |
| Late | Agitation, altered consciousness, rising pulse and RR, paradoxical pulse |
| Danger | Pallor or cyanosis, fatigue and exhaustion — intervene before these appear |
Intervene early rather than wait for late or danger signs.
Surgical Technique — Open Tracheotomy
Position: Supine, neck extended (shoulder roll under shoulders)
Steps:
- Skin incision — Horizontal or vertical midline incision, 2 cm below the cricoid cartilage
- Subcutaneous dissection — Divide subcutaneous tissue and superficial cervical fascia
- Strap muscle separation — Retract sternohyoid and sternothyroid muscles laterally at the midline (do not cut)
- Thyroid isthmus — Retract superiorly or divide between clamps and ligate if it overlies the trachea
- Pretracheal fascia — Dissect and expose anterior tracheal wall
- Tracheal incision — Between the 2nd and 3rd tracheal rings (never the 1st ring — risks subglottic stenosis)
- Options: vertical incision, horizontal incision, window/Bjork flap
- Stay sutures — Placed through tracheal rings on each side; labeled LEFT/RIGHT and taped to chest for emergency re-access
- Partial withdrawal of ETT — Pull ET tube tip just superior to the tracheotomy site before inserting trach tube
- Tracheotomy tube insertion — Insert with obturator, inflate cuff, confirm with capnography and bilateral auscultation
- Secure tube — Suture flange to skin + trach ties (one–two fingers should fit under ties)
Operative Image
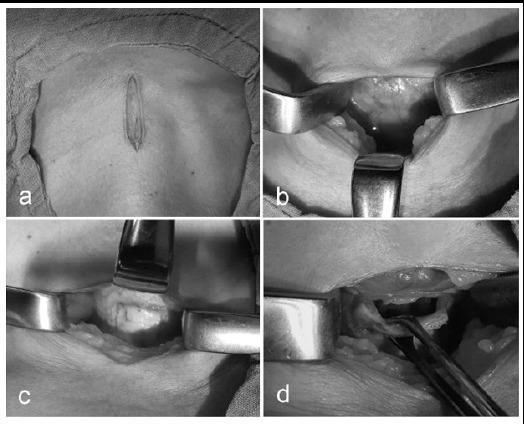
Intraoperative steps: (a) vertical midline incision, (b) retraction exposing thyroid isthmus, (c) inferiorly-based tracheal flap creation between 2nd–3rd rings, (d) elevation of flap exposing tracheal lumen
Bjork Flap Technique
Inverted-U tracheal flap sutured down to skin — facilitates easier tube changes and reduces risk of false passage on reinsertion
Postoperative Care
- Chest X-ray (AP + lateral) to confirm tube position, exclude pneumothorax and pneumomediastinum
- Do not change outer tube for 3–4 days (tract not yet formed — risk of false passage)
- Frequent inner cannula cleaning and suctioning
- Stay sutures remain accessible for at least 7 days in case of accidental decannulation
- Humidified oxygen/air to prevent crusting of secretions
Complications
| Timing | Complications |
|---|---|
| Immediate | Bleeding, pneumothorax, pneumomediastinum, subcutaneous emphysema, false passage, tube displacement, post-obstructive pulmonary oedema, apnoea (loss of hypoxic drive) |
| Delayed | Granulation tissue, stomal infection, subglottic/tracheal stenosis, tracheomalacia, tracheo-oesophageal fistula, tracheo-innominate fistula (life-threatening — tube too low), persistent tracheocutaneous fistula after decannulation |
Types of Tracheotomy Tubes
| Type | Use |
|---|---|
| Cuffed | Mechanical ventilation, aspiration risk |
| Uncuffed | Speaking, decannulation weaning |
| Fenestrated | Allows phonation through upper airway |
| Metal (Jackson) | Long-term use, easy to clean |
| PVC (Shiley) | Standard ICU use |
— Cummings Otolaryngology 7e; K.J. Lee's Essential Otolaryngology
Acute epiglottitis
Asking for Preferences
Finding Sources
Searching the Web
acute epiglottitis full overview etiology pathophysiology clinical features management 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Acute Epiglottitis — Full Overview
Definition
Acute epiglottitis (supraglottitis) is an acute, rapidly progressive bacterial cellulitis causing inflammation and oedema of the epiglottis, aryepiglottic folds, arytenoids, and surrounding supraglottic structures — resulting in potentially fatal upper airway obstruction.
Epidemiology
- Pre-vaccine era: primarily affected children aged 2–7 years
- Post-Hib vaccine era (post-1985): incidence in children has fallen dramatically; disease now relatively more common in older children and adults (adults peak at 20–40 years)
- Incidence: ~10–40 cases per million in the USA
Etiology
| Type | Causative Agents |
|---|---|
| Infectious (most common) | H. influenzae type B (Hib) — still most common in children; Streptococci (Gp A, S. pneumoniae), S. aureus (including MRSA), Neisseria meningitidis |
| Post-vaccine era | Streptococcal & staphylococcal species now predominate |
| Immunocompromised | Pseudomonas aeruginosa, Candida spp. |
| Non-infectious (rare) | Thermal injury (hot liquids/steam), caustic ingestion, allergic reaction, foreign body, lymphoproliferative disorders |
Pathophysiology
Bacterial invasion of supraglottic mucosa
↓
Cellulitis → Inflammation & oedema of epiglottis +
aryepiglottic folds + arytenoids
↓
Structures protrude DOWNWARD over the glottic opening
↓
Reduced upper airway calibre → turbulent inspiratory airflow (STRIDOR)
↓
Epiglottis acts as a BALL VALVE:
- Obstructs airflow during INSPIRATION
- Permits exhalation
↓
Worsening hypoxia → respiratory failure → DEATH
The danger is the speed — a child can progress from mild sore throat to complete airway obstruction within hours.
Clinical Features — The 4 D's
| D | Feature |
|---|---|
| Drooling | Cannot swallow — secretions pool |
| Dysphagia | Intense, painful swallowing |
| Dysphonia | Muffled "hot potato" voice (not hoarse) |
| Dyspnoea | Respiratory distress, inspiratory stridor |
Additional features:
- Abrupt onset of high fever (>39°C)
- Severe sore throat out of proportion to physical findings
- Toxic, anxious appearance
- Tripod/sniffing position — sitting upright, leaning forward, jaw jutted, neck extended ← near-pathognomonic
- No cough (key differentiator from croup)
- Anterior neck tenderness on palpation
- Cyanosis — late, pre-terminal sign
Investigations
| Investigation | Finding |
|---|---|
| Lateral soft tissue X-ray neck | "Thumbprint sign" — swollen epiglottis ± thickened aryepiglottic folds; absent vallecula air sign. Up to 70% may be normal |
| FBC | Leukocytosis (WBC elevated) |
| Blood culture | Bacteraemia in ~25% of cases |
| Direct laryngoscopy | Cherry-red, swollen epiglottis — only in controlled OR/ICU setting |
| CT neck | Used in stable adults if diagnosis uncertain |
⚠️ Never perform direct throat examination in the ED in an unsecured patient — may trigger total laryngospasm.
Management
Step 1 — Immediate Priorities (ABC)
- Do NOT lay patient flat — maintain sitting/tripod position
- Minimise disturbance — no IV lines, blood draws, or throat exam until airway is secured
- Administer humidified oxygen by mask if tolerated (do not force)
- Call anaesthesiology + ENT + ICU simultaneously
- Transport to operating theatre for controlled airway management
Step 2 — Airway Management
| Situation | Action |
|---|---|
| Child with airway compromise | Immediate transfer to OR → inhalation induction → oral/nasotracheal intubation under GA |
| Stable older child / adult | Fiberoptic nasotracheal intubation under conscious sedation |
| Intubation fails | Emergency cricothyroidotomy (adults) or needle cricothyroidotomy (children) |
| Skilled personnel unavailable | Emergency tracheostomy |
- Remain intubated for 3–5 days while antibiotics reduce oedema
- Extubate when an air leak develops around the tube (indicates reduced swelling)
Step 3 — Medical Management
| Drug | Dose/Detail |
|---|---|
| IV antibiotics | 2nd/3rd-generation cephalosporin (ceftriaxone) + vancomycin if MRSA suspected — for 7–10 days |
| Nebulised L-epinephrine | Decreases mucosal oedema temporarily |
| Corticosteroids | Often used (dexamethasone) to reduce supraglottic oedema |
| IV fluids | Maintain hydration |
Step 4 — Admission
- All patients → ICU or HDU regardless of initial severity
Epiglottitis vs Croup — Key Differences
| Feature | Epiglottitis | Croup |
|---|---|---|
| Age | 2–7 yrs (pre-vaccine); adults | 6 months – 3 years |
| Onset | Hours | Days |
| Cough | Absent | Barky/seal-like |
| Drooling | Prominent | Absent |
| Position | Tripod/sniffing | No preference |
| Voice | Muffled | Hoarse |
| Fever | High (>39°C) | Low-grade |
| X-ray | Thumbprint sign | Steeple sign |
| Cause | Bacterial | Viral (parainfluenza) |
Complications
- Total airway obstruction → respiratory arrest → death
- Bacteraemia / septicaemia
- Epiglottic abscess (especially adolescents)
- Necrotising epiglottitis (immunocompromised)
- Pulmonary oedema post-obstruction
- Subglottic stenosis (after prolonged intubation)
— Rosen's Emergency Medicine 10e; Tintinalli's Emergency Medicine 9e; Barash Clinical Anesthesia 9e
Surgical management
Reading File
Finding Sources
Searching the Web
acute epiglottitis surgical airway management intubation tracheostomy cricothyrotomy steps
Reading File
Searching Images
epiglottitis airway management algorithm intubation tracheostomy
Surgical Management of Acute Epiglottitis
Guiding Principle
Airway first — everything else second. The goal of surgical management is to establish and maintain a patent, secure airway before respiratory failure occurs. The approach differs based on age and severity.
Decision Algorithm
SUSPECTED ACUTE EPIGLOTTITIS
↓
Keep patient calm, upright (tripod)
Humidified O₂ by mask if tolerated
Call: Anaesthesiology + ENT + ICU
↓
┌─────────────────────────────────┐
│ ASSESS SEVERITY │
└─────────────────────────────────┘
↓ ↓
CHILD / Severe ADULT / Stable
airway compromise mild-moderate
↓ ↓
Transfer directly ICU admission
to OPERATING IV antibiotics
THEATRE IV steroids
↓ Monitor closely
Inhalation induction ↓
(sevoflurane, O₂) Worsening? → OR
↓
Oral intubation
(tube 0.5mm smaller)
↓
FAILS → Rigid bronchoscopy
↓
FAILS → Surgical airway
Step-by-Step Surgical Airway Management
1. Pre-operative Preparation (in OR)
- Patient kept sitting upright in the OR while monitoring is placed
- Pulse oximetry + capnography + precordial stethoscope
