Version
I'm Orris, your AI assistant. