Flagellates SN 1. LD Bodies [Leishmania donovani] 2. Acute Giardiasis - laboratory diagnosis, findings LAQ 1. Leishmania donovani - life cycle, Kala Azar* (visceral leishmaniasis) - pathogenicity, laboratory diagnosis*; life cycle Sporozoa SN 1. Malaria - laboratory diagnosis 2. Plasmodium falciparum* infections - complications*; laboratory diagnosis LAQ 1. Malignant Tertian Malaria - life cycle of parasite, complications, laboratory diagnosis 2. Plasmodium vivax - morphology, life cycle, laboratory diagnosis microbiology 2 MBBS REFER APURB SHASTRI MUHS EXAM ORITNTED detail answer of questions, colour diagrams as well for exam important points for muhs exam cover all ANSWER
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here is your complete, MUHS exam-oriented answer covering all the flagellate and sporozoa topics. Answers are structured in the Apurb Shastri style - clear headings, exam points highlighted, and diagrams included.
FLAGELLATES
SN 1 - LD Bodies (Leishmania donovani)
Full name: Leishman-Donovan Bodies
What are LD bodies?
LD bodies are the intracellular amastigote forms of Leishmania donovani seen inside macrophages (reticuloendothelial cells) in the human host. They are the diagnostic stage of visceral leishmaniasis.
Morphology of LD Bodies:
| Feature | Detail |
|---|---|
| Shape | Round to oval |
| Size | 1-5 µm |
| Nucleus | Large, round, eccentrically placed - stains red/pink |
| Kinetoplast | Rod-shaped, small, stains dark - located adjacent to nucleus |
| Flagellum | Absent (non-motile in tissue) |
| Location | Inside macrophages (NOT free in blood) |
| Stain | Giemsa stain (best), Leishman stain |
MUHS Exam Tip: LD body = nucleus + rod-shaped kinetoplast inside macrophage. Must differentiate from T. cruzi amastigotes (also inside cells, but form pseudocysts in muscle, not just macrophages).
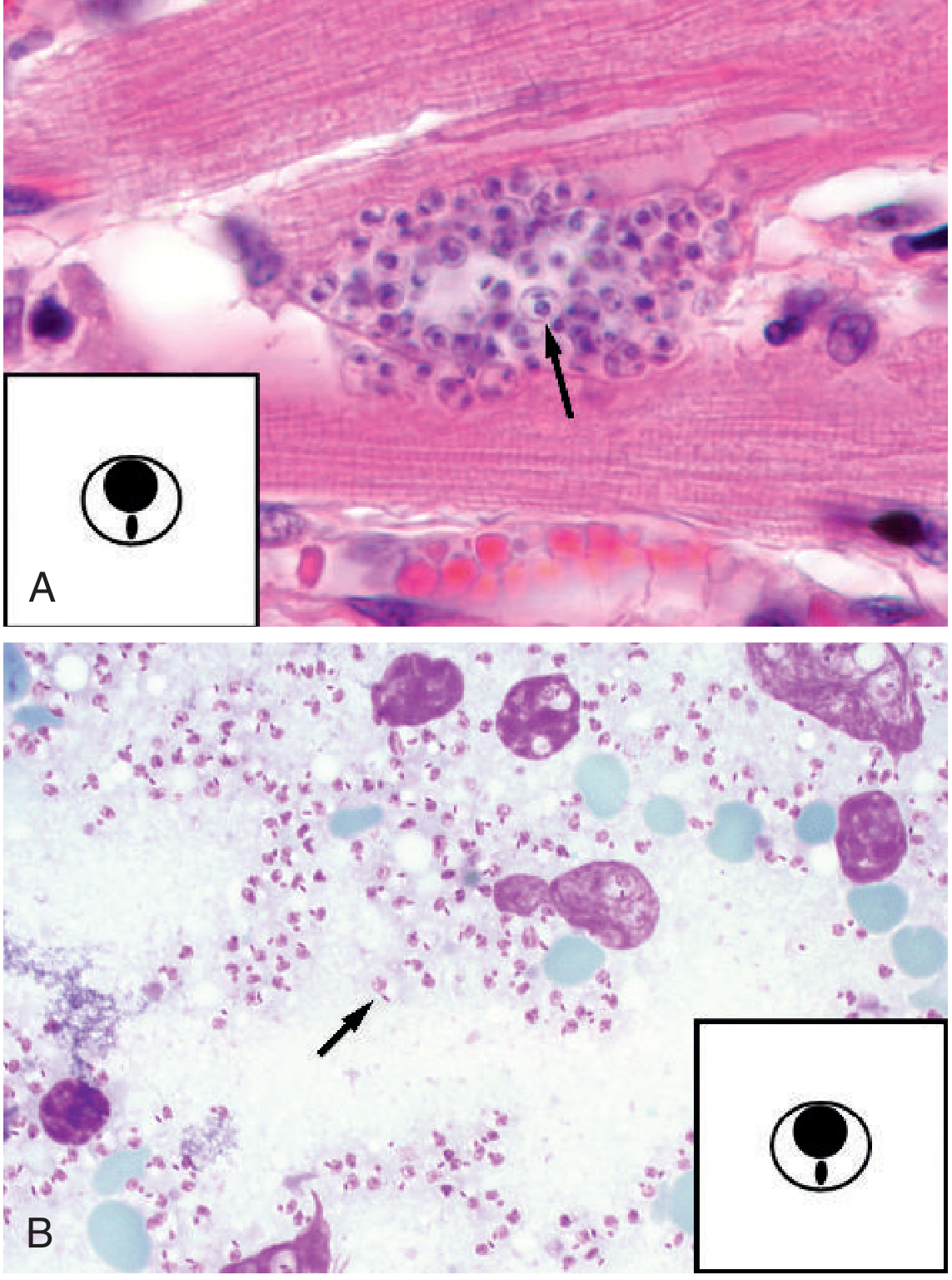
(Fig: Amastigotes of Leishmania spp. [B] inside macrophages on Giemsa stain - each contains nucleus + rod-shaped kinetoplast)
