Treatment of haemangioma in paediatric 7 month baby
Reading File
Finding Sources
Searching PubMed
infantile hemangioma treatment propranolol
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, evidence-based guide to the treatment of infantile haemangioma (IH) in a 7-month-old infant.
Treatment of Infantile Haemangioma in a 7-Month-Old
Background: Why 7 Months Matters
A 7-month-old is at a critical juncture. Infantile haemangiomas (IH) typically proliferate rapidly in the first 3-5 months, with 80% of growth completed by 3 months and near-maximal size by 5 months. By 7 months, many IH are at or near peak size and are entering a plateau before spontaneous involution begins (usually around 12 months). This makes 7 months an important window - treatment initiated now can still meaningfully alter the growth trajectory and prevent complications.
Step 1: Decision to Treat
Not all IH require active treatment. The majority of small, uncomplicated IH can be observed, as ~50% involute by age 5 years and ~70% by age 7 years. However, treatment is indicated in the following circumstances:
| Indication | Examples |
|---|---|
| Life-threatening | Airway (subglottic) IH, hepatic IH with high-output cardiac failure or hypothyroidism |
| Function-threatening | Periocular (amblyopia risk), nasal tip, lip/oral |
| Ulceration | Especially in nappy area, lip, neck folds |
| Disfigurement risk | Large facial IH, beard distribution (airway risk), segmental IH |
| Psychosocial concern | Large or prominent lesions causing significant distress |
| PHACE or LUMBAR syndrome | Segmental IH with associated structural anomalies |
Step 2: First-Line Treatment - Oral Propranolol
Oral propranolol is the gold-standard first-line treatment for IH requiring systemic therapy. It received FDA approval in 2014 specifically for this indication. At 7 months, your patient is well within the treatment window.
Mechanism of Action
Propranolol's benefit in IH was discovered serendipitously in 2008. It works via:
- Vasoconstriction (immediate color change)
- Inhibition of angiogenesis and VEGF signaling
- Induction of apoptosis in proliferating endothelial cells
Dosing Protocol
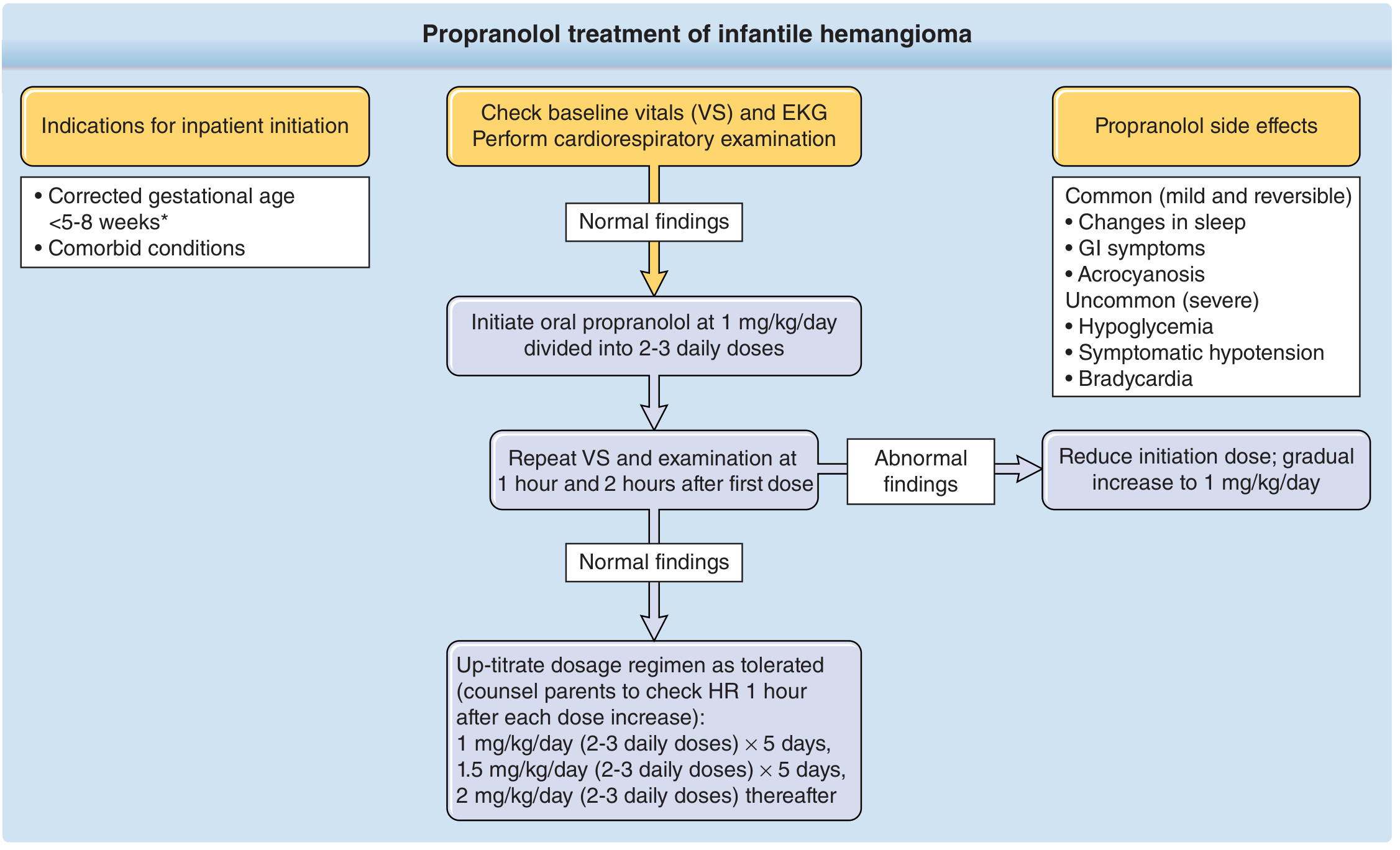
Before starting:
- Take family history (congenital heart disease, arrhythmia, maternal connective tissue disease)
- Baseline vitals (HR, BP) and EKG
- Cardiorespiratory examination
Initiation:
- Start: 1 mg/kg/day divided into 2-3 daily doses
- Escalate by 0.5 mg/kg/day every 3-7 days
- Target dose: 2-3 mg/kg/day (most practitioners use 2 mg/kg/day)
- Always dose with or just after feeds to prevent hypoglycaemia
Monitoring:
- Monitor HR and BP at 1 hour and 2 hours after first dose
- A 7-month-old otherwise healthy infant is suitable for outpatient initiation
- Inpatient initiation is recommended if corrected gestational age <5-8 weeks, comorbid cardiac/respiratory conditions, or inadequate social support
Duration: Continue until at least 12 months of age, and often until 15-18 months, then taper gradually. Rebound growth can occur with abrupt cessation.
