Inter costal nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile a thorough answer.
Intercostal Nerves
Origin
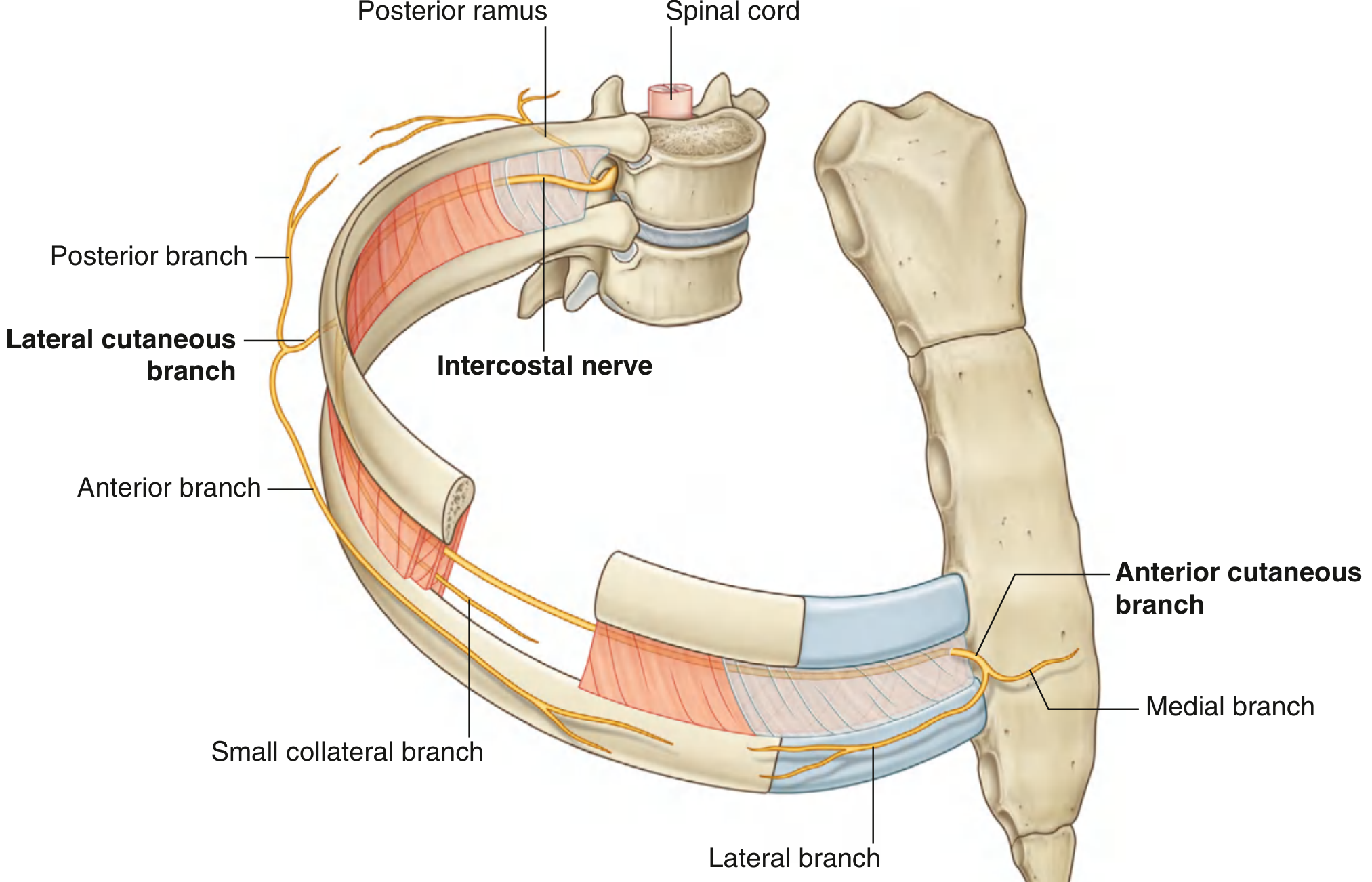
The intercostal nerves are the anterior rami of thoracic spinal nerves T1 to T11. They lie in the intercostal spaces between adjacent ribs. The anterior ramus of T12 (the subcostal nerve) runs inferior to rib XII and is not technically an intercostal nerve, though it is closely related.