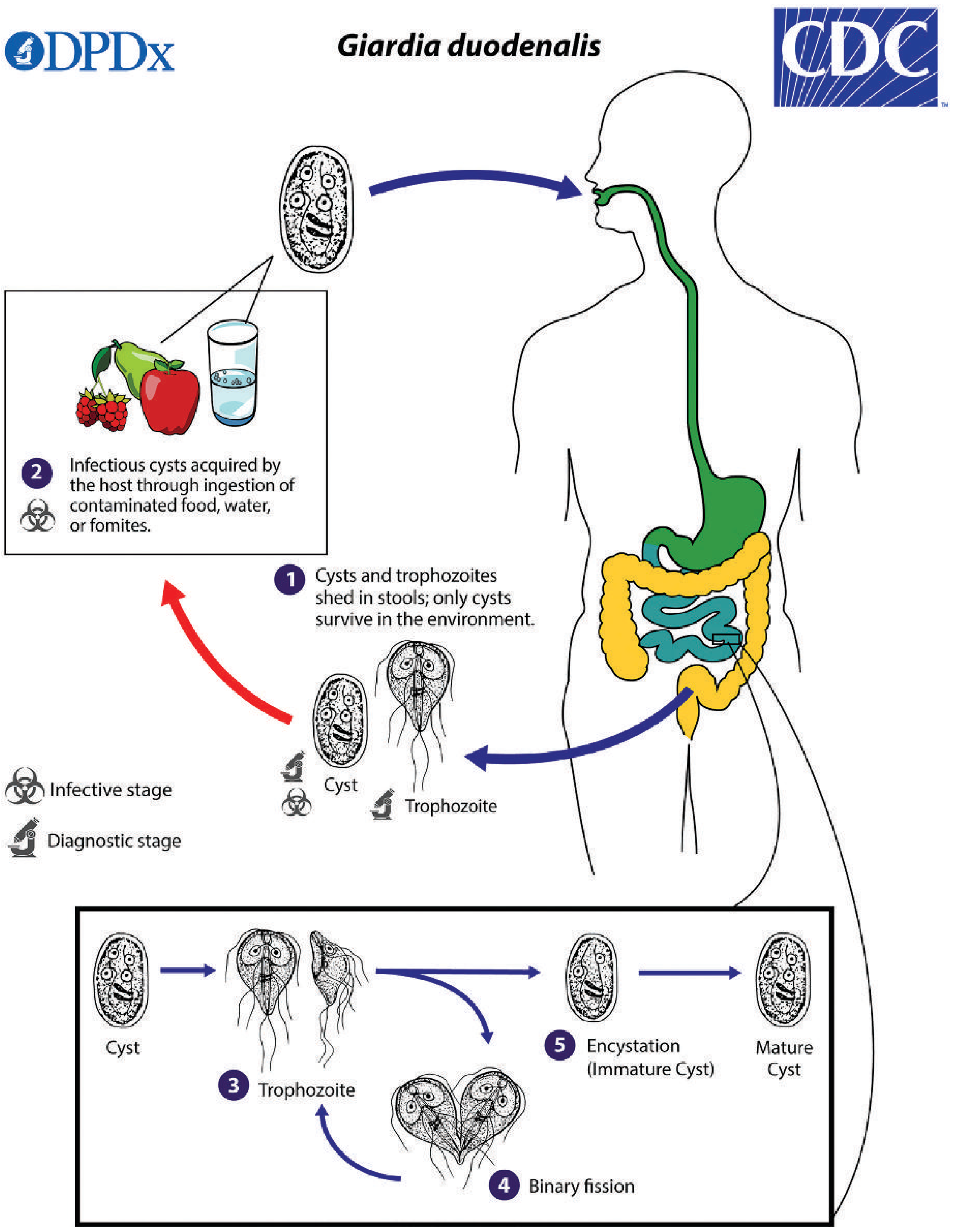
SN 2 - Acute Giardiasis: Laboratory Diagnosis and Findings
Organism: Giardia duodenalis (also called G. lamblia or G. intestinalis)
Clinical Findings in Acute Giardiasis:
- Incubation period: 1-3 weeks
- Acute diarrhea: Watery, foul-smelling, greasy (steatorrhoeic) stools
- Abdominal cramps and bloating
- Flatulence - very characteristic
- Nausea, anorexia
- Self-limited illness lasting 7-10 days
- No blood or mucus in stool (non-invasive parasite)
- Chronic form: malabsorption syndrome (resembling Celiac sprue)
Laboratory Diagnosis:
1. Microscopy (Gold Standard)
- Stool examination (wet mount + permanently stained smear)
- Trophozoite form: Seen in acute/diarrheal stage
- Pear/kite/teardrop shaped
- Size: 10-20 µm
- 2 nuclei anteriorly (giving "owl face" appearance)
- Sucking disc on ventral surface
- 4 pairs of flagella (8 flagella total)
- Characteristic "falling leaf" motility on wet mount
- Cyst form: Seen in chronic/formed stool
- Oval, 8-19 µm
- 2-4 nuclei
- Intracytoplasmic fibrils (axonemes) and curved median bodies
- Cytoplasm retracted from wall
- Concentration methods (formol-ether) increase sensitivity
- Up to 7 stool samples needed for optimal sensitivity (shed sporadically)
2. Duodenal Aspiration / String Test (Enterotest)
- Useful when stool exam is negative
- Trophozoites recovered directly from duodenal fluid
3. Antigen Detection
- EIA (ELISA), DFA (Direct Fluorescent Antibody), LFIC rapid tests
- Sensitivity 90-100%, Specificity ~100%
- Faster than microscopy; preferred in resource-rich settings
- Results in < 30 minutes for rapid tests
4. Molecular Diagnosis
- PCR-based multiplex stool panels - sensitivity ~100%
- Detects G. duodenalis with high accuracy; also used for genotyping
MUHS Exam Tip: "Falling leaf motility" and "owl face trophozoite" are classic exam picks. Stool examination x3 (minimum) to x7 (optimal) needed.
