Lipoma gross and microscopy size measuring 4.1x3.2x1.8 cms
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I have rich content and clear images. Here is a complete pathology report-style description for this lipoma:
Lipoma - Gross and Microscopic Pathology
Specimen size: 4.1 x 3.2 x 1.8 cm
GROSS EXAMINATION
Size: 4.1 x 3.2 x 1.8 cm (within the typical range for conventional subcutaneous lipoma; most present as small, solitary masses, though they can reach several centimeters)
Shape: Well-defined, ovoid to lobulated mass
Surface / Capsule: Surrounded by a thin, glistening fibrous capsule - the tumor is well-encapsulated, clearly demarcated from surrounding tissues
Cut section:
- Uniform yellow, greasy, glistening surface - identical in appearance to normal subcutaneous fat
- Soft, compressible consistency
- Lobulated architecture separated by thin whitish fibrous septa
- No areas of necrosis, hemorrhage, or cystic change (in uncomplicated cases)
Margins: Pushing, well-circumscribed borders; slips cleanly out of the surrounding tissue at surgery ("enucleation" plane is easily established)
MICROSCOPIC EXAMINATION (H&E)
Low power (scanning):
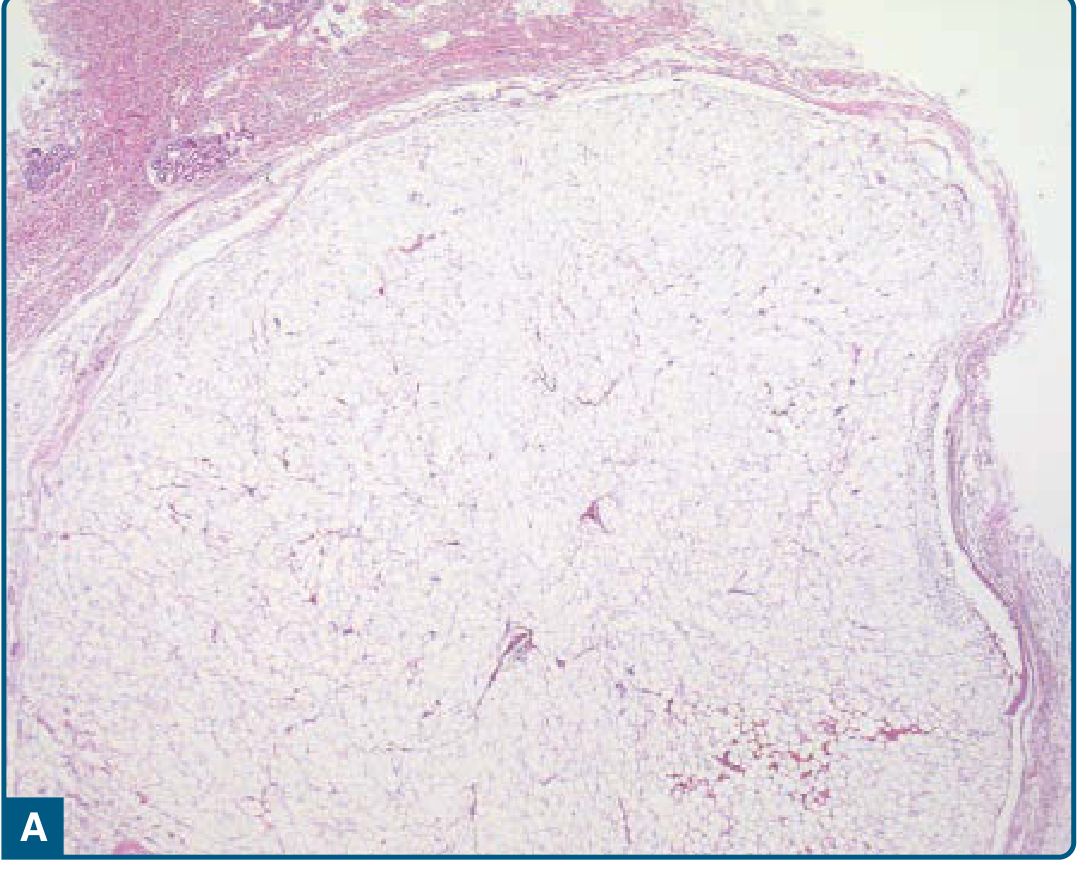
Figure 122-1A (Fitzpatrick's Dermatology): Well-circumscribed, encapsulated lipogenic lesion in the subcutis with a thin fibrous capsule
- Well-circumscribed, encapsulated, lobulated lesion
- Lobules of mature adipose tissue separated by thin, hypocellular fibrous septa
- Septa contain thin-walled capillaries
- Tumor is clearly demarcated from the surrounding dermis/subcutis
High power:
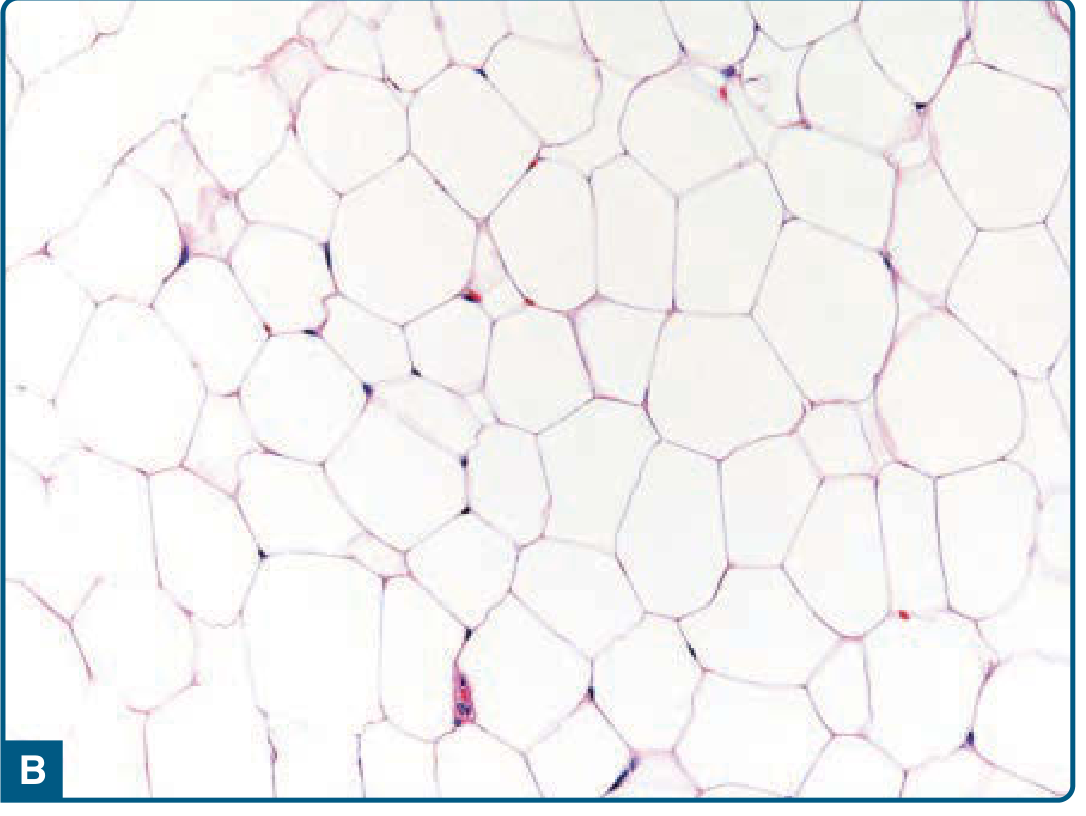
Figure 122-1B (Fitzpatrick's Dermatology): Mature, univacuolated adipocytes showing only mild variation in size and shape
- Adipocytes: Large, mature, univacuolated cells - each cell contains a single large lipid vacuole that displaces the nucleus peripherally ("signet ring" appearance is the mature adipocyte form)
- Nuclei: Small, compressed, peripherally placed, without atypia or hyperchromasia
