Volkmann ischemic contracture 10 marks pg orthopaedics answer with flow chart and images
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
I now have sufficient information to write a comprehensive 10-mark PG orthopaedics answer. Let me compile the complete answer with flowcharts and images.
Volkmann Ischemic Contracture (VIC)
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine
Definition
Volkmann Ischemic Contracture is the classic sequela of untreated or inadequately treated acute compartment syndrome of the forearm, resulting in progressive muscle ischemia, myonecrosis, fibrosis, and a characteristic deformity of the forearm and hand. First described by Richard von Volkmann (19th century German surgeon), who attributed it to trauma, swelling, and tight bandaging.
Etiology / Causes
| Category | Examples |
|---|---|
| Fractures (most common) | Supracondylar humerus fracture (classic in children), forearm fractures, distal radius fractures |
| Soft tissue injury | Crush injury, vascular injury, reperfusion injury |
| Iatrogenic | Tight casts/bandages, circumferential dressings, prolonged tourniquet, IV extravasation |
| Vascular | Brachial artery injury/spasm, embolism |
| Burns | Circumferential burns of forearm |
| Anticoagulants/Bleeding disorders | Spontaneous hematoma causing compartment rise |
The supracondylar fracture of the humerus is the single most common cause, classically in children, compromising the brachial artery (and median nerve) at the elbow.
Pathophysiology
Vicious Cycle of Compartment Syndrome
PRECIPITATING EVENT (fracture/injury/tight cast)
│
▼
↑ Intracompartmental Pressure
│
▼
Venous outflow obstruction
(arterial inflow initially preserved)
│
▼
↑ Venous pressure → ↓ AV gradient
│
▼
Tissue ischemia (capillary insufficiency)
│
▼
Inflammatory cytokines released
↑ Capillary permeability → MORE EDEMA
│
▼
Further ↑ Compartment Pressure
│
▼
Arterial inflow disrupted
│
▼
Muscle necrosis → Myoglobin release
(risk: renal failure, arrhythmia)
│
▼
Muscle fibrosis & contracture = VIC
Why the Forearm Flexors are Most Vulnerable
The anatomy of the forearm creates a "cruciate portal" where ischemia preferentially affects the deep flexors:
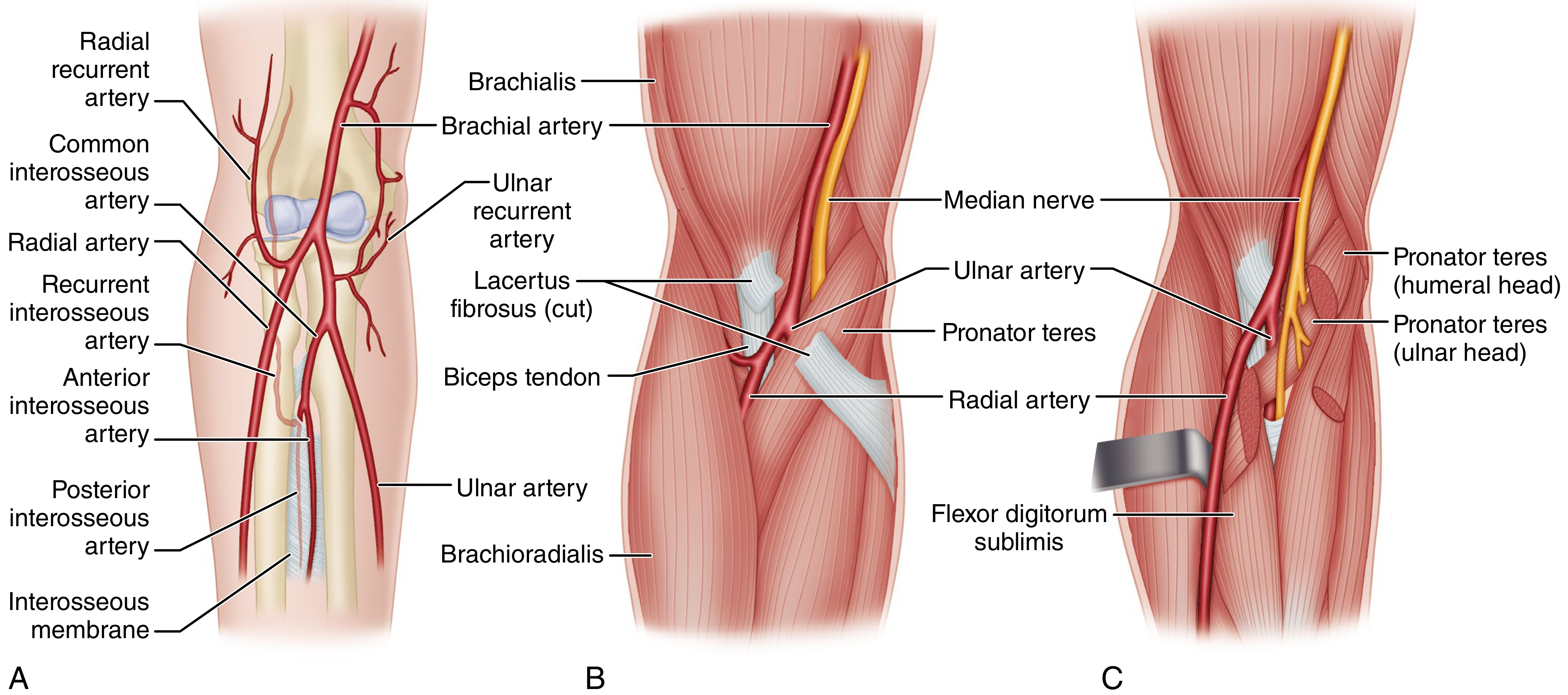
Figure: Volkmann ischemia anatomy. (A) Collateral circulation of elbow does NOT communicate with vessels within the flexor compartment. (B) Brachial artery and median nerve enter the forearm through the tight opening formed by the biceps tendon and pronator teres, covered by the lacertus fibrosus - any proximal compression here causes major neurovascular compromise. (C) Ulnar artery passes beneath pronator teres and lies in the deepest compartment, explaining why FDP is most vulnerable.
- FDP (Flexor Digitorum Profundus) and FPL (Flexor Pollicis Longus) lie deepest - most ischemia-prone
- Nerves (median > ulnar) also undergo strangulation within the fibrotic mass
Clinical Features
Acute Stage (Compartment Syndrome - 6 Ps)
| Sign | Details |
|---|---|
| Pain | Out of proportion to injury; earliest and most sensitive sign |
| Pain on passive stretch | Passive finger extension causes severe forearm pain |
| Pressure | Tense, woody hardness of forearm compartment |