LAQ 1 - Leishmania donovani: Life Cycle, Kala-Azar (Visceral Leishmaniasis) - Pathogenicity and Laboratory Diagnosis
Classification
- Kingdom: Protozoa
- Phylum: Sarcomastigophora
- Order: Kinetoplastida
- Class: Flagellates (Hemoflagellates)
- Species: Leishmania donovani
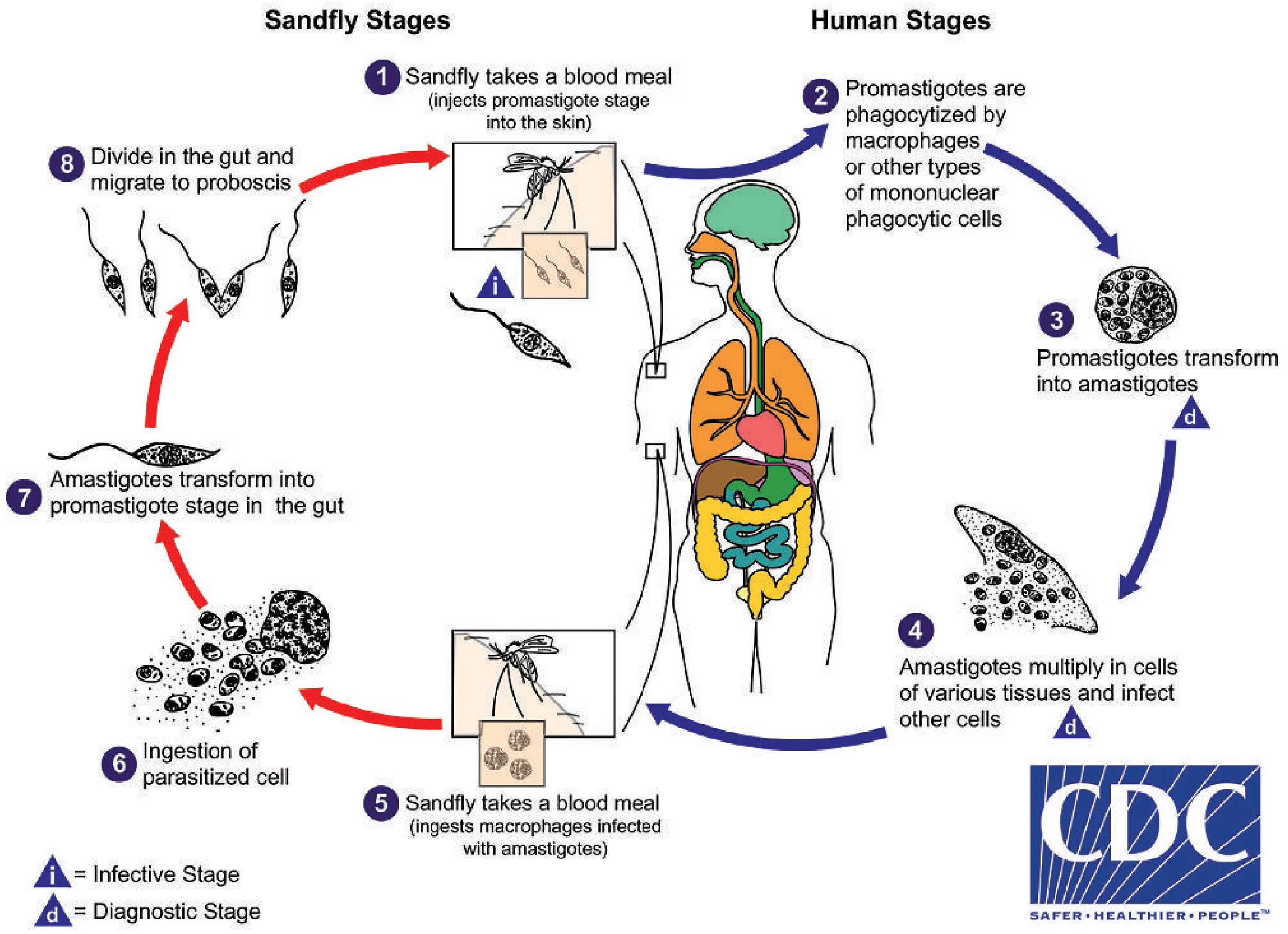
Life Cycle of Leishmania donovani
Two Hosts Required:
- Invertebrate host (vector): Phlebotomus sandfly (Old World) / Lutzomyia (New World)
- Vertebrate host: Humans and dogs
Two Morphological Forms:
| Form | Host | Motility | Description |
|---|---|---|---|
| Promastigote | Sandfly gut | Motile | Elongated, 15-20 µm, flagellum at anterior end, kinetoplast anterior to nucleus |
| Amastigote (LD body) | Human macrophages | Non-motile | Round/oval, 1-5 µm, nucleus + kinetoplast |
Step-by-Step Life Cycle:
In the Sandfly:
- Sandfly takes a blood meal from an infected human - ingests macrophages containing amastigotes
- Amastigotes transform into promastigotes in the midgut of the sandfly
- Promastigotes multiply by binary fission in the gut
- Migrate anteriorly to the proboscis (infective stage ready in ~1 week)
In the Human:
- Infected sandfly bites human - promastigotes inoculated into skin
- Promastigotes immediately phagocytosed by macrophages at the bite site
- Inside the phagolysosome, promastigotes transform into amastigotes (LD bodies)
- Amastigotes multiply by binary fission within macrophages
- Macrophage ruptures → amastigotes infect new macrophages
- Infected macrophages travel via lymphatics/bloodstream to liver, spleen, bone marrow, lymph nodes (reticuloendothelial system)
- Cycle continues → tissue destruction and clinical disease
Kala-Azar (Visceral Leishmaniasis) - Pathogenicity
"Kala-Azar" = Black fever (Hindi) - due to darkening of skin
Organs affected: Liver, spleen, bone marrow, lymph nodes (reticuloendothelial system)
Pathogenesis:
- Massive multiplication of amastigotes in macrophages throughout the RES
- Splenomegaly - due to hyperplasia of macrophages packed with LD bodies; spleen becomes the largest solid organ in the body
- Hepatomegaly - Kupffer cell hyperplasia with amastigotes
- Bone marrow infiltration - replacement of normal marrow leads to:
- Anaemia (normocytic normochromic)
- Leucopenia
- Thrombocytopenia - i.e., Pancytopenia
- Hypergammaglobulinemia - polyclonal B-cell activation (non-specific antibodies - NOT protective)
- Hypoalbuminemia - due to malnutrition and liver involvement → edema
- Aldehyde test (Napier's) becomes positive due to elevated serum globulins
- Skin darkening (hyperpigmentation) - especially on face, hands, feet - due to increased melanin; giving the name "black fever"
- Post-Kala-Azar Dermal Leishmaniasis (PKDL) - hypopigmented or erythematous skin lesions appear months-years after apparently successful treatment
Clinical Features of Kala-Azar:
- Prolonged irregular fever ("double-daily rise" pattern)
- Massive splenomegaly (most important sign) - can reach the pelvis
- Hepatomegaly
- Progressive weight loss and cachexia
- Anaemia - pallor
- Skin darkening
- Lymphadenopathy (in African form)
- Hypergammaglobulinemia
Laboratory Diagnosis of Kala-Azar
A. Parasitological (Definitive):
| Specimen | Method | Sensitivity |
|---|---|---|
| Bone marrow aspirate (sternum/iliac crest) | Giemsa smear, culture | ~70-85% - SAFEST procedure |