- Gray's Anatomy for Students, p. 193-195
Course and Position in the Intercostal Space
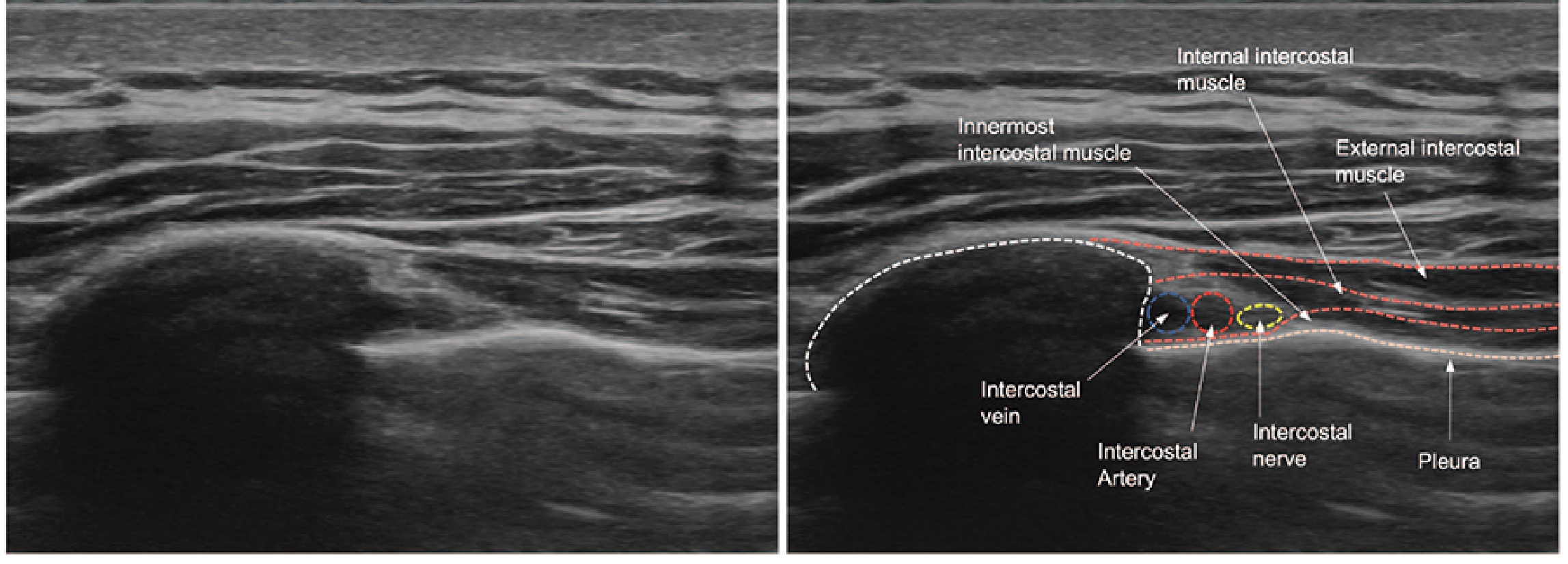
Each nerve runs in the subcostal groove on the inferior (inner) surface of its corresponding rib, between the internal intercostal muscle and the innermost intercostal muscle. The neurovascular bundle arrangement from top to bottom is:
V - A - N (Vein, Artery, Nerve)
The nerve is the most inferior structure in the groove.
Fiber Types Carried
Each intercostal nerve carries three types of fibers:
- Somatic motor - to muscles of the thoracic wall (intercostal, subcostal, and transversus thoracis)
- Somatic sensory - from skin and parietal pleura
- Postganglionic sympathetic fibers - to the periphery
Branches of a Typical Intercostal Nerve
| Branch | Origin | Distribution |
|---|---|---|
| Lateral cutaneous branch | Mid-axillary line | Divides into anterior and posterior branches; supplies overlying skin of the trunk |
| Anterior cutaneous branch | Terminal branch | Emerges parasternally (or anteriorly on abdominal wall); supplies anterior chest/abdominal skin |
| Small collateral branch | Within intercostal space | Runs along the superior border of the lower rib |
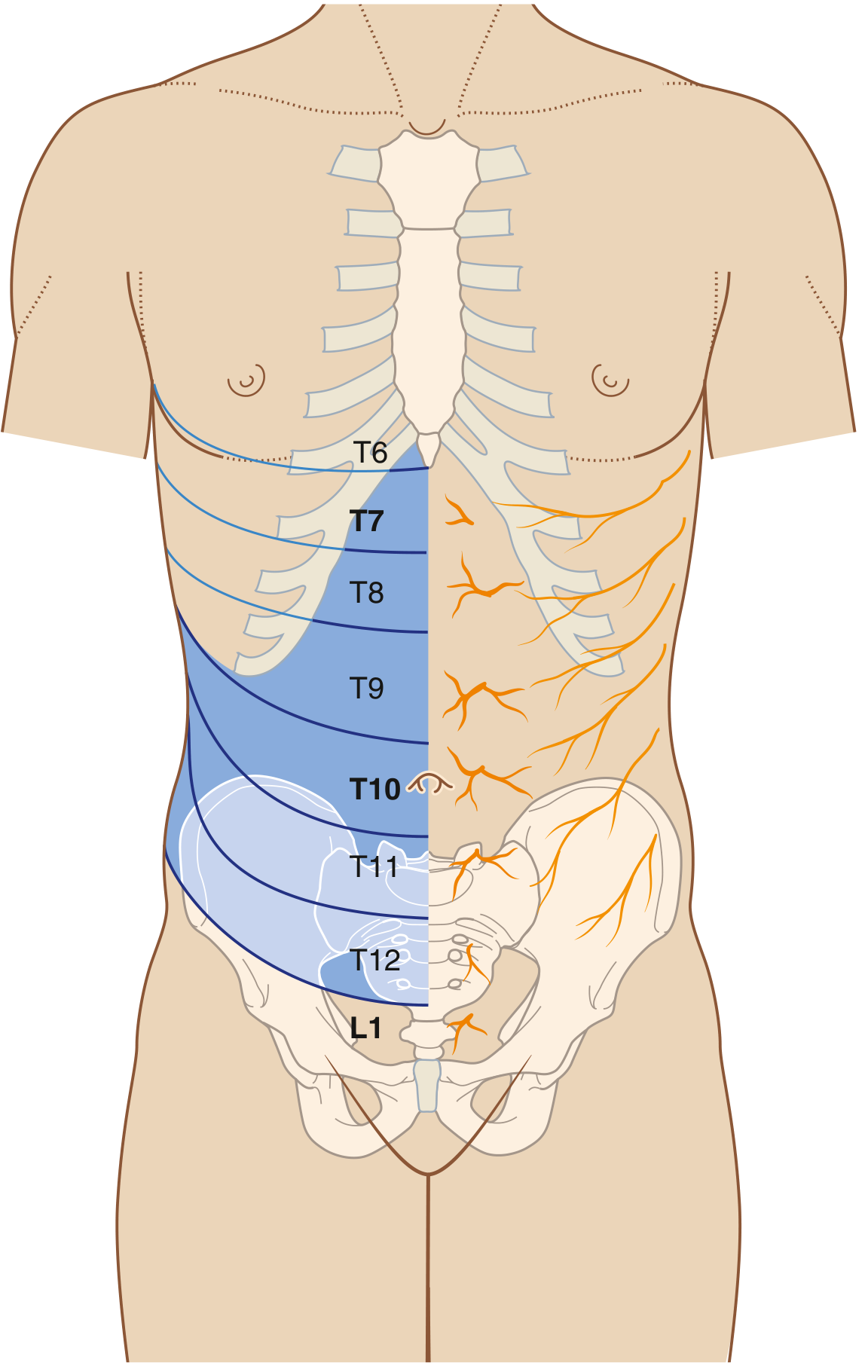
Segmental Landmarks (Dermatomes)
