colles fracture
Reading File
Finding Sources
Searching PubMed
"Colles fracture" AND treatment
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have rich content from multiple authoritative sources. Here is the comprehensive answer:
Colles' Fracture
Definition
A Colles' fracture is a transverse fracture of the distal radial metaphysis within 2-2.5 cm of the articular surface, characterized by dorsal angulation, dorsal and proximal displacement, and radial deviation of the distal fragment. It is the most common wrist fracture in adults.
- Pye's Surgical Handicraft, p. 189
- Rosen's Emergency Medicine, p. 611
Mechanism
- Fall on an outstretched, extended hand (FOOSH)
- Compression forces on the dorsal side produce dorsal comminution
- Most common in postmenopausal women (often a pathological fracture on an osteoporotic background)
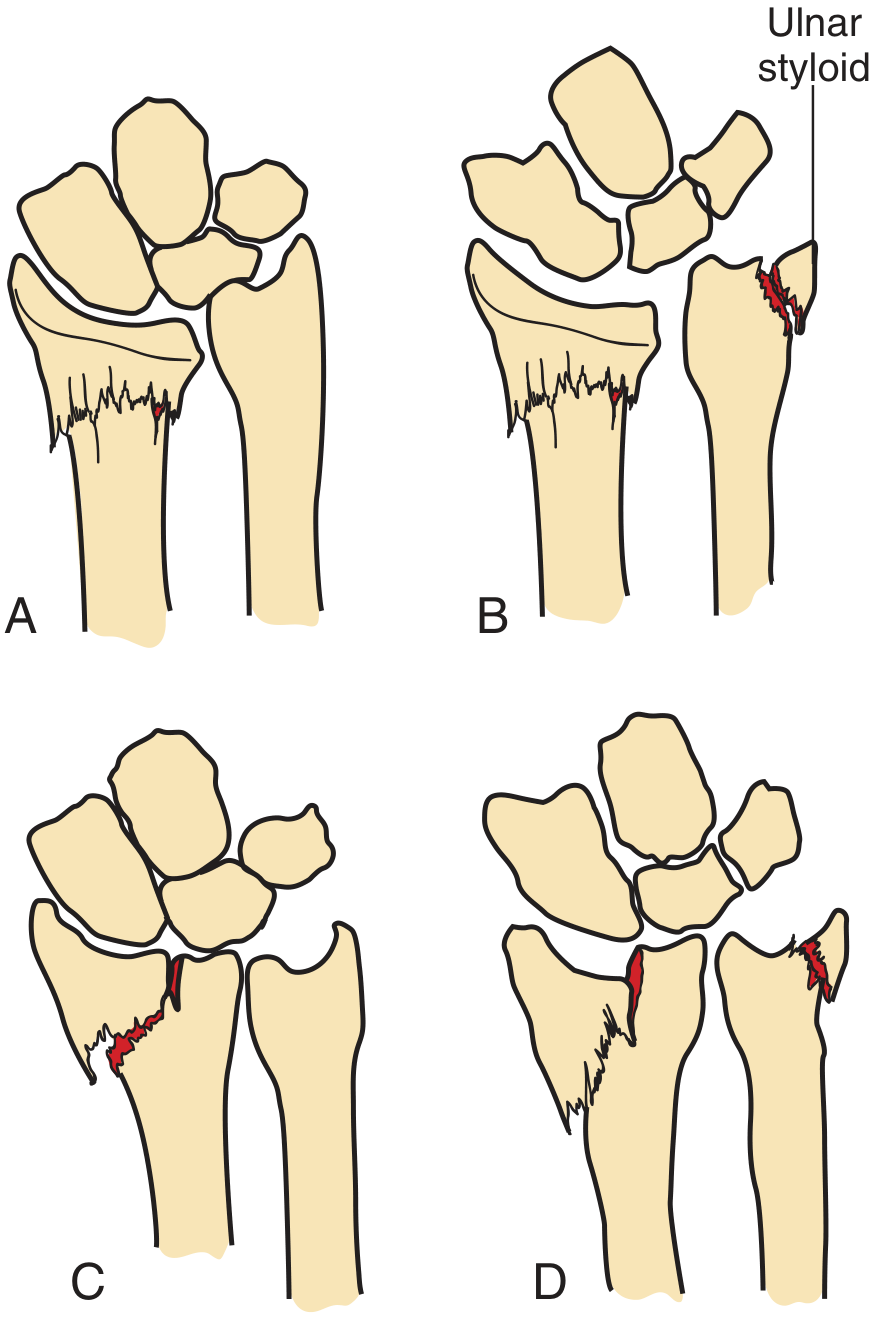
Radiographic Appearance
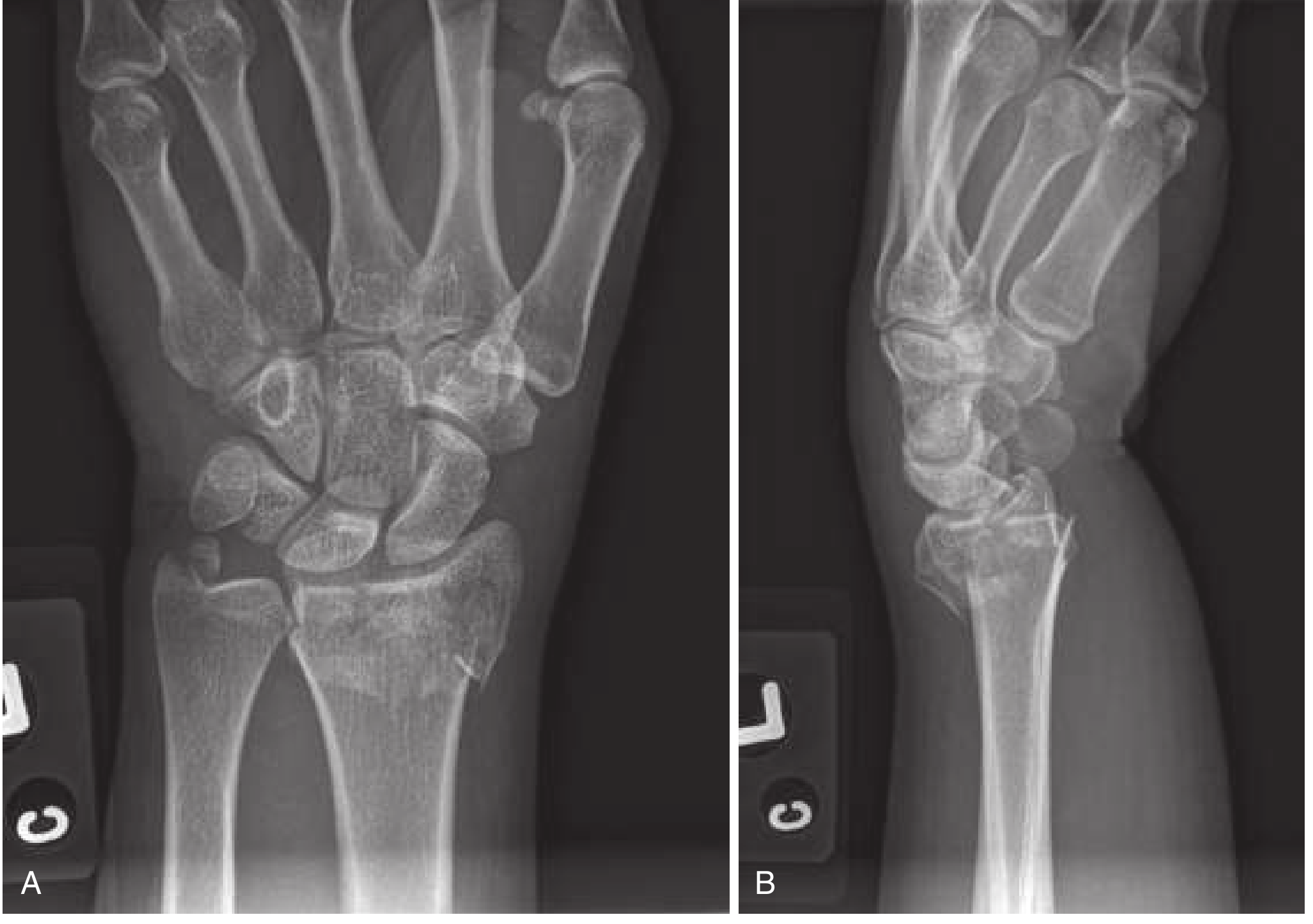
PA view findings:
- Distal metaphyseal radius fracture, often shortened
- Radial displacement of the carpus
- Ulnar styloid fracture (present in ~60% of cases)
- Intraarticular extension into radiocarpal or radioulnar joints possible
Lateral view findings (best for diagnosis):
- Dorsal angulation and displacement of radial fragment
- Loss of normal volar tilt of the distal radial articular surface
Clinical Features
| Feature | Detail |
|---|---|
| Deformity | "Dinner fork" (lateral view) |
| Swelling & tenderness | Over distal radius |
| Radial deviation | Lower end of ulna becomes prominent |
| Paresthesias | Palmar - median nerve compression |
Radiology: Criteria for Instability / Reduction
Reduction is indicated when:
- Dorsal angulation >20 degrees on lateral view
- Radial shortening - radius shorter than ulna on PA view (positive ulnar variance)
- Intraarticular involvement with step-off
- Marked comminution, or >1 cm shortening
The lateral view line test (Pye's): Draw a line between the anterior and posterior lips of the radial articular surface. If tilted backwards relative to the radial shaft or displaced radially, reduction is needed. If tilted slightly forwards or at right angles, reduction is likely unnecessary.
Management
Non-Operative (Stable Fractures)
- Extra-articular, non-displaced: double sugar-tong splint (one from elbow to wrist, second from elbow to axilla) for 3-5 days, then short-arm cast for 4-6 weeks
- Follow-up radiographs at 1, 2, and 6 weeks to ensure no displacement
Closed Reduction Technique
- Anesthesia: Hematoma block - inject 5-10 mL of 1% lidocaine (±bupivacaine) via 22-gauge needle into the dorsal fracture hematoma. Bier block (IV regional anesthesia) or regional nerve blocks (median, radial, ulnar, brachial plexus) are alternatives.
- Finger traps: Applied to relax deforming forces from muscle spasm; may achieve reduction alone and hold position during splinting.
- Traction: While the forearm is held firmly, push the fragment distally and palmarly.
- Goal: Restore volar tilt (at minimum, neutral/zero degrees), radial inclination, and proper radial length.
- Splint: Sugar-tong splint post-reduction. Avoid circumferential casting for ≥24 hours due to post-reduction edema.
- Post-reduction: Urgent orthopedic follow-up within 2-3 days.
Operative Indications
- Unstable fractures (>20° angulation, marked comminution, intraarticular)
- Fractures not amenable to or not maintained by closed reduction
- Open fractures
- Neurovascularly compromised fractures
- High-demand patients (dominant wrist, young/active)
CT scan is helpful when significant intraarticular extension, comminution, or distal radioulnar joint (DRUJ) instability is suspected.
Associated Injuries
- Ulnar styloid fracture (~60%) - may indicate triangular fibrocartilage complex (TFCC) injury and DRUJ disruption (a significant source of long-term morbidity)
- Carpal instability
- Median nerve injury (most common nerve, ~17%)
- TFCC tears
- Radiocarpal/radioulnar instability
Complications (occur in 6-80% of cases)
| Complication | Notes |
|---|---|
| Carpal tunnel syndrome | Most common; immediate or delayed; from nerve damage or swelling |
| Median nerve injury | ~17%; from contusion, traction, compression, or cast |
| Malunion | Especially with inadequate reduction |
| DRUJ instability | From TFCC injury / ulnar styloid fracture |
| Post-traumatic arthritis | Especially with intraarticular extension |
| Stiffness & weakness | Particularly in elderly |
| Reflex sympathetic dystrophy (CRPS) | Rare but debilitating |
| Iatrogenic | Extreme wrist flexion in splint can cause median nerve damage; thin skin may convert closed to open fracture |
Red flags for poor outcome: dorsal angulation ≥20°, radial shortening ≥5 mm.
Comparison with Related Fractures
| Fracture | Displacement | Deformity |
|---|---|---|
| Colles' | Dorsal | "Dinner fork" |
| Smith's (reverse Colles') | Volar | "Garden spade" |
| Barton's | Volar or dorsal articular fragment + carpal shift | Intraarticular |
Sources: Tintinalli's Emergency Medicine, p. 1847-1848 | Rosen's Emergency Medicine, p. 611-612 | Pfenninger & Fowler's Procedures for Primary Care, p. 1321 | Pye's Surgical Handicraft, p. 189
This is a shared conversation. Sign in to Orris to start your own chat.