| Splenic aspirate | Giemsa smear | >95% sensitivity - HIGHEST but risky (risk of splenic rupture) |
| Lymph node aspirate | Giemsa smear | ~60% |
| Liver biopsy | Giemsa stain | ~70% |
| Buffy coat of peripheral blood | Giemsa smear | Low sensitivity |
- Stain: Giemsa (preferred), Leishman, H&E
- Look for: LD bodies (oval amastigotes with nucleus + kinetoplast) inside macrophages
B. Serological Tests:
| Test | Details |
|---|---|
| rK39 ICT (Rapid Test) | Most widely used; based on recombinant antigen K39; high sensitivity & specificity; India uses this for national program |
| ELISA | High sensitivity for VL |
| IFAT (Indirect Fluorescent Antibody Test) | Serodiagnosis |
| Aldehyde (Napier's Formol-Gel) Test | Tube of serum + 1 drop of formalin - jelly/opaque white clot = positive; indicates hypergammaglobulinemia; non-specific, cheap |
| Chopra's Antimony Test | 4% urea stibamine precipitates in serum - positive in kala-azar |
| DAT (Direct Agglutination Test) | Sensitive for VL |
C. Molecular:
- PCR on peripheral blood, bone marrow, or tissue - highest sensitivity; used in reference labs
D. Leishmanin (Montenegro) Skin Test:
- Negative in active kala-azar (due to depressed CMI)
- Becomes positive only after successful treatment
- NOT useful for diagnosis
MUHS Exam High-Yield Points:
- Splenic aspirate: highest sensitivity (>95%) but risky
- Bone marrow biopsy: safest definitive diagnosis
- rK39 ICT: used in national Kala-Azar elimination program
- Aldehyde test = positive in kala-azar (nonspecific)
- Leishmanin test = NEGATIVE in active disease
- Treatment: Liposomal Amphotericin B (single dose 10 mg/kg IV) - used in India's national program; also Miltefosine (oral)
SPOROZOA
SN 1 - Malaria: Laboratory Diagnosis
Laboratory Diagnosis of Malaria
A. Peripheral Blood Smear (Gold Standard)
Two types of films prepared:
- Thick film - concentration method; detects presence of parasite (screening); better sensitivity at low parasitemia
- Thin film - species identification; morphology better appreciated
Best time to collect: Midway between paroxysms of chills and fever (maximum intracellular organisms present). Repeat every 4-6 hours if initial smear negative.
Stain: Leishman stain or Giemsa stain (preferred)
Species Differentiation on Smear:
| Feature | P. falciparum | P. vivax | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC size | Normal (no enlargement) | Enlarged | Normal | Slightly enlarged, oval |
| Stippling | Maurer dots (clefts) | Schüffner dots (pink) | Ziemann dots | Schüffner dots |
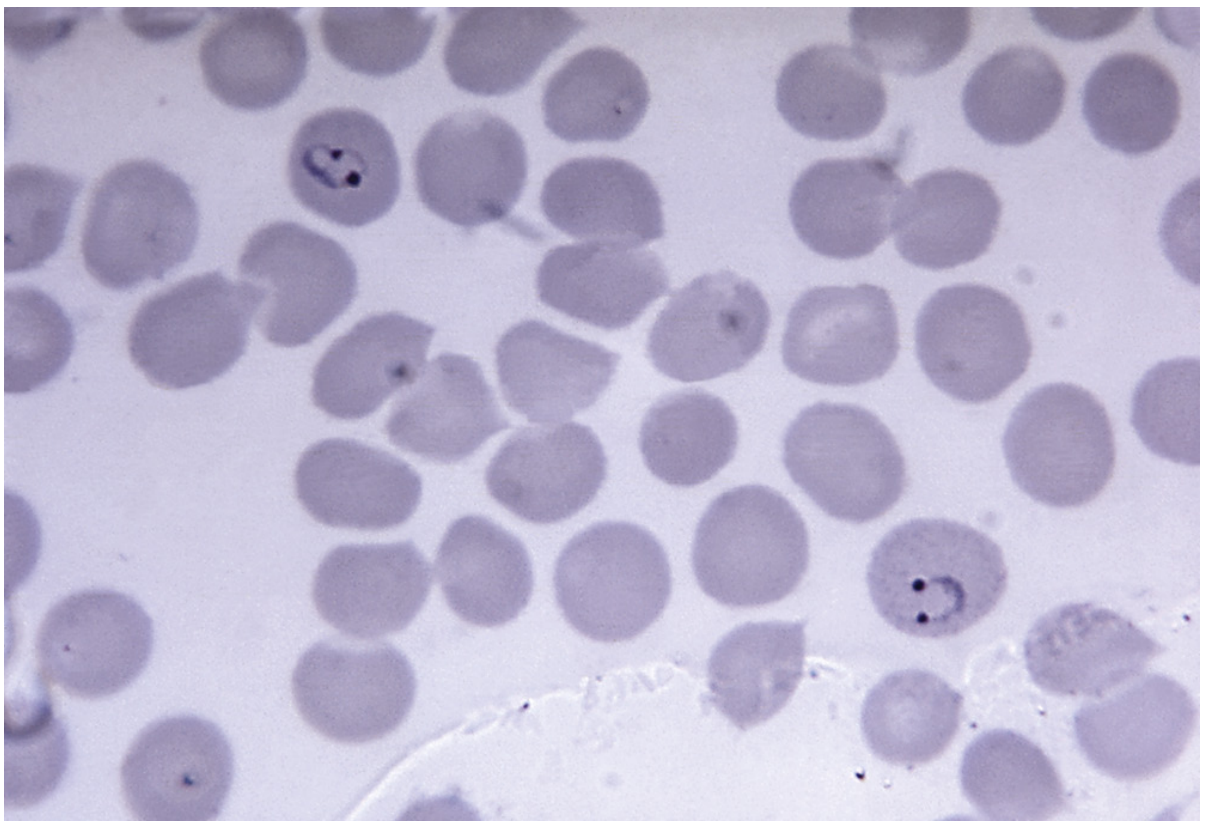
| Ring forms | Multiple rings/cell, accolé (appliqué) position | Single, large rings | Single, compact rings | Single rings |
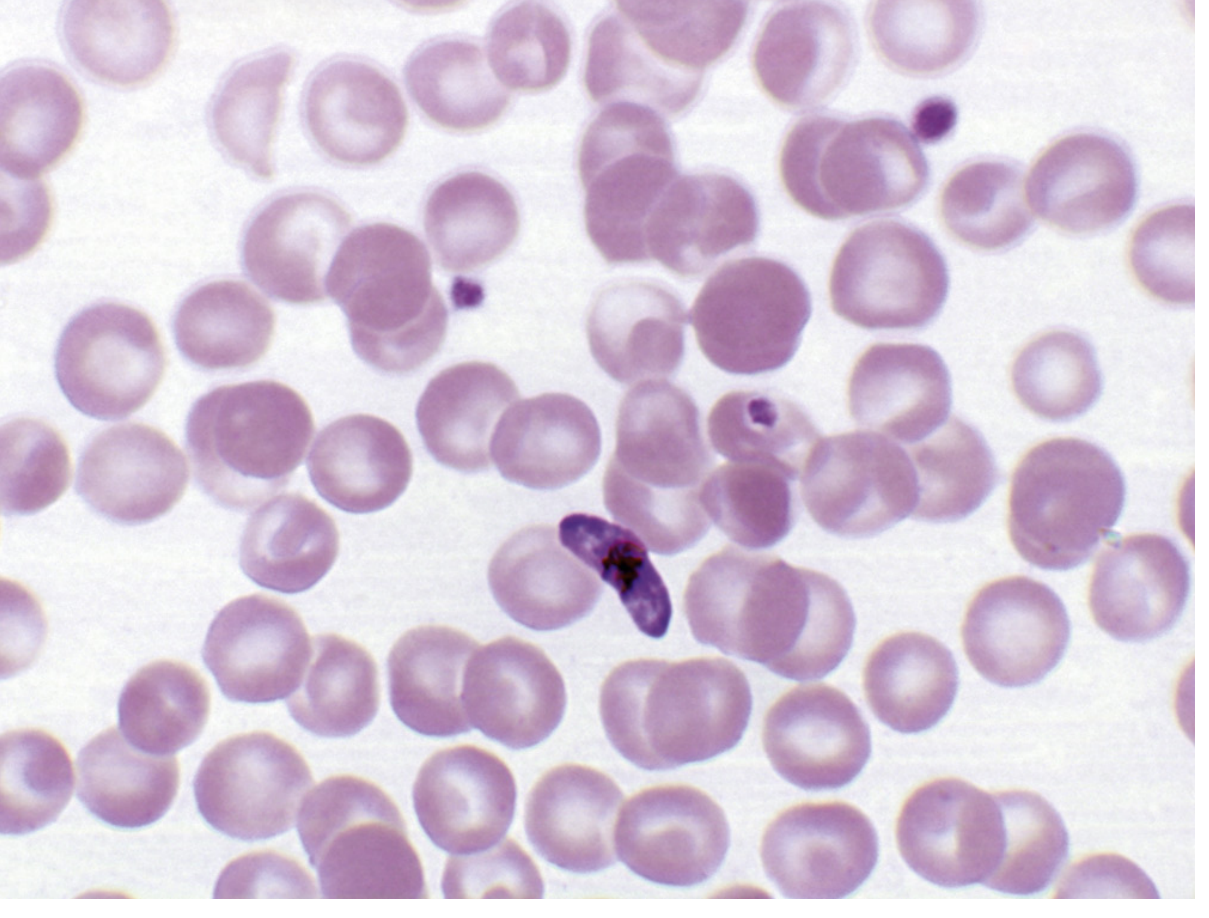
| Gametocyte | Crescent/sausage/banana shape (DIAGNOSTIC) | Rounded | Rounded | Rounded |
| Schizont | Rarely seen in peripheral blood | Up to 24 merozoites | Rosette (8 merozoites around central pigment) | 8 merozoites |
| Merozoites | Up to 32 | Up to 24 | 8 | 8 |
| High-grade parasitemia | >10% of RBCs infected | Low | Low | Low |
MUHS Key Diagnostic Smear Features:
- P. falciparum: Multiple rings + accolé position + banana gametocytes
- P. vivax: Enlarged RBC + Schüffner dots + amoeboid trophozoite
- P. malariae: Rosette schizont + band/bar trophozoite forms
B. Rapid Diagnostic Tests (RDTs)
- Immunochromatographic lateral flow strips