| Level | Surface landmark |
|---|---|
| T4 | Nipple line |
| T6 | Xiphoid process |
| T10 | Umbilicus |
| T12 | Suprapubic/inguinal |
Special/Atypical Intercostal Nerves
- T1 - Most of the anterior ramus contributes to the brachial plexus (C5-T1). Only a small branch enters the first intercostal space.
- T2 (intercostobrachial nerve) - The lateral cutaneous branch of T2 crosses the axilla and supplies the medial surface of the upper arm. This is important in breast/axillary surgery as it is often sacrificed, causing sensory loss in the axilla and inner arm.
- T7-T11 - Follow the inferior slope of the lateral ribs and cross the costal margin to enter the abdominal wall, supplying muscles and skin there.
- T12 (subcostal nerve) - Travels below rib XII to supply the abdominal wall and iliac skin.
Neurovascular Bundle - Ultrasound View
The intercostal neurovascular bundle lies deep to the external and internal intercostal muscle layers, and superficial to the innermost intercostal muscle:
Clinical Applications
1. Chest Tube Insertion
Always insert at the upper margin of a rib to avoid the neurovascular bundle (vein, artery, nerve) that runs in the subcostal groove. The recommended site is the 7th-8th intercostal space, posterior axillary line, for pleural effusion.
- THIEME Atlas of General Anatomy, p. 228
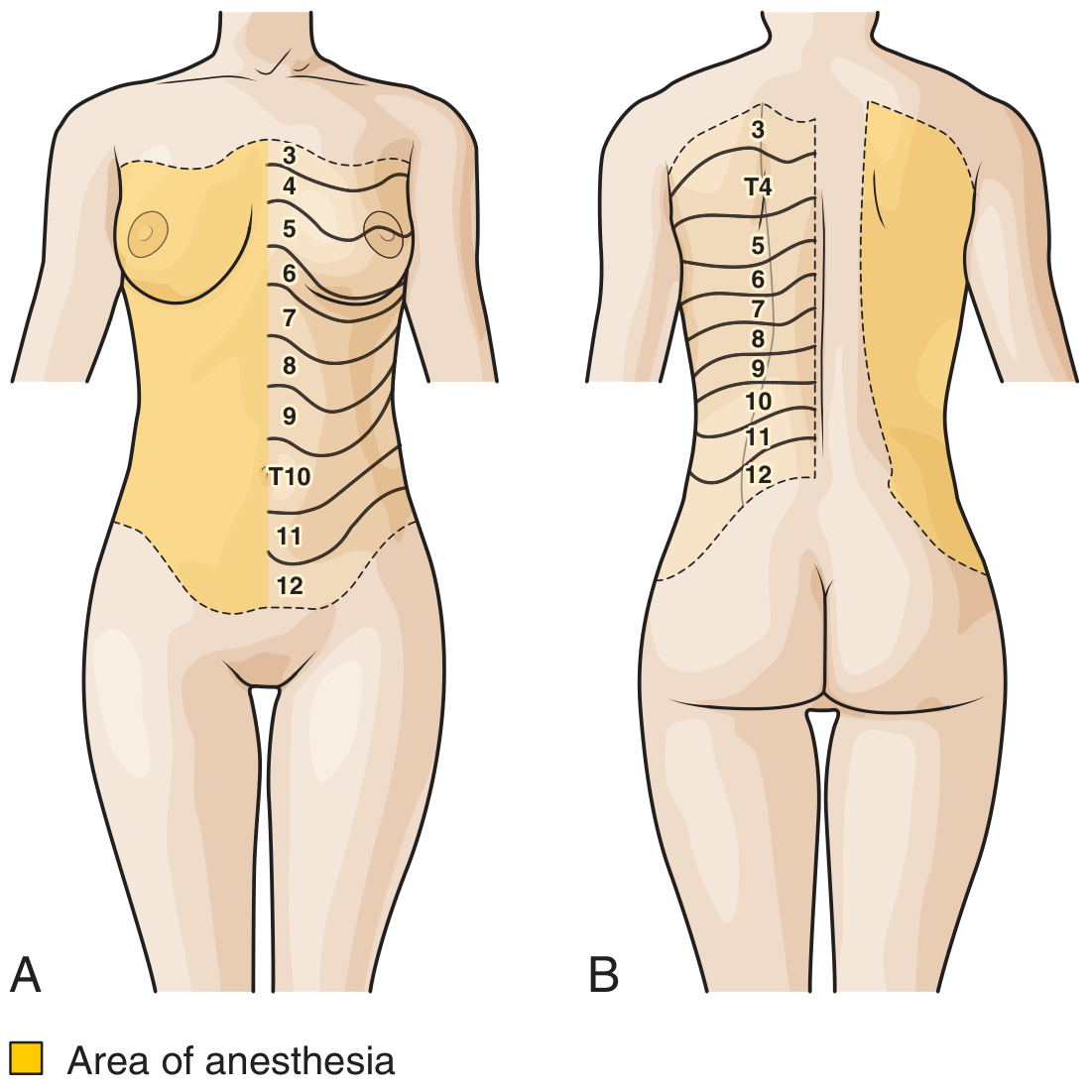
2. Intercostal Nerve Block
Used for analgesia in:
- Rib fractures
- Post-thoracotomy pain
- Tube thoracostomy
- Mastectomy/upper abdominal surgery
- Herpes zoster (shingles) affecting the chest wall
Technique: Needle inserted at the rib angle (~6 cm lateral to midline), advancing to the subcostal groove with the needle angled cephalad at 10-15 degrees. Deposit 2-5 mL of local anesthetic. Blocking posterior to the mid-axillary line ensures coverage of both the lateral cutaneous and anterior branches.
Duration: 8-18 hours with long-acting local anesthetic (e.g., bupivacaine)
Complications:
- Pneumothorax (~8-9% cumulative, ~1.4% per individual block)
- Intravascular injection (arterial or venous puncture)
- Parietal pleural puncture
3. Lateral Thoracotomy
Division of thoracic wall muscles causes significant postoperative pain; intercostal nerves (particularly lateral cutaneous branches) are at risk during thoracotomy incisions.
4. Breast Innervation
The nipple is innervated by the 4th intercostal nerve (T4). Innervation of the breast overall is via anterior and lateral cutaneous branches of T2-T6.
5. Intercostobrachial Nerve (T2)
Commonly divided during axillary lymph node dissection for breast cancer, resulting in numbness/dysesthesia of the axilla and medial arm. Surgeons attempt to preserve it when possible.
Sources:
- Gray's Anatomy for Students, pp. 193-197
- Morgan & Mikhail's Clinical Anesthesiology, 7e
- Tintinalli's Emergency Medicine, p. 287
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 228
This is a shared conversation. Sign in to Orris to start your own chat.