Inj. Cefparzone for gi pt had vomiting pain in abdo with low grade fever
Inj. Cefoperazone (Cefoperazone-Sulbactam) - GI Patient with Vomiting, Abdominal Pain & Low-Grade Fever
Most Likely Cause: Disulfiram-Like Reaction
- Katzung's Basic and Clinical Pharmacology, 16th Ed: "Disulfiram-like reactions are noted with cefamandole, cefoperazone, cefotetan, and moxalactam."
- Nausea and vomiting (most prominent)
- Abdominal pain / cramping
- Flushing, headache, tachycardia
- Low-grade fever (from vasodilation and autonomic activation)
- In severe cases: hypotension, chest pain
Other Contributing Causes to Consider
| Cause | Explanation |
|---|---|
| Direct GI effects of Cefoperazone | Cephalosporins commonly cause nausea, vomiting, diarrhea as direct GI adverse effects |
| Altered gut flora / C. difficile colitis | Cefoperazone has high biliary excretion (~70-75%), leading to high gut concentrations and disruption of normal flora; C. difficile-associated diarrhea and colitis are a real risk |
| Biliary sludge | Cefoperazone is a known cause of biliary sludge and pseudolithiasis - can cause RUQ/abdominal pain |
| Underlying GI disease flare | Patient is already a "GI patient" - the drug may be irritating an existing condition |
Key Risk Factor to Ask About
- Alcohol-based hand sanitizer absorbed through skin (rare but described)
- Fermented foods
- Cough syrups with alcohol base
Management
- Stop alcohol exposure completely - counsel patient and family strictly
- Assess severity - check vitals, BP, HR, temperature
- Supportive care - IV fluids if vomiting is significant, antiemetics (ondansetron/metoclopramide)
- For fever - paracetamol (acetaminophen); note that paracetamol metabolism in alcoholics can produce hepatotoxic metabolites, so dose carefully
- Rule out C. difficile - if diarrhea accompanies symptoms, send stool for C. difficile toxin
- Check LFTs + INR - Cefoperazone's MTT side chain can also cause hypoprothrombinemia (inhibits Vitamin K-dependent clotting factor synthesis); monitor PT/INR especially in malnourished patients
- Vitamin K - consider prophylactic Vit K1 (phytonadione) if patient is malnourished or has prolonged course
Important Side Effects of Cefoperazone to Monitor
| Side Effect | Mechanism |
|---|---|
| Disulfiram-like reaction | MTT side chain inhibits ALDH |
| Hypoprothrombinemia / bleeding | MTT side chain inhibits Vit K-dependent clotting factors |
| Biliary sludge / pseudolithiasis | High biliary concentration |
| C. difficile colitis | Disruption of gut flora (high biliary excretion) |
| Hypersensitivity (rash, anaphylaxis) | Beta-lactam class effect |
| Diarrhea | Very common (up to 1 in 3 patients) |
Bottom Line
- Confirm/rule out alcohol exposure
- Supportive care
- Check INR (MTT-related hypoprothrombinemia risk)
- Rule out C. difficile if diarrhea is present
- Katzung's Basic and Clinical Pharmacology, 16th Ed, Drug Interactions Table
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Beta-Lactam Antibacterials section
Pt is not alcholic
Cefoperazone in a Non-Alcoholic GI Patient - Vomiting, Abdominal Pain, Low-Grade Fever
1. Clostridioides difficile Infection (CDI) - Most Important to Rule Out
- It is excreted predominantly via bile (~75%), creating very high concentrations in the colon
- This disrupts normal colonic flora more than renally-excreted antibiotics
- The patient is already a GI patient (likely hospitalized, with comorbidities) - all CDI risk factors
"Most patients develop watery diarrhea during antibiotic therapy or shortly after... Other symptoms of CDI include abdominal pain, fever, weakness, loss of appetite, nausea, and vomiting."
- Sabiston Textbook of Surgery
- Send stool for C. difficile toxin A/B (ELISA or PCR)
- If high clinical suspicion, do not wait for results - start treatment
- Vancomycin 125 mg PO QID x 10 days (first-line) OR Fidaxomicin 200 mg PO BD x 10 days
- Consider stopping Cefoperazone if clinically appropriate
2. Direct GI Adverse Effects of the Drug
- Nausea, vomiting, and abdominal cramping as direct GI effects
- Diarrhea (very common with broad-spectrum agents)
- This is a diagnosis of exclusion - rule out CDI first
3. Hypoprothrombinemia (MTT Side Chain Effect)
"Cephalosporins that contain a methylthiotetrazole group may cause hypoprothrombinemia and bleeding disorders... this group included cefamandole, cefmetazole, and cefoperazone."