| Paresthesia | Tingling, numbness (median > ulnar distribution) |
| Paralysis | Weakness of finger/wrist flexion |
| Pallor / Pulselessness | Late signs - absence does NOT rule out compartment syndrome |
Established VIC (Deformity Pattern)
The classic posture of established Volkmann contracture:
- Elbow flexion
- Forearm pronation
- Wrist flexion
- Thumb adduction
- MCP joint extension
- IP joint flexion ("intrinsic minus" / claw hand)

Figure: Abduction contracture of the fifth finger from ischemic myositis of abductor digiti quinti secondary to compressive bandage - demonstrating localized Volkmann ischemic process.
Key test: Wrist flexion increases finger extension range (pseudoparalysis sign) - when wrist is flexed, fingers can be straightened; when wrist is extended, fingers curl into flexion.
Classification (Seddon's Classification)
┌─────────────────────────────────────────────────────────────────────────┐
│ VOLKMANN'S CLASSIFICATION │
├──────────────┬──────────────────────────────┬───────────────────────────┤
│ SEVERITY │ FINDINGS │ TREATMENT │
├──────────────┼──────────────────────────────┼───────────────────────────┤
│ │ • Partial ischemia of FDP │ │
│ MILD │ • 2-3 fingers flexion │ • Physiotherapy │
│ (Localized) │ contracture │ • Dynamic splinting │
│ │ • No/minimal sensory change │ • Tendon lengthening/ │
│ │ • No intrinsic contracture │ release (after 3 months)│
├──────────────┼──────────────────────────────┼───────────────────────────┤
│ │ • All finger & thumb flexors │ • Muscle sliding operation│
│ MODERATE │ • Possible wrist flexors │ • Neurolysis (median + │
│ │ • Median + ulnar sensory │ ulnar nerves) │
│ │ changes │ • ± Carpal resection / │
│ │ • Intrinsic minus deformity │ bone shortening │
├──────────────┼──────────────────────────────┼───────────────────────────┤
│ │ • Flexors AND extensors │ • Excision of all │
│ SEVERE │ • Wrist flexion contracture │ necrotic muscles │
│ │ • Forearm pronation │ • Complete neurolysis │
│ │ • Severe median + ulnar │ • Tendon transfers: │
│ │ sensory/motor deficits │ BR → FPL, ECRL → FDP │
│ │ • Claw hand deformity │ • Free gracilis transfer │
└──────────────┴──────────────────────────────┴───────────────────────────┘
FDP = Flexor digitorum profundus; FPL = Flexor pollicis longus; BR = Brachioradialis; ECRL = Extensor carpi radialis longus
Management Flowchart
SUSPECTED COMPARTMENT SYNDROME
│
▼
┌──────────────────────────┐
│ Clinical Assessment │
│ - 6 Ps │
│ - Pain on passive stretch│
│ - Tense compartment │
└──────────┬───────────────┘
│
▼
Remove all constricting casts/bandages
│
▼
Compartment Pressure Measurement
(Stryker device / arterial line transducer)
│
┌──────┴──────┐
│ │
P < 30 mmHg P ≥ 30 mmHg OR
(ΔP > 30) ΔP ≤ 30 mmHg*
│ │
▼ ▼
Monitor EMERGENCY FASCIOTOMY
closely (within 6 hours)
│
▼
┌─────────────────────────────┐
│ FOREARM FASCIOTOMY │
│ • Volar + Dorsal incisions │
│ • Carpal tunnel release │
│ • Mobile wad release │
└─────────────┬───────────────┘
│
▼
Wound left open
Delayed primary closure
or skin grafting (48-72h)
│
┌────────┴────────┐
│ │
Success Established VIC
│ │
Healed ┌────┴────────────────────────┐
│ │
MILD MODERATE/SEVERE
│ │
Physiotherapy Surgical reconstruction:
Dynamic splinting • Muscle slide (Page-Scaglietti)