- Use monoclonal antibodies against:
- HRP-2 (Histidine-Rich Protein 2) - P. falciparum specific
- pLDH (Plasmodium Lactate Dehydrogenase) - pan-malarial
- Aldolase - pan-malarial
- Results in <20 minutes
- P. falciparum RDTs: sensitivity 94-100%, specificity 94.2%
- BinaxNOW (FDA approved) detects HRP-2 and pLDH
C. Molecular Methods
- PCR (most sensitive; 18S rRNA gene target) - species differentiation, drug resistance markers
- LAMP (Loop-Mediated Isothermal Amplification) - field-deployable
- NASBA (Nucleic Acid Sequence-Based Amplification)
D. Serology
- Not for acute diagnosis; used for epidemiological surveys and blood donor screening
- Remains positive ~1 year after treatment
E. Other Tests (Non-specific)
- Anaemia (normocytic normochromic) - haemolysis
- Thrombocytopenia - very common in malaria
- Elevated LDH, bilirubin
- Leucopenia
SN 2 - Plasmodium falciparum Infections: Complications and Laboratory Diagnosis
Plasmodium falciparum - Overview
- Causes Malignant Tertian Malaria
- Most dangerous species; responsible for majority of malaria deaths
- Incubation period: 7-10 days (shortest of all species)
- No hypnozoites - no relapses from liver (only recrudescence)
- Distribution: tropical and subtropical regions
Complications of P. falciparum Malaria (★★★ MUHS FAVOURITE)
The high pathogenicity is due to:
- Infects ALL ages of RBCs (not just young or old) → massive parasitemia
- Cytoadherence: Infected RBCs adhere to vascular endothelium (via PfEMP1 - P. falciparum Erythrocyte Membrane Protein 1), forming "knobs" on RBC surface
- Rosetting: Infected RBCs bind to uninfected RBCs
- Capillary plugging: Masses of parasitized RBCs, platelets, leucocytes and malarial pigment block capillaries
- Sequestration of schizonts and trophozoites in deep capillaries → rarely seen in peripheral blood
Complications:
| Complication | Mechanism | Features |
|---|---|---|
| Cerebral Malaria (most important) | Capillary plugging of cerebral vessels; cytoadherence to brain endothelium | Coma, seizures, delirium, death; high mortality; retinal haemorrhages |
| Blackwater Fever | Massive intravascular haemolysis (especially after quinine in G6PD deficiency) | Haemoglobinuria (dark/black urine), severe anaemia, renal failure |
| Algid Malaria | Gram-negative septicaemia complicating malaria | Severe hypotension, shock, cold clammy skin |
| Hypoglycaemia | Parasite consumes glucose + quinine-stimulated insulin release | Especially in children and pregnant women |
| Severe Anaemia | Massive haemolysis of infected + innocent bystander RBCs | Hb <5 g/dL; common in children |
| Pulmonary Oedema / ARDS | Increased capillary permeability | Non-cardiogenic; very high mortality |
| Acute Renal Failure | Dehydration + haemoglobinuria + immune complex deposition | Oliguria, rising creatinine |
| Hyperparasitaemia | >5% RBCs infected (or >250,000 parasites/µL) | Poor prognostic indicator |
| DIC | Platelet activation, endothelial damage | Bleeding from multiple sites |
| Hyperpyrexia | Temperature >41°C | Convulsions, especially in children |
| Splenic Rupture | Massive splenomegaly + trauma | Acute abdomen, haemoperitoneum |
WHO Criteria for Severe Malaria: Impaired consciousness, >5% parasitemia, severe anaemia (Hb <7 g/dL), renal failure, pulmonary oedema, hypoglycaemia, shock, bleeding, hyperparasitemia, jaundice, repeated convulsions.
