Epidemiology psm
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the core content needed. Let me compile the comprehensive answer.
Epidemiology PSM: Screening & Natural History of Disease
Source: Park's Textbook of Preventive and Social Medicine, 24th ed.
NATURAL HISTORY OF DISEASE
Natural history of disease refers to the course a disease takes in an individual from its earliest stage until its final outcome - without medical intervention. It is divided into two major phases:
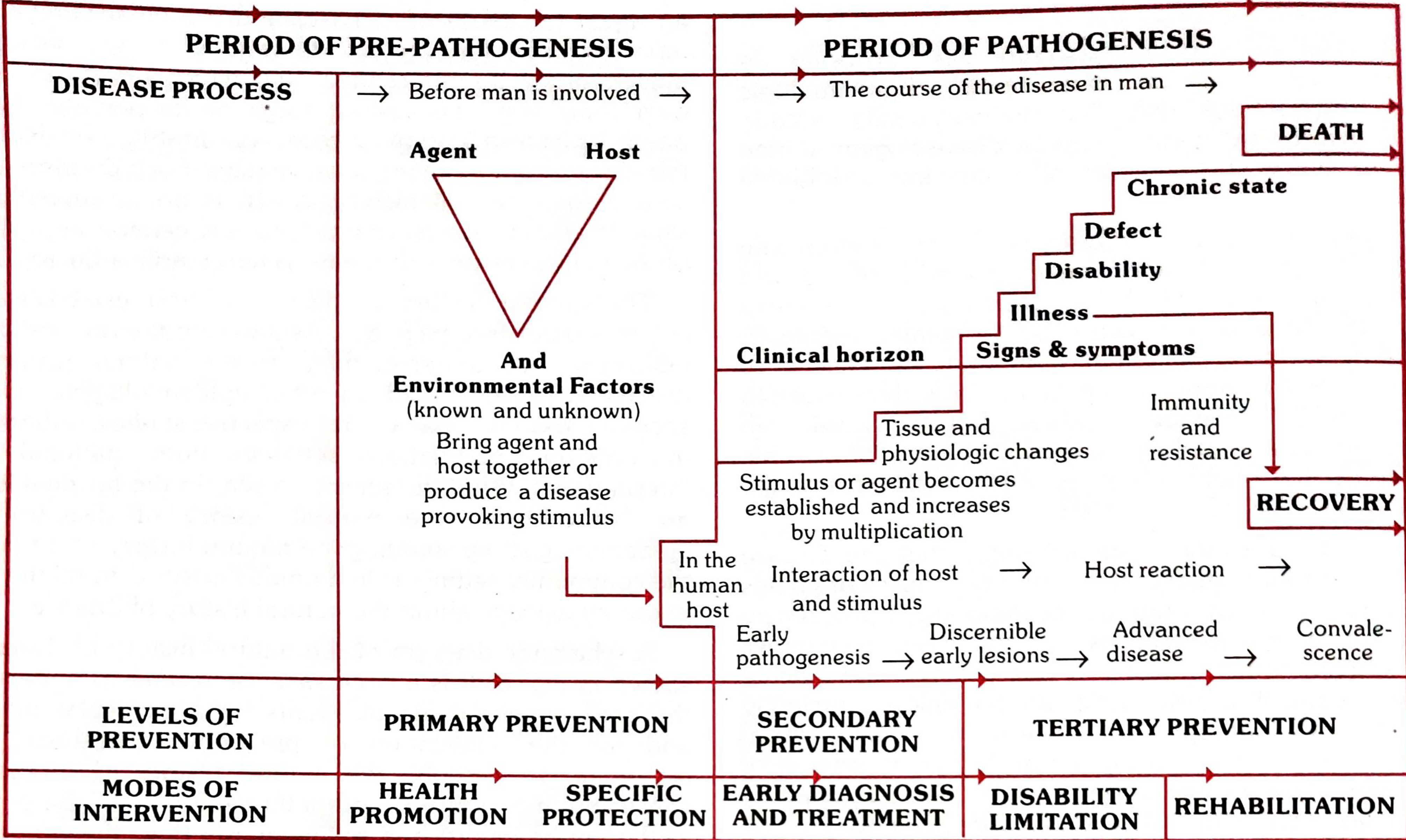
Phase 1: Pre-pathogenesis Phase
- Refers to the period before the disease agent enters the host
- The disease agent has not yet interacted with man, but favourable factors (Agent + Host + Environment) already exist
- This situation is called "man in the midst of disease" or "man exposed to risk"
- We are all, potentially, in the pre-pathogenesis phase of many diseases
- The three interacting factors form the Epidemiological Triad:
- Agent - biological, nutrient, chemical, physical, or social
- Host - age, sex, immunity, genetics, behaviour
- Environment - physical, biological, social
- Their interaction determines whether disease starts, and whether it becomes sporadic, endemic, or epidemic
Level of prevention: PRIMARY PREVENTION
Modes of intervention: Health Promotion + Specific Protection
Phase 2: Pathogenesis Phase
Begins when the disease agent enters the susceptible host.
