Anti glide plating mechanism
Reading File
Finding Sources
Searching the Web
anti-glide plating mechanism orthopedic fracture fixation
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of anti-glide plating, sourced from Rockwood and Green's Fractures in Adults (10th ed, 2025) and the AO Foundation.
Anti-Glide Plating - Mechanism and Principles
Definition
Anti-glide plating is a method of fracture fixation where the plate is positioned to physically block the mobile fracture fragment from "gliding" (translating/shortening) along the fracture plane under axial load. The plate does not primarily generate compression itself - it prevents displacement.
"Antiglide plating is a term many surgeons use to describe plating of shearing-type fractures where the plate primarily acts to prevent shortening (whereas a buttress plate also applies compression). Antiglide plates are often shorter than buttress plates and generally rely on lag screws to generate compression."
- Rockwood and Green's Fractures in Adults, 10th ed.
Biomechanical Mechanism
The key concept is the "axilla" effect:
- The plate is placed at the apex of the fracture, on the side toward which the distal fragment would tend to displace
- The proximal edge of the plate, sitting just proximal to the fracture line, forms an "axilla" (armpit) with the intact cortex
- Under axial loading, when the distal fragment tries to slide proximally along the oblique fracture surface, the plate's proximal edge acts as a physical block - the fragment cannot ride up past the plate
- This converts shear forces at the fracture site into compressive forces across the fracture plane
- Lag screws (through or separate from the plate) provide interfragmentary compression
Critical plate positioning: The proximal hole nearest the fracture should sit 3-5 mm proximal to the fracture line. If the plate is improperly positioned or over-contoured, bony contact at the apex is lost and the anti-glide effect fails.
Anti-Glide vs. Buttress Plating - Key Distinction
| Feature | Anti-Glide | Buttress |
|---|---|---|
| Fracture type | Diaphyseal oblique/spiral | Metaphyseal/partial articular (OTA B-type) |
| Primary function | Prevents shortening/sliding | Also generates compression |
| Plate length | Shorter | Longer |
| Compression source | Lag screws | Undercontoured plate + axillary screw |
| Environment | Usually relative stability | Absolute stability, primary bone healing |
The terms are frequently used interchangeably in clinical practice, but the distinction matters mechanically.
Prototype Application: Distal Fibula (Weber B / Denis-Weber B)
The classic example is a posterolateral plate on the distal fibula for an oblique lateral malleolus fracture:
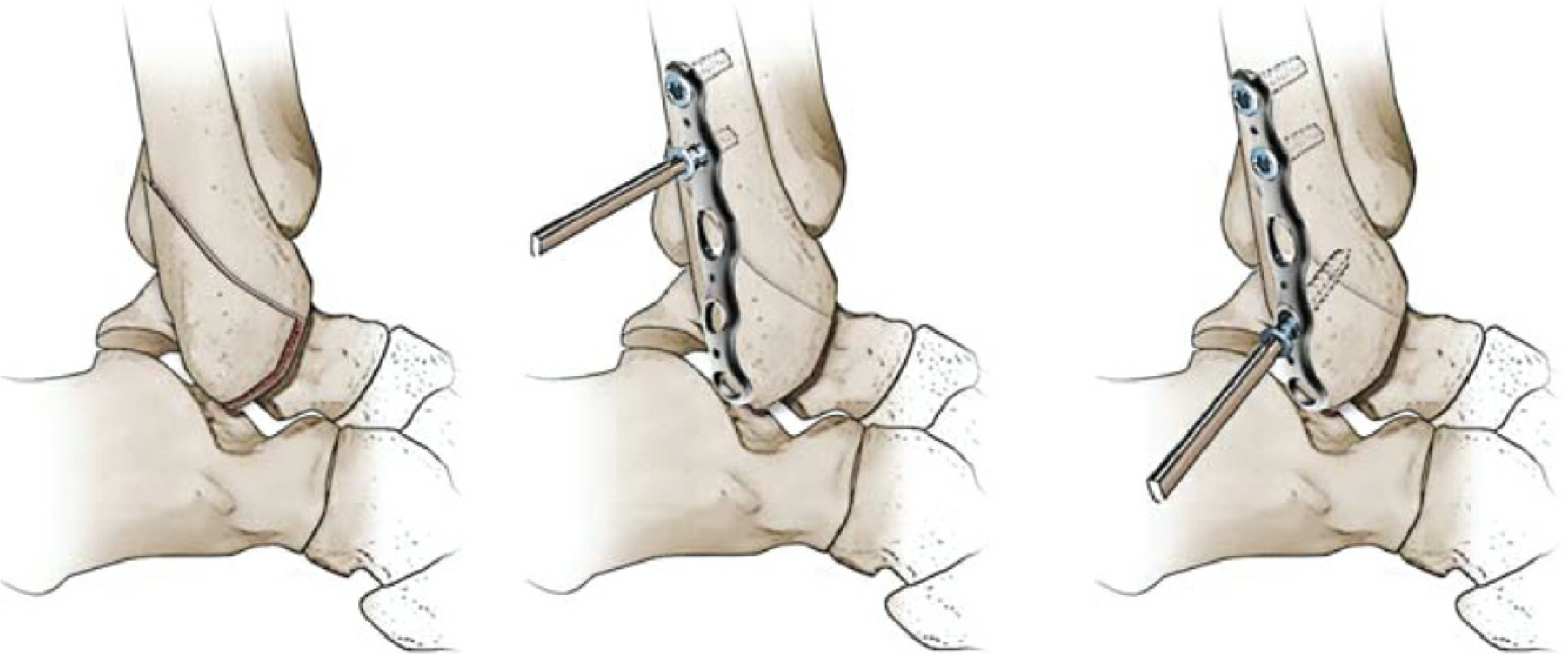
Antiglide technique for a type B distal fibular fracture - the plate is applied posteriorly, with a lag screw supplementing interfragmentary compression. (Rockwood and Green's, 10th ed, Fig. 13-23)
- The fracture line runs obliquely from anteroinferior to posterosuperior
- With axial load (walking), the distal fragment tends to ride proximally and posteriorly
- The posterior plate sits directly in the path of this displacement
- The proximal plate edge "catches" the distal fragment at the fracture apex
- A lag screw is typically added through the plate across the fracture for interfragmentary compression
- Advantages: lower soft tissue profile compared to a lateral plate, less wound complication risk, potentially stronger construct
Other Locations
- Medial malleolus - anti-glide plating used as an alternative to lag screws for oblique medial malleolar fractures
- Femoral neck - medial anti-glide plate at the medial apex for certain femoral neck fracture patterns (Mir and Collinge technique)
- Posterior malleolus - posterior plate in anti-glide mode for posterior tibial plafond fractures
Plate Contouring Rules
- Slightly undercontoured at the apex - this ensures the plate contacts bone at the fracture apex when screws are tightened, maximizing the blocking/axilla effect
- If over-contoured (plate bows away from bone at apex): no contact at apex, anti-glide effect lost, fragment can still displace
- If under-contoured too aggressively: tightening screws can actually displace the fracture
Summary
The anti-glide plate works by geometric obstruction - it sits proximal to the fracture apex on the tension/displacement side, physically blocking the distal fragment from sliding along the fracture plane. Lag screws generate compression; the plate prevents shortening and rotational displacement. It is not a neutralization plate (which only protects a lag screw) and is not a pure compression plate.
- Source: Rockwood and Green's Fractures in Adults, 10th ed (2025), Chapter 12 - Buttress and Antiglide Plating section; Chapter 13
- AO Foundation Surgery Reference - Antiglide Plate technique
This is a shared conversation. Sign in to Orris to start your own chat.