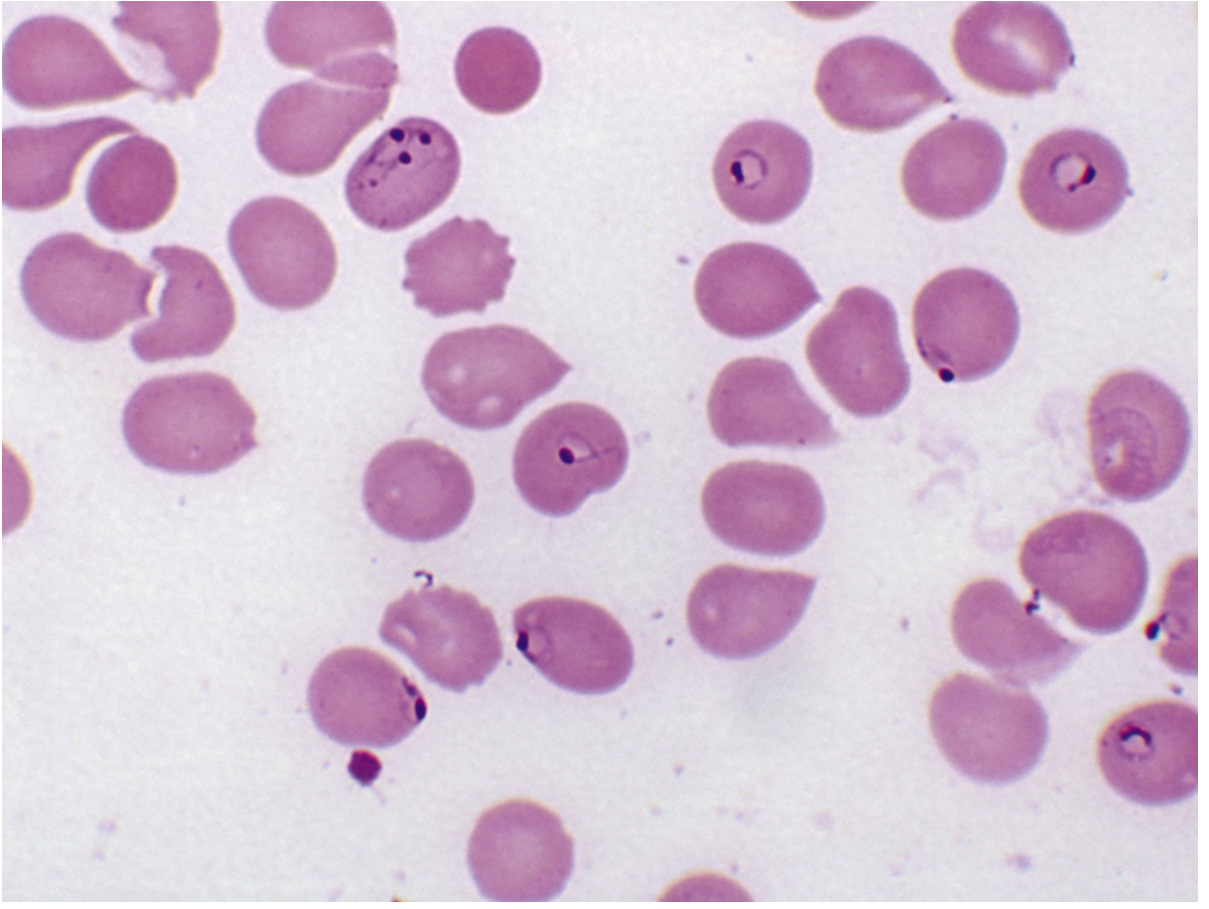
Laboratory Diagnosis of P. falciparum:
Peripheral Smear - Characteristic Features:
- Multiple ring forms within a single RBC (2 or more rings/cell)
- Rings in accolé (appliqué) position - ring appears at the periphery/margin of RBC
- No enlargement of RBC
- Schizonts and trophozoites usually absent (sequestered in deep capillaries)
- Crescentic (banana/sausage-shaped) gametocytes = PATHOGNOMONIC of P. falciparum
- Maurer dots (dots/clefts) occasionally seen
- High parasitemia (>10%) of ring forms = strongly suggestive even without gametocytes
RDTs: HRP-2 based tests highly specific for P. falciparum; sensitivity 94-100%
PCR: Detects at very low parasitemia; identifies drug-resistance markers
LAQ 1 - Malignant Tertian Malaria: Life Cycle, Complications, Laboratory Diagnosis
(This is Plasmodium falciparum malaria - covered comprehensively above. The full life cycle follows below)
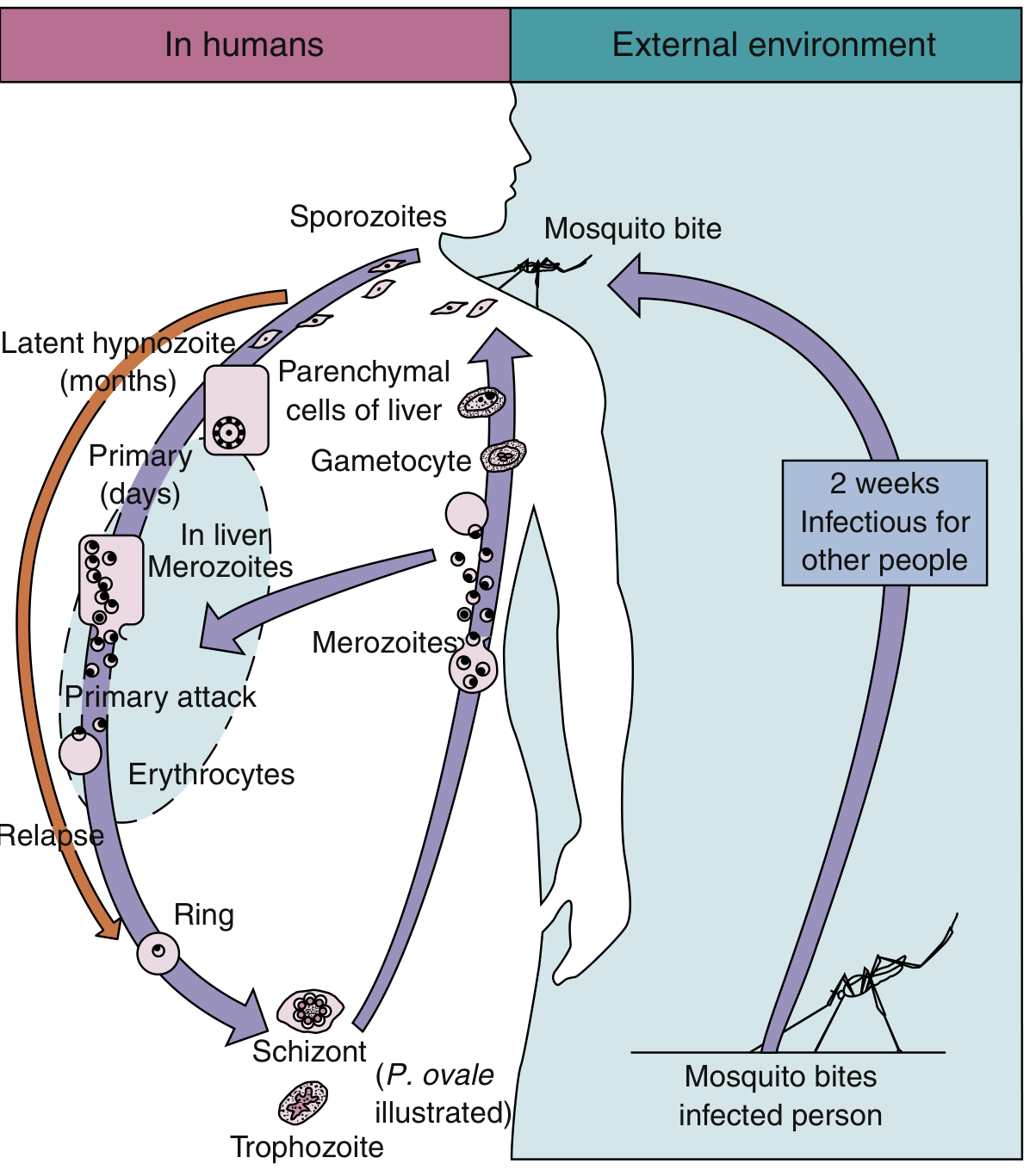
Life Cycle of Plasmodium Species (Common to All 5 Species)
Hosts:
- Definitive host: Female Anopheles mosquito (sexual reproduction occurs here)
- Intermediate/Incidental host: Humans (asexual reproduction)
Phase 1: EXOERYTHROCYTIC (Pre-erythrocytic) Cycle - in Liver
- Infected female Anopheles mosquito bites human → inoculates sporozoites via saliva
- Sporozoites enter bloodstream → travel to liver parenchymal cells within 30 minutes
- In hepatocytes: sporozoites undergo schizogony (asexual division) → liver schizont
- Liver schizont matures → 10,000-40,000 merozoites released
- Hepatocytes rupture → merozoites enter bloodstream
- Duration: 7-10 days for P. falciparum; 8-25 days depending on species
- P. vivax and P. ovale can form HYPNOZOITES (dormant forms in liver) → cause RELAPSE months to years later
- P. falciparum and P. malariae do NOT form hypnozoites (recrudescence, not relapse)
Phase 2: ERYTHROCYTIC Cycle - in RBCs
-
Merozoites attach to specific receptors on RBC surface → enter RBC
-
Ring stage (early trophozoite): ring appearance with hemozoin pigment forming
-
Growing trophozoite stage: fills RBC, pigment granules appear
-
Schizont stage: nucleus divides → merozoites formed (species-specific number)
-
RBC ruptures → merozoites released into bloodstream → infect new RBCs → FEVER PAROXYSM
-
Duration of erythrocytic cycle:
- P. falciparum, P. vivax, P. ovale: 48 hours → Tertian (fever every 48 hours, day 1 and day 3)
- P. malariae: 72 hours → Quartan (fever every 72 hours)
-
Some merozoites develop into male (microgametocyte) and female (macrogametocyte) in RBCs
Phase 3: SEXUAL Cycle (Sporogony) - in Mosquito
- Female Anopheles bites infected human → ingests blood containing mature gametocytes
- In mosquito midgut:
- Exflagellation of microgametocyte → 8 motile microgametes
- Macrogametocyte → macrogamete
- Fertilization → Zygote (non-motile)
- Zygote → elongated Ookinete (motile)
- Ookinete penetrates gut wall → forms Oocyst on outer gut wall
- Oocyst matures → contains sporozoites (10,000+)
- Oocyst ruptures → sporozoites released → migrate to salivary glands