-
Katzung's Basic & Clinical Pharmacology, 16th Ed
-
Risk is higher in malnourished patients, elderly, prolonged use
-
GI patients are often nutritionally depleted - making this a real concern
-
Check PT/INR now
-
Give Vitamin K1 (phytonadione) 10 mg orally twice weekly prophylactically, or IV if bleeding is present
4. Drug Fever (Hypersensitivity)
Immediate Action Plan
| Step | Action |
|---|---|
| 1 | Send stool for C. difficile toxin (PCR preferred) |
| 2 | Check CBC, LFTs, PT/INR, CRP |
| 3 | IV fluids + antiemetics (ondansetron) for symptom relief |
| 4 | Give Vitamin K1 if INR is elevated or patient is malnourished |
| 5 | If CDI confirmed - start oral vancomycin 125 mg QID x 10 days |
| 6 | Reassess whether Cefoperazone can be stopped or switched |
Key Point for This Patient
- Katzung's Basic and Clinical Pharmacology, 16th Ed - Cephalosporin Toxicity
- Sabiston Textbook of Surgery - Clostridioides difficile Colitis
Tell me diff diagnosis of this pt c/o vomiting after eating since 8 days loss of appetite no taste she on anti depressant medication also
Differential Diagnosis - Female on Antidepressants, Vomiting After Eating x 8 Days, Anorexia, Loss of Taste
MOST LIKELY DIAGNOSES
1. Antidepressant-Induced GI Side Effects ⭐ (FIRST TO CONSIDER)
- When first started or dose increased
- SSRIs (fluoxetine, sertraline, escitalopram) cause nausea/vomiting in up to 20-30% of patients by stimulating 5-HT3 receptors in the gut
- SNRIs (venlafaxine, duloxetine) cause nausea + dry mouth + loss of appetite
- TCAs can cause anticholinergic effects - delayed gastric emptying, bloating, constipation, nausea
"Higher incidence of nausea/vomiting, dry mouth, sexual side effects, and hypertension" with SNRIs - Bradley and Daroff's Neurology in Clinical Practice
2. Functional Dyspepsia / Postprandial Distress Syndrome
- Very common in patients with psychiatric comorbidity (depression, anxiety)
- Symptoms: postprandial fullness, early satiety, nausea, vomiting, anorexia
- Brain-gut axis dysregulation is the core mechanism - antidepressants actually both cause AND treat this
- Loss of taste (dysgeusia) and appetite suppression are characteristic
"Epigastric pain, postprandial fullness, early satiation, anorexia, belching, nausea and vomiting, upper abdominal bloating" - Sleisenger & Fordtran's GI and Liver Disease
3. Gastroparesis
- Delayed gastric emptying causing postprandial nausea and vomiting
- Nausea (92%), vomiting (84%), early satiety, anorexia are the hallmarks
- Can be:
- Idiopathic (most common)
- Diabetic (check blood sugar - patient may be on antidepressants for diabetic neuropathy)
- Post-infectious (viral gastroparesis - can present subacutely over days)
- Antidepressants (especially TCAs) can worsen gastroparesis via anticholinergic effects
"Nausea was present in 92%, vomiting in 84%, abdominal bloating in 75%, early satiety" in gastroparesis patients - Yamada's Textbook of Gastroenterology
4. H. pylori / Peptic Ulcer Disease / Gastritis
- H. pylori: nausea, anorexia, vomiting, epigastric pain
- Gastritis / PUD: postprandial nausea and vomiting, loss of appetite, epigastric discomfort
- Very common cause of subacute vomiting - always rule out
"Primary infection with H. pylori causes nausea and upper abdominal pain... findings of gastritis and PUD include nausea, anorexia, vomiting, epigastric pain" - Sherris & Ryan's Medical Microbiology
5. Depression Itself as a Cause (Somatic Symptoms)
- Depression directly causes anorexia, loss of taste/dysgeusia, nausea, and weight loss as somatic symptoms
- The patient is already on antidepressants - this suggests she has significant depression
- Inadequately controlled depression = persistent GI somatic symptoms
- This is a diagnosis of exclusion after organic causes are ruled out
6. Psychogenic / Anxiety-Related Vomiting
