Indications for Transfusion i. Anemia, thrombocytopenia, coagulopathy ii. Massive transfusion protocol in medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have all the information needed for a thorough, well-sourced answer. Here it is:
Indications for Transfusion
I. Anemia - Red Blood Cell (RBC) Transfusion
Rationale
RBC transfusions are used to treat anemia when a patient requires increased oxygen-carrying capacity. In an average adult, one unit of packed RBCs (pRBCs) raises hemoglobin (Hb) by ~1 g/dL and hematocrit (Hct) by ~3%.
Transfusion Thresholds (Triggers)
| Clinical Setting | Hb Threshold |
|---|---|
| General hospitalized / critically ill (stable) | < 7.0 g/dL (restrictive strategy) |
| Acute coronary syndrome / acute MI | < 8.0 g/dL |
| Symptomatic anemia (dyspnea, angina, tachycardia) | Regardless of Hb level |
| Active hemorrhagic shock | Immediate regardless of Hb |
| Chronic transfusion-dependent anemia | Higher threshold may apply |
The restrictive strategy (transfuse at Hb < 7 g/dL) has been validated in nearly 50 RCTs and is as effective as the liberal strategy (Hb < 10 g/dL) for most patients, with equivalent rates of mortality, MI, stroke, and infection. A large RELIEVE trial of ventilated ICU patients over age 55 showed the restrictive group had >30% lower mortality.
Critical principle: Hb level alone should NOT be the sole transfusion trigger - the patient's overall clinical status (symptoms, hemodynamics, comorbidities, trajectory of blood loss) must guide the decision.
- Goldman-Cecil Medicine, p. 2990-2992
- Mulholland & Greenfield's Surgery, p. 619
Practical Notes
- Give as single units in stable, non-hemorrhaging patients, then reassess
- Do NOT use lactated Ringer's as a diluent (contains Ca²+, may cause clotting via citrate reversal)
- Compatible diluents: 0.9% saline, 5% dextrose in 0.9% saline, Normosol-R
II. Thrombocytopenia - Platelet Transfusion
Indications fall into two categories: prophylactic (prevention of hemorrhage) and therapeutic (treatment of active bleeding).
Prophylactic Platelet Thresholds
| Platelet Count | Indication |
|---|---|
| < 10,000/μL | Hospitalized patients with therapy-induced hypoproliferative thrombocytopenia (chemotherapy, stem cell transplant) - high risk of spontaneous hemorrhage |
| < 20,000/μL | Febrile/septic patients; central venous catheter placement; bronchoscopy; minor procedures |
| < 50,000/μL | Major non-neuraxial surgery; elective diagnostic lumbar puncture; invasive procedures; active bleeding |
| < 100,000/μL | Neurosurgery; ocular procedures; CNS/retinal bleeding |
Therapeutic Platelet Transfusion (Active Bleeding)
- Maintain platelet count > 50,000/μL in bleeding patients (most sites)
- Maintain > 100,000/μL for neurologic hemorrhage or CNS bleeding
- Platelet transfusion is not recommended for intracranial hemorrhage while receiving antiplatelet therapy (PATCH trial showed no benefit and greater morbidity)
- Not routinely indicated as prophylaxis for CABG (AABB guideline)
Response Assessment
-
One platelet dose (single apheresis unit or 4-6 pooled whole-blood-derived units) should raise count by 30,000-60,000/μL
-
Corrected Count Increment (CCI) > 7.5 at 1 hour = acceptable response
-
CCI < 7.5 at 1 hour = platelet refractoriness (consider HLA-matched platelets)
-
Goldman-Cecil Medicine (Table 162-4), p. 2997-3000
-
Fischer's Mastery of Surgery, p. 395
-
Henry's Clinical Diagnosis & Management, p. 980-983
III. Coagulopathy - Plasma, Cryoprecipitate, and Factor Replacement
Fresh Frozen Plasma (FFP)
FFP contains all coagulation factors. Dose of 10-15 mL/kg increases factor levels by approximately 20%.
Indications:
- Massive transfusion (plasma : RBC ratio of at least 1:2, ideally 1:1)
- INR > 2.0 prior to invasive procedure or surgery with active bleeding
- Replacement fluid for plasma exchange in thrombotic thrombocytopenic purpura (TTP)
- Reversal of warfarin when vitamin K and prothrombin complex concentrate (PCC) are unavailable or insufficient
- Dilutional coagulopathy after massive PRBC transfusion
FFP is not recommended in the absence of bleeding (e.g., no role in sepsis prophylaxis, no evidence from RCTs in that context).