In Infectious Diseases:
- Agent multiplies → tissue and physiological changes → incubation period → early pathogenesis → late pathogenesis
- Final outcome: Recovery, Disability, or Death
- Host response is not always predictable - infection may be clinical or subclinical, typical or atypical, or the host may become a carrier (e.g., diphtheria, Hepatitis B)
In Chronic Diseases (e.g., hypertension, CAD, cancer):
- Early pathogenesis is the presymptomatic phase - pathological changes are below the "clinical horizon" (not yet apparent clinically)
- Disease becomes clinically apparent only in the late pathogenesis phase when signs/symptoms appear, by which time the disease is already well advanced
Progression through pathogenesis phase (from the Leavell & Clark model):
| Stage | Description |
|---|---|
| Early pathogenesis | Agent established, tissue changes beginning |
| Discernible early lesions | Sub-clinical changes detectable by tests |
| Advanced disease | Clinical signs and symptoms appear (above clinical horizon) |
| Convalescence/Outcome | Recovery, Defect, Disability, Chronic state, or Death |
Level of prevention: SECONDARY PREVENTION (early detection) + TERTIARY PREVENTION (late disease)
Modes of intervention: Early Diagnosis & Treatment → Disability Limitation → Rehabilitation
CONCEPT OF LEAD TIME
Lead time is the time by which screening advances the diagnosis - the period between when a screening test detects the disease and when it would ordinarily have been diagnosed clinically.
- Only diseases with a significant time lag between biological onset and clinical appearance are worth screening
- Screening has no value in diseases whose onset is immediately obvious
- The goal is to intervene during the presymptomatic phase (below the clinical horizon) before irreversible damage occurs
SCREENING
Definition
"The search for unrecognized disease or defect by means of rapidly applied tests, examinations or other procedures in apparently healthy individuals."
Screening is a preventive care function - it is not diagnostic. Positive results are referred for formal diagnostic work-up.
Screening vs. Diagnostic Tests
| Feature | Screening Test | Diagnostic Test |
|---|---|---|
| Applied to | Apparently healthy | Sick / with indications |
| Scope | Groups | Individual patients |
| Accuracy | Less accurate | More accurate |
| Cost | Less expensive | More expensive |
| Result | Not final - needs confirmation | Basis for treatment |
| Initiative | From investigator / agency | From patient with complaint |
| Cut-off | Single criterion / cut-off point | Multiple symptoms, signs, labs |
Note: Some tests serve both purposes (e.g., GTT, anaemia test).
Types of Screening
| Type | Description |
|---|---|
| Mass screening | Applied to the entire population without selection |
| Selective (high-risk) screening | Targets a defined high-risk group (e.g., antenatal mothers, industrial workers) |
| Multiphasic screening | Two or more tests applied simultaneously to a large group at one time |
Multiphasic screening: RCT evidence from the UK and USA showed no benefit in mortality or morbidity reduction and increased healthcare costs without observable benefit. Its utility has therefore been questioned.
Uses of Screening
- Early detection and treatment of disease
- Epidemiological research - estimating prevalence, distribution
- Education of public and health professionals
- Completing the natural history of disease
CRITERIA FOR SCREENING (Wilson & Jungner Criteria)
Two sets of criteria must be satisfied before initiating a programme: criteria related to the disease and the test.
A. Criteria Related to the Disease
- The condition must be an important health problem (generally, high prevalence)
- There must be a recognizable latent or early asymptomatic stage
- The natural history must be adequately understood - including when the process becomes irreversible
- A test must exist that can detect disease before signs/symptoms appear
- Facilities for confirmation of diagnosis must be available
- There must be an effective treatment available
- There must be an agreed policy on whom to treat (e.g., borderline hypertension, pre-diabetes)
- Good evidence that early detection + treatment reduces morbidity and mortality
- Expected benefits must exceed risks and costs
B. Criteria Related to the Screening Test
The test must satisfy:
- Acceptability - must be acceptable to the target population; painful, embarrassing, or uncomfortable tests (e.g., rectal/vaginal exams) reduce compliance in mass campaigns
- Repeatability (Reliability/Precision) - consistent results on repeated application under same conditions
- Validity - ability to correctly identify those with and without disease, measured by:
- Sensitivity - ability to correctly identify true positives (TP / TP+FN × 100)
- Specificity - ability to correctly identify true negatives (TN / TN+FP × 100)
- Yield - amount of previously unrecognized disease detected
- Simplicity - can be administered by non-physicians
- Safety - minimal risk to the population
- Rapidity - results available quickly
- Low cost
Sensitivity & Specificity (2×2 Table)
| Disease Present | Disease Absent | |
|---|---|---|
| Test Positive | True Positive (TP) | False Positive (FP) |
| Test Negative | False Negative (FN) | True Negative (TN) |
- Sensitivity = TP / (TP + FN) × 100 → "Ability to detect disease when it IS present"
- Specificity = TN / (TN + FP) × 100 → "Ability to rule out disease when it is ABSENT"
- Positive Predictive Value (PPV) = TP / (TP + FP) × 100 → depends heavily on prevalence
- Negative Predictive Value (NPV) = TN / (TN + FN) × 100
Example from Park's (EEG for brain tumours):
- Sensitivity = 36/40 × 100 = 90%
- Specificity = 306,000/360,000 × 100 = 85%
Key rule: When sensitivity ↑, specificity tends to ↓ (trade-off determined by the cut-off point chosen). A lower cut-off → more sensitive but less specific. This is illustrated by the ROC (Receiver Operating Characteristic) curve.
Predictive Value and Prevalence
A critical concept: PPV is directly influenced by the prevalence of disease in the population screened.
- When prevalence is high → PPV is high (more true positives among positive tests)
- When prevalence is low → PPV falls dramatically (most positives will be false positives)
- This is why screening is more effective in high-risk populations rather than the general public for rare conditions
Summary: Where Screening Fits in Natural History
Pre-pathogenesis → Presymptomatic phase → Clinical horizon → Clinical disease
↑
[SCREENING WINDOW]
Lead time gained here
Secondary prevention
Screening targets the presymptomatic phase - after pathological changes have begun but before the clinical horizon is crossed. The goal is to detect disease here, where intervention can still alter the outcome.
Park's Textbook of Preventive and Social Medicine, 24th ed., Block 1 (Natural History, pp. 46-47) and Block 2 (Screening, pp. 155-162)
This is a shared conversation. Sign in to Orris to start your own chat.