Step 3: Alternative/Adjunct Systemic Options
| Drug | Notes |
|---|---|
| Atenolol (β1-selective) | Preferred if bronchial reactivity is a concern; no liquid formulation in some countries |
| Nadolol (non-selective β-blocker) | Cannot cross blood-brain barrier - less CNS side effects; not available in liquid form in the US |
| Oral corticosteroids | Prednisolone 2-3 mg/kg/day - used pre-propranolol era; now largely replaced but may have a role in PHACE syndrome where propranolol carries cardiovascular risk |
Step 4: Topical Therapy
Topical timolol 0.5% gel (non-selective beta blocker, 8-10x more potent than propranolol) is suitable for small, superficial, uncomplicated IH where systemic therapy is not warranted. Applied twice daily. It has minimal systemic absorption and is well tolerated. Best for thin, flat lesions; less effective for deep or mixed components.
Step 5: Interventional Options
| Modality | Role |
|---|---|
| Pulsed Dye Laser (PDL) | Adjunct for residual telangiectasias, superficial thin lesions, or post-involution residua; not first-line for bulk lesions |
| Nd:YAG laser | Deeper penetration; used for thicker lesions but higher risk profile in infants |
| Surgical excision | Reserved for lesions causing functional compromise unresponsive to medical therapy, or for post-involution fibrofatty residua in older children |
| Intralesional corticosteroids | Rarely used now; option for small localised lesions (e.g., periorbital) when systemic therapy not suitable |
Side Effects of Propranolol to Counsel Parents About
Common (mild/reversible):
- Sleep disturbances (restlessness, nightmares, insomnia) - ~11% of patients
- GI symptoms (nausea, diarrhoea)
- Acrocyanosis
Uncommon (serious):
- Hypoglycaemia - most feared; mitigated by dosing with feeds and holding dose during illness/poor intake
- Symptomatic bradycardia
- Hypotension
- Bronchospasm (use atenolol if reactive airway disease)
Special Scenarios at 7 Months
- Periocular IH: Treat urgently even if small - risk of amblyopia from visual axis obstruction or astigmatism; ophthalmology referral mandatory
- Subglottic/airway IH: ENT referral + propranolol; may need airway evaluation
- Hepatic IH: Thyroid function (TSH, T3) must be checked - risk of consumptive hypothyroidism
- PHACE syndrome (segmental facial IH + structural anomalies): Cardiology workup before propranolol; MRI/MRA of head and neck; risk of arterial stroke with propranolol-induced hypotension
- Ulcerated IH: Wound care (barrier cream, non-adherent dressings) + treat the underlying IH with propranolol; PDL can accelerate ulcer healing
Evidence Summary (Recent Literature)
Recent meta-analyses confirm propranolol's superiority:
- Hu et al., 2026 (PMID 41700540) - Systematic review and meta-analysis: propranolol superior to other drugs for IH treatment with acceptable safety profile
- Huang et al., 2024 (PMID 39687294) - Meta-analysis: oral propranolol and topical timolol both effective; oral propranolol preferred for significant/deep lesions
- Chaple Gil et al., 2025 (PMID 40404110) - Systematic review: laser therapy (PDL) effective for superficial and residual lesions; not first-line for bulk treatment
Summary Algorithm for a 7-Month-Old
Is treatment indicated? (functional risk, ulceration, significant disfigurement)
|
YES
|
Superficial + small? Deep/mixed/large/functional risk?
| |
Topical timolol 0.5% gel Oral propranolol 2 mg/kg/day
| |
Reassess at 4-6 weeks Continue to 12-15 months
Taper before stopping
Sources: Fitzpatrick's Dermatology, 9th ed., Chapter 118; Fitzpatrick's block18
This is a shared conversation. Sign in to Orris to start your own chat.