Tendon lengthening • Necrotic muscle excision
(after 3 months) • Neurolysis (median + ulnar)
• Tendon transfers
• Free gracilis transfer (severe)
ΔP = Diastolic BP - Compartment Pressure; threshold ≤ 30 mmHg = surgical indication
Treatment in Detail
1. Prevention (Most Important)
- Early recognition of compartment syndrome
- Remove tight casts/splints immediately
- Urgent fasciotomy - do NOT delay
2. Acute Management
- Fasciotomy: Emergent, double-incision technique (volar S-shaped + dorsal straight incision)
- Bivalve plaster, elevation (not above heart level)
- Wound closure: delayed primary closure at 48-72 hours or split-skin graft
3. Established VIC - by Grade
Mild Contracture:
- Physiotherapy, dynamic extension splinting
- Active muscle use
- After 3 months: Tendon lengthening (Z-plasty or step-cut) of FDP/FDS
- Muscle sliding operation if multiple tendons involved
Moderate Contracture:
- Muscle sliding operation (Page-Scaglietti): Detaches the muscle origins from the humerus/ulna; allows the muscle-tendon units to "slide" distally, correcting the contracture
- Neurolysis of median and ulnar nerves
- Excision of fibrotic muscle mass
- Adjuncts: Wrist/carpal resection, bone shortening if needed
Severe Contracture:
- Excision of ALL necrotic muscles (fibrotic, non-contractile tissue)
- Complete median + ulnar neurolysis (median nerve may show hourglass deformity at mid-forearm)
- Tendon transfers: Brachioradialis → FPL, ECRL → FDP (to restore finger flexion)
- Free innervated gracilis muscle transfer: Selected cases where no motors remain; good/M3-M4 results reported
- Free medial gastrocnemius myocutaneous flap: Alternative for reconstruction
Complications
| Complication | Notes |
|---|---|
| Permanent finger/wrist contracture | If not treated promptly |
| Intrinsic minus (claw) hand | Severe involvement |
| Median/Ulnar nerve palsy | Strangulation by fibrotic muscle |
| Myoglobinuria / Renal failure | From acute massive myonecrosis |
| Volkmann ischemia of lower limb | Tibial compartment syndrome |
| Growth disturbance | In children - physis damage |
Key Examination Points (PG Focus)
- Classic cause: Supracondylar humerus fracture in children
- Most vulnerable muscles: FDP and FPL (deepest compartment)
- Earliest sign of compartment syndrome: Pain on passive stretch
- Pulselessness is a LATE sign - do not wait for absent pulse to act
- "Safe" compartment pressure: < 30 mmHg (or ΔP > 30 mmHg)
- Time window for fasciotomy: < 6 hours for best outcome
- Muscle sliding operation (Page-Scaglietti): Treatment of moderate VIC
- Gracilis free muscle transfer: For severe VIC with no remaining motors
- Wrist posture test: Flexing wrist allows passive IP extension - confirms VIC
- Artery and nerve compromised: Brachial artery + Median nerve (from Sabiston review tables)
References:
- Campbell's Operative Orthopaedics 15th Ed 2026, Ch. 79 - Compartment Syndrome and Volkmann Contracture
- Miller's Review of Orthopaedics 9th Edition, Ch. 7 - Hand Surgery
- Sabiston Textbook of Surgery - Acute Compartment Syndrome
- Tintinalli's Emergency Medicine - Complications of Supracondylar Fractures
This is a shared conversation. Sign in to Orris to start your own chat.