Cryoprecipitate
Rich in fibrinogen, Factor VIII, Factor XIII, and von Willebrand factor (vWF). Units are typically pooled (multiple donors) for large-dose delivery.
Indications:
- Fibrinogen < 150 mg/dL with active bleeding (each unit raises fibrinogen by ~7 mg/dL)
- Hypofibrinogenemia in DIC, massive hemorrhage, obstetric hemorrhage
- Hemophilia A (Factor VIII deficiency) when specific concentrates unavailable
- von Willebrand disease (when vWF concentrate unavailable)
- Factor XIII deficiency
Prothrombin Complex Concentrate (PCC)
-
Preferred over FFP for urgent warfarin reversal (faster, smaller volume, no thawing required)
-
Goldman-Cecil Medicine (Table 162-4), p. 3008
-
Fischer's Mastery of Surgery, p. 395-396
IV. Massive Transfusion Protocol (MTP)
Definition
Massive transfusion is classically defined as transfusion of ≥ 10 units of pRBCs within 24 hours, though many centers now use ≥ 6 units in 6 hours or projected ongoing hemorrhage as activation criteria.
When to Activate MTP
The MTP is activated based on hemodynamic and injury criteria. The Denver Health / Schwartz's Principles protocol uses:
| Trigger | Criteria |
|---|---|
| SBP ≤ 70 mmHg alone in field or ED | + penetrating torso injury, major pelvic fracture, or FAST positive in >1 body region |
| SBP 71-90 mmHg AND HR ≥ 108 | Same injury criteria as above |
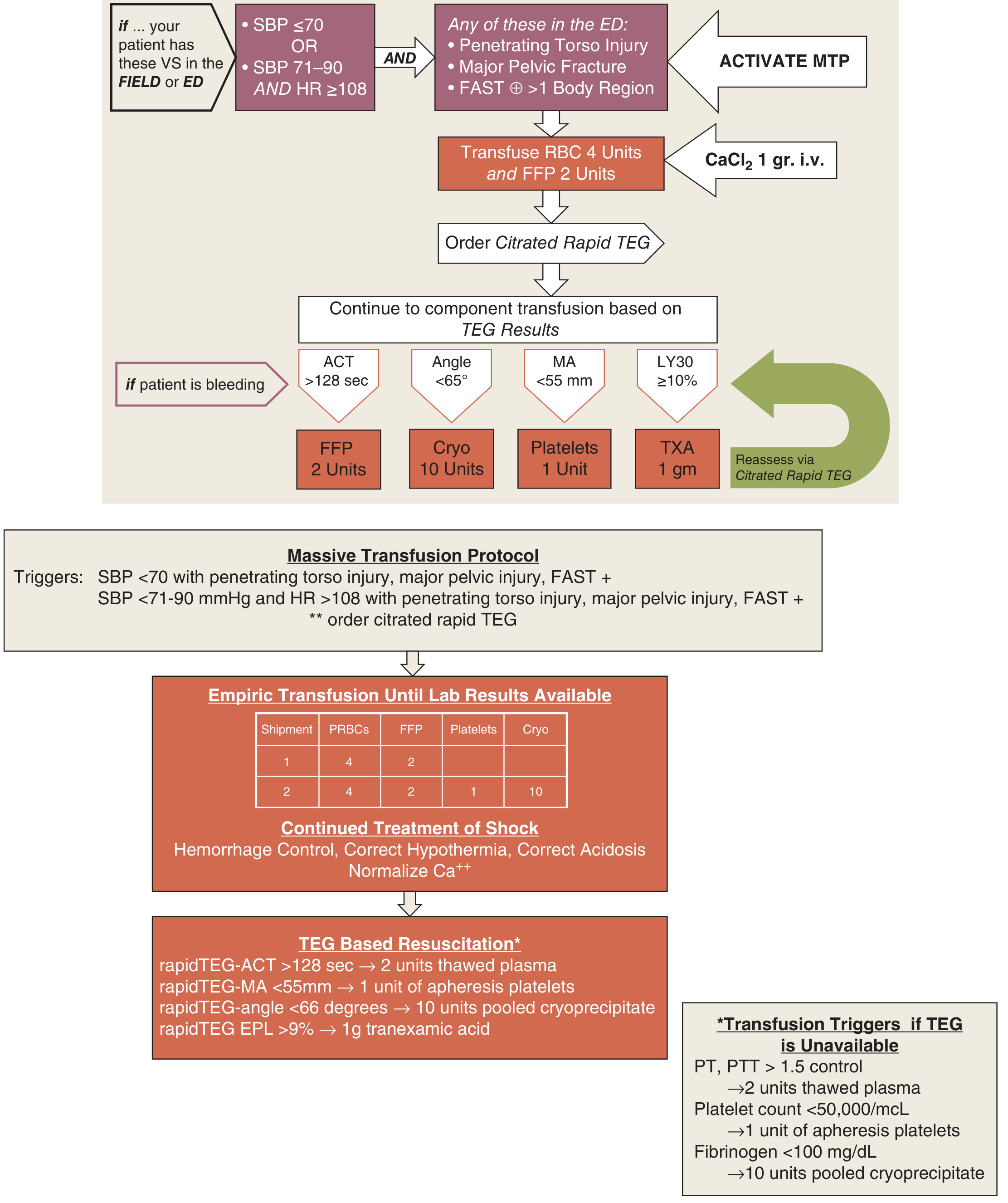
MTP Steps
Step 1 - Activation & Initial Empiric Transfusion:
- Give CaCl₂ 1 g IV (to counteract citrate-induced hypocalcemia)
- Transfuse 4 units pRBCs + 2 units FFP immediately (first cooler)
- Order citrated rapid TEG (thromboelastography)
Step 2 - Continued Empiric Component Therapy:
Subsequent coolers provide blood products in a 1:1:1 ratio (pRBC : FFP : platelets):
| Shipment | pRBCs | FFP | Platelets | Cryoprecipitate |
|---|---|---|---|---|
| 1st | 4 units | 2 units | - | - |
| 2nd | 4 units | 2 units | 1 unit | 10 units |
Step 3 - TEG-Guided (Goal-Directed) Resuscitation:
| TEG Finding | Component |
|---|---|
| ACT > 128 sec (factor deficiency) | FFP 2 units |
| Angle < 65° (hypofibrinogenemia) | Cryoprecipitate 10 units |