- Ready to infect next human host
- Duration in mosquito: ~2 weeks (10-14 days at 27°C)
Malignant Tertian Malaria - Key Points:
- Caused by P. falciparum
- "Malignant" - because it is life-threatening
- "Tertian" - fever spikes every 48 hours (days 1 and 3)
- Complications listed in full in SN 2 above
LAQ 2 - Plasmodium vivax: Morphology, Life Cycle, Laboratory Diagnosis
Plasmodium vivax - Overview
- Causes Benign Tertian Malaria
- Most prevalent plasmodium species with widest geographic distribution
- Predominantly in South America and Southeast Asia
- Invades only young, immature RBCs (reticulocytes)
- Receptor: Duffy blood group antigen on RBC surface (Duffy-negative individuals (West Africans) are naturally resistant, though rare cases now reported)
- Unique feature: Forms hypnozoites in the liver → RELAPSE
Morphology of P. vivax
In Peripheral Blood (Giemsa stain):
| Stage | Features |
|---|---|
| Ring trophozoite | Large ring, 1/3 of RBC diameter; chromatin dot (double chromatin dots rare feature sometimes seen) |
| Growing trophozoite | Amoeboid, irregular, pleomorphic appearance - characteristic of P. vivax |
| Mature trophozoite | Fills most of RBC; golden-brown hemozoin (malarial pigment) granules |
| Schizont | Contains up to 24 merozoites; golden-brown pigment |
| Gametocyte | Rounded, fills the enlarged RBC |
| Infected RBC | Enlarged (1.5x normal size) |
| Schüffner dots | Pink granules in RBC cytoplasm - pathognomonic of P. vivax (also P. ovale) |
MUHS Mnemonic for P. vivax: "SAVES" - Schüffner dots, Amoeboid trophozoite, Vivid enlargement of RBC, Extra merozoites (up to 24), Sleeping forms (hypnozoites)
Life Cycle of P. vivax
(Same general life cycle as described in LAQ 1 above - key specific features for P. vivax:)
- Exoerythrocytic phase: 8 days (some sporozoites become HYPNOZOITES)
- Hypnozoites: Dormant liver stage; can reactivate after months to years → RELAPSE
- Erythrocytic cycle: 48 hours → Tertian fever (every 48 hours)
- Schizont: Up to 24 merozoites
- Gametocytes: Rounded, fill enlarged RBC
Only P. vivax and P. ovale form hypnozoites → hence the term "relapsing malaria"
Treatment to prevent relapse: Primaquine (targets liver hypnozoites)
Clinical Features of P. vivax Malaria:
- Incubation period: 10-17 days (short incubation); can be months if hypnozoites
- Prodrome: Vague flu-like illness - headache, myalgia, photophobia, anorexia
- Classic Malarial Paroxysm (every 48 hours - tertian pattern):
- Cold stage: Chills, rigors (shivering) - 15 min to 1 hour
- Hot stage: High fever 103-106°F, headache, vomiting - 2-6 hours
- Sweating stage: Profuse sweating, fever drops, exhaustion - 2-4 hours
- Splenomegaly - progressive
- Anaemia - progressive haemolytic
- Recent evidence: P. vivax can also cause severe disease - pulmonary oedema, renal failure, cerebral involvement (not just P. falciparum)
Laboratory Diagnosis of P. vivax:
1. Peripheral Blood Smear (Gold Standard)
- Thick film: Screening; detect presence of parasites