- Size/shape variation: Only slight variation in adipocyte size and shape - no significant pleomorphism
- Nuclear atypia: Absent
- Mitoses: Absent (or extremely rare)
- Fibrous septa: Thin, hypocellular with thin-walled capillaries
- Necrosis: Absent in uncomplicated cases (post-traumatic cases may show fat necrosis, lipid-laden histiocytes, and chronic inflammation)
IMMUNOHISTOCHEMISTRY (if performed)
| Marker | Result |
|---|---|
| S-100 | Positive (adipocytes) |
| p16 | Negative |
| MDM2 | Negative |
| CDK4 | Negative |
The negativity for p16, MDM2, and CDK4 is important to distinguish lipoma from atypical lipomatous tumor (ALT)/well-differentiated liposarcoma, which shows focal positivity for these markers.
DIAGNOSIS
Benign lipoma, conventional type
KEY DISTINGUISHING FEATURES FROM MALIGNANCY
| Feature | Lipoma | Atypical Lipomatous Tumor / WD Liposarcoma |
|---|---|---|
| Encapsulation | Well-encapsulated | May be poorly marginated (especially retroperitoneal) |
| Adipocyte atypia | None | Striking variation in size; hyperchromatic nuclei |
| Fibrous septa | Thin, hypocellular | Often contain atypical/enlarged stromal cells |
| Lipoblasts | Absent | May be present |
| MDM2/CDK4 IHC | Negative | Focally positive (nuclear) |
| MDM2 FISH | No amplification | 12q13-q15 amplification |
NOTES FOR THIS SPECIMEN
- At 4.1 cm, this lipoma is moderately sized. Most conventional lipomas are < 5 cm. Lipomas > 5-10 cm or those in deep locations (intramuscular, retroperitoneal) warrant extra scrutiny to exclude ALT/WD liposarcoma.
- Intramuscular lipomas can be poorly circumscribed with infiltration of skeletal muscle fibers (which show secondary atrophy).
- If any worrisome histologic features are present (atypia, lipoblasts, thick septa with atypical cells), MDM2 FISH should be performed.
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 1117
- Robbins & Kumar Basic Pathology (Robbins Pathology), block 8
- Fitzpatrick's Dermatology, Vol. 1-2, pp. 2202-2203 (Fig. 122-1)
This is a shared conversation. Sign in to Orris to start your own chat.