- Anxiety disorders frequently co-exist with depression (she is on antidepressants for likely both)
- Anticipatory vomiting triggered by eating (conditioned response)
- Loss of appetite and dysgeusia are prominent features
LESS COMMON BUT IMPORTANT TO RULE OUT
| Diagnosis | Key Feature |
|---|---|
| Pregnancy | Must rule out in women of childbearing age - urine βhCG first |
| Addison's Disease | Loss of taste (salt craving), nausea, anorexia, fatigue - can mimic depression |
| Hypothyroidism | Overlaps with depression; nausea, constipation, anorexia |
| Viral gastroenteritis | Usually resolves in <1 week; 8-day duration makes this less likely |
| Hepatitis (A, B, E) | Anorexia, nausea, vomiting, dysgeusia, low-grade fever |
| Early gastric malignancy | In older patients - anorexia + vomiting + weight loss = red flag |
| Pancreatitis / GERD | Postprandial nausea and vomiting |
Investigations to Order
| Test | Reason |
|---|---|
| Urine pregnancy test | First test in any female of childbearing age |
| H. pylori stool antigen / UBT | Rule out H. pylori |
| Upper GI endoscopy | If red flags (weight loss >8 days, age >40) |
| Blood glucose / HbA1c | Rule out diabetic gastroparesis |
| TFTs (TSH, T4) | Rule out hypothyroidism |
| LFTs, bilirubin | Rule out hepatitis |
| Gastric emptying scintigraphy | If gastroparesis suspected |
| Review antidepressant | Was it started/changed ~8 days ago? |
Clinical Bottom Line
"Was the antidepressant started or changed about 8 days ago?"
- Sleisenger & Fordtran's GI and Liver Disease - Functional Dyspepsia & Gastroparesis
- Yamada's Textbook of Gastroenterology - Gastroparesis, Clinical Presentation
- Bradley and Daroff's Neurology in Clinical Practice - Antidepressant Side Effects
Generate a diagnostic checklist/flowchart for postprandial vomiting
A clean clinical diagnostic flowchart for postprandial vomiting (vomiting after eating). The flowchart should be professional, medical style, on a white background with clear boxes, arrows, and color-coded branches. Start at the top with "POSTPRANDIAL VOMITING" as the title box. First branch: "Is patient female of childbearing age?" → YES → "Urine βhCG" → Positive → "Nausea/Vomiting of Pregnancy / Hyperemesis Gravidarum" (pink box). Negative → continue down. Second step: "Review Medications" box → "Started/changed drug in last 2 weeks?" → YES → List in a yellow box: "Drug-induced: SSRIs, SNRIs, TCAs, Metformin, Opioids, Antibiotics, Digoxin, NSAIDs" → "Adjust dose / switch drug / take with food". NO → continue. Third step: "Duration?" split into two branches: - LEFT: "Acute less than 1 week" → orange box → "Viral gastroenteritis / Food poisoning / Acute pancreatitis / Acute hepatitis / DKA / Appendicitis" - RIGHT: "Subacute / Chronic more than 1 week" → blue box → continue down Fourth step under Subacute/Chronic: "Associated Symptoms?" with 4 color-coded branches: 1. "Epigastric pain + bloating" → Green box → "H. pylori / Peptic Ulcer / Gastritis → Endoscopy + H. pylori test" 2. "Early satiety + fullness + bloating" → Purple box → "Gastroparesis → Gastric emptying scintigraphy" 3. "Heartburn + regurgitation" → Teal box → "GERD / Hiatus Hernia → Endoscopy / pH study" 4. "Anorexia + weight loss + no taste" → Red box → "Functional Dyspepsia / Depression / Malignancy → Endoscopy + psychiatric review" Fifth step: "Red Flag Symptoms?" box with checklist inside: weight loss >5kg, age >40, dysphagia, blood in vomit, night sweats, family history of cancer → "YES → URGENT Endoscopy + CT Abdomen" Bottom box: "Investigations Summary" table with two columns listing: All cases: Urine βhCG, blood glucose, TFTs, LFTs, FBC, CRP Targeted: H. pylori stool antigen, upper GI endoscopy, gastric emptying scan, abdominal ultrasound, CT abdomen Use color coding: pink for pregnancy, yellow for drugs, orange for acute, blue/purple for chronic, red for red flags. Clear Arial font, medical infographic style.
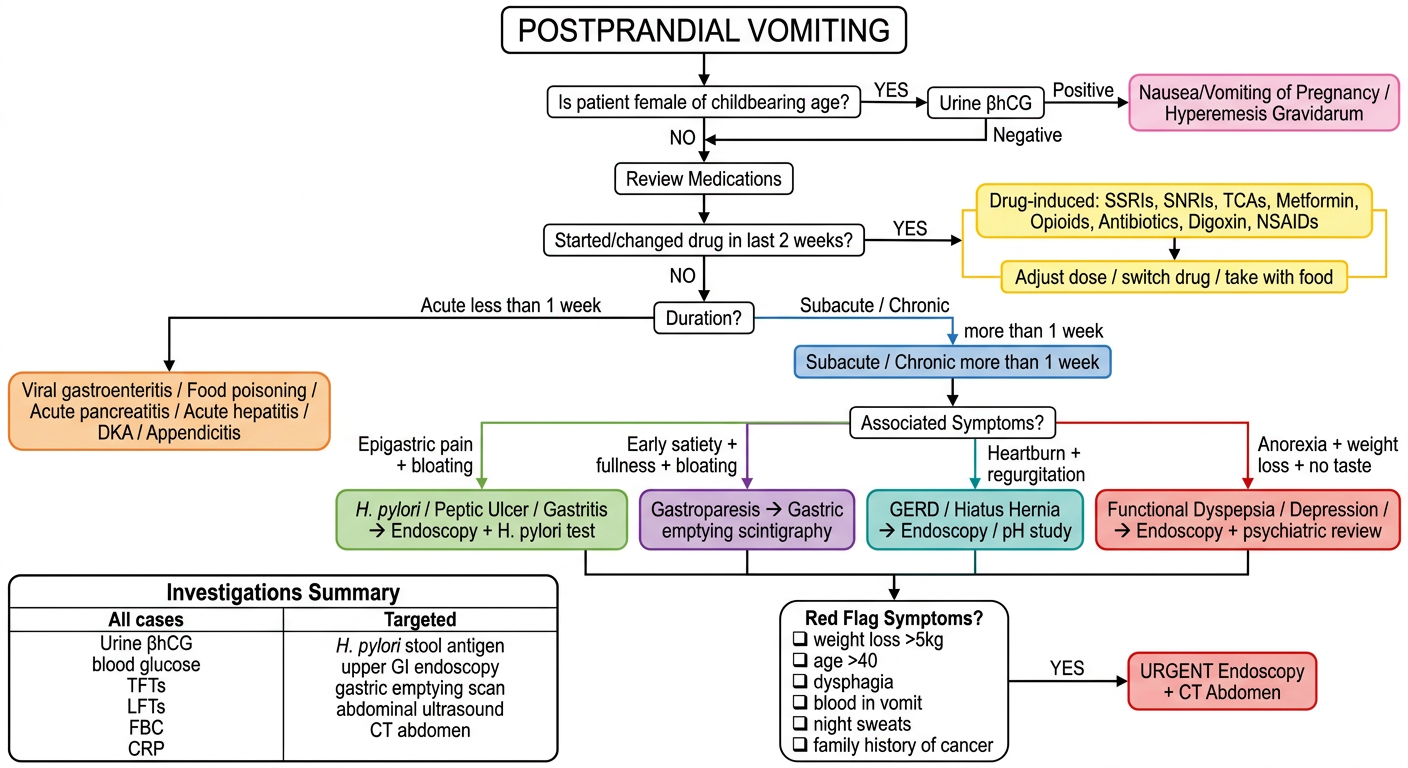
How to Use This Flowchart
- < 1 week (Acute): Think viral gastroenteritis, food poisoning, acute pancreatitis, acute hepatitis, DKA, appendicitis
- > 1 week (Subacute/Chronic): Follow the symptom branches below
| Dominant Symptom | Think | Test |
|---|---|---|
| Epigastric pain + bloating | H. pylori / PUD / Gastritis | Endoscopy + stool antigen |
| Early satiety + fullness | Gastroparesis | Gastric emptying scintigraphy |
| Heartburn + regurgitation | GERD / Hiatus hernia | Endoscopy / pH study |
| Anorexia + no taste + low mood | Functional dyspepsia / Depression / Malignancy | Endoscopy + psychiatric review |
- Weight loss > 5 kg
- Age > 40 with new symptoms
- Dysphagia
- Blood in vomit (haematemesis)
- Night sweats
- Family history of GI cancer