- Thin film: Species identification (Giemsa/Leishman stain)
- Characteristic features:
- Enlarged RBC with Schüffner dots (pink granules)
- Amoeboid growing trophozoite
- Schizont with up to 24 merozoites
- Rounded gametocyte filling enlarged RBC
- Best time: Between paroxysms (4-6 hours after fever) when peak parasitemia
2. Rapid Diagnostic Tests (RDTs)
- Anti-pLDH (pan-malarial) and anti-aldolase antibody tests
- Specific P. vivax pLDH-based tests available
- Sensitivity 67-86% for P. vivax (lower than for falciparum)
- Not recommended as sole diagnostic test for P. vivax in low-endemic settings
3. Serology
- IFAT, ELISA - used for epidemiological studies, not acute diagnosis
- Cross-react with other Plasmodium species
4. PCR
- Highest sensitivity for P. vivax
- Used for mixed infections and species confirmation
- Detects P. vivax at very low parasitemia (sub-microscopic infections)
5. Other supportive tests:
- Anaemia (normocytic normochromic)
- Thrombocytopenia
- Elevated bilirubin (indirect/unconjugated)
- Elevated LDH
- Leucopenia
MUHS TREATMENT TIPS:
- Chloroquine: For blood-stage P. vivax (in sensitive areas)
- Primaquine: Essential to eliminate hypnozoites and prevent relapse; check G6PD before giving (causes haemolysis in G6PD-deficient patients)
QUICK COMPARISON TABLE - All Plasmodium Species (MUHS EXAM FAVOURITE)
| Feature | P. falciparum | P. vivax | P. malariae | P. ovale |
|---|---|---|---|---|
| Malaria type | Malignant Tertian | Benign Tertian | Quartan | Benign Tertian |
| Fever cycle | 48 hrs | 48 hrs | 72 hrs | 48 hrs |
| RBC preference | All ages | Reticulocytes | Old RBCs | Reticulocytes |
| RBC size | Normal | Enlarged | Normal | Slightly enlarged |
| Stippling | Maurer dots (clefts) | Schüffner dots | Ziemann dots | Schüffner dots |
| Trophozoite | Multiple rings, accolé | Amoeboid | Band/bar forms | Compact |
| Schizont in blood | ABSENT (sequestered) | Up to 24 merozoites | Rosette, 8 merozoites | 8 merozoites |
| Gametocyte | Crescent/banana | Rounded | Rounded | Rounded |
| Hypnozoites | ABSENT | PRESENT | ABSENT | PRESENT |
| Relapse | No (recrudescence only) | Yes | No | Yes |
| HRP-2 test | POSITIVE | Negative | Negative | Negative |
| Incubation | 7-10 days | 10-17 days | 18-40 days | 10-17 days |
| Mortality | Highest | Low | Very low | Very low |
KEY EXAM MNEMONICS
LD Body = Large nucleus + Distinctive rod kinetoplast - inside macrophage
Giardia Findings = "FAT MAN"
- Foul-smelling greasy stool
- Acute diarrhea (self-limited 7-10 days)
- Trophozoites with "falling leaf" motility
- Malabsorption in chronic form
- Antigenic detection by ELISA
- No blood/mucus in stool
P. falciparum Complications = "BEACH HARP"
- Blackwater fever
- Encephalopathy (Cerebral malaria)
- ARDS / pulmonary oedema
- Coagulopathy (DIC)
- Hypoglycaemia
- Hyperparasitemia
- Anaemia (severe)
- Renal failure
- Pancytopenia
Sources: Medical Microbiology 9e (Murray et al.); Tietz Textbook of Laboratory Medicine 7e; Medical Microbiology (standard references)
This is a shared conversation. Sign in to Orris to start your own chat.