| MA < 55 mm (thrombocytopenia/dysfunction) | Platelets 1 unit |
| LY30 ≥ 10% (hyperfibrinolysis) | Tranexamic acid (TXA) 1 g |
If TEG is unavailable, use conventional lab triggers:
- PT/PTT > 1.5× control → 2 units thawed plasma
- Platelet count < 50,000/μL → 1 unit apheresis platelets
- Fibrinogen < 100 mg/dL → 10 units pooled cryoprecipitate
The "Lethal Triad" - What MTP is Designed to Prevent
MTP addresses the three self-reinforcing causes of death in massive hemorrhage:
- Hypothermia (<34°C): impairs coagulation enzyme activity, causes myocardial irritability. Prevented with warm IV fluids, Bair Hugger warmers, warmed ventilatory gases.
- Acidosis: impairs coagulation cascade, cardiac performance, enzyme activity.
- Coagulopathy: dilutional (from crystalloid resuscitation) + consumptive (from shock and injury). Prevented by early balanced blood product resuscitation.
Damage Control Resuscitation (DCR) Principle
The modern evidence-based approach uses early high-ratio blood product resuscitation - reconstituting whole blood from components - rather than crystalloid-first resuscitation. Multiple studies have shown that implementing an MTP improves survival in trauma patients. The American College of Surgeons now requires all verified trauma centers to have an MTP in place.
- Schwartz's Principles of Surgery, p. 962-969
- Sabiston Textbook of Surgery, p. 587-588
- Mulholland & Greenfield's Surgery, p. 1593-1600
Summary Table: Evidence-Based Transfusion Triggers
| Component | Threshold / Indication | Expected Response |
|---|---|---|
| pRBCs | Hb < 7 g/dL (stable); Hb < 8 g/dL (ACS/MI) | +1 g/dL Hb; +3% Hct per unit |
| Platelets | <10K (med); <20K (procedure); <50K (surgery/bleeding); <100K (neuro) | +30,000-60,000/μL per dose |
| FFP | INR >2.0 + bleeding; MTP (1:1 with RBC) | +20% factor levels per 10-15 mL/kg |
| Cryoprecipitate | Fibrinogen < 150 mg/dL + bleeding | +7 mg/dL fibrinogen per unit |
| PCC | Urgent warfarin reversal; factor deficiency | Rapid INR correction |
This is a shared conversation. Sign in to Orris to start your own chat.