- OR prepared with: laryngoscope, video laryngoscope, rigid bronchoscope, surgical tracheostomy set — all immediately available
- One parent may remain in the OR to keep child calm
- Do NOT give IV access or perform venepuncture before induction — crying worsens stridor and can trigger total obstruction
2. Anaesthetic Induction
- Inhalation induction with sevoflurane + oxygen (increasing concentrations slowly)
- Child may sit in anaesthesiologist's lap during induction
- Spontaneous breathing maintained throughout — muscle relaxants avoided until airway is secured
- Once consciousness is lost: IV access obtained, patient lowered supine
3. Laryngoscopy and Intubation
- Video laryngoscopy preferred — allows shared view of distorted anatomy among the whole team
- Oral endotracheal intubation performed without muscle relaxants
- ETT 0.5 mm smaller than usual (to accommodate swollen supraglottic structures)
- Stylet often needed
- If glottis cannot be visualised: ask assistant to compress the chest → air bubble rises from glottis → aim for it
4. Failed Intubation Protocol
| Step | Action |
|---|---|
| 1st attempt fails | Reposition, use video laryngoscope |
| Video laryngoscopy fails | Rigid bronchoscopy — can be passed through swollen supraglottis |
| Rigid bronchoscopy fails | Surgical airway |
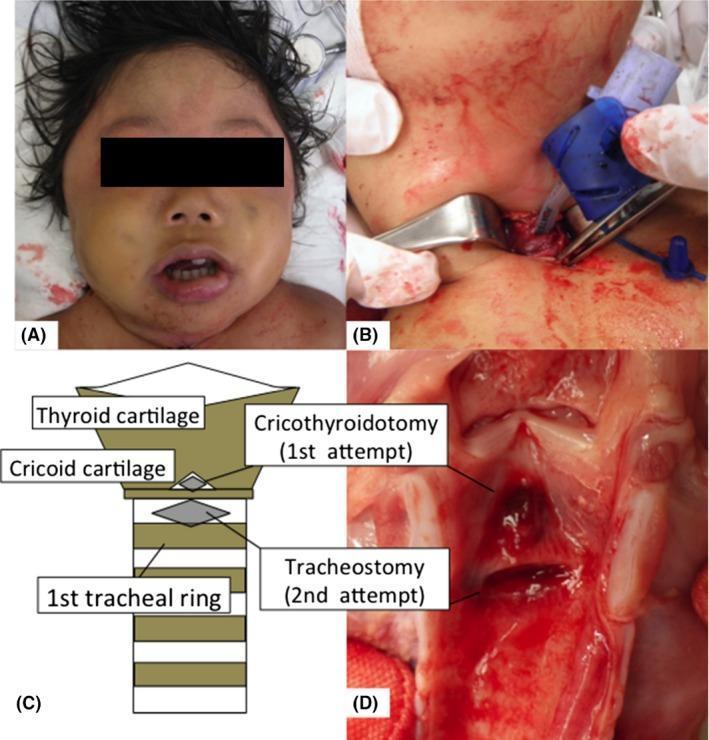
5. Surgical Airway Options
A. Cricothyroidotomy (adults & older children ≥12 yrs)
- Landmark: cricothyroid membrane (between thyroid & cricoid cartilage)
- Vertical skin incision → horizontal stab through membrane → insert cuffed tube/airway catheter
- Fastest emergency surgical airway
- Must be converted to tracheostomy within 24–72 hrs (risk of subglottic stenosis)
B. Needle Cricothyroidotomy (children <12 yrs)
- 14G angiocatheter through cricothyroid membrane
- Attach to jet ventilator or 3mL syringe barrel + bag-valve-mask
- Temporising only — buys 30–45 minutes of oxygenation
C. Emergency Tracheostomy
- Preferred when personnel skilled in difficult airways are not available
- Creates airway below the obstruction — most definitive
- Between 2nd–3rd tracheal rings
- Larger, more stable airway; better for prolonged ventilation
Post-Intubation Management
| Action | Detail |
|---|---|
| Transfer to ICU | Immediate after airway secured |
| Throat + blood cultures | Taken intraoperatively once intubated |
| IV antibiotics started | Ceftriaxone ± vancomycin (MRSA cover) |
| Conversion to nasotracheal tube | More comfortable for patient; easier to secure |
| Sedation | To prevent accidental self-extubation |
| Duration of intubation | 48–72 hours (Barash); up to 3–5 days (Rosen's) |
| Extubation criteria | Air leak around tube + fiberoptic bronchoscopy confirms epiglottic swelling reduced |
| Extubation location | Back in OR, not at bedside — with surgeon and equipment on standby |
Adult vs Child — Key Difference
| Child | Adult | |
|---|---|---|
| Urgency | Immediate OR — no delay | Many can be managed in ICU with conservative Rx first |
| Induction | Inhalation (sevoflurane) | Awake fiberoptic nasotracheal intubation preferred |
| Muscle relaxants | Avoided until airway secured | Avoided until airway secured |
| Tracheostomy | Fallback if intubation fails | Fallback if intubation fails |

— Barash Clinical Anesthesia 9e; Miller's Anesthesia 10e; Rosen's Emergency Medicine 10e; Tintinalli's Emergency Medicine 9e
Medical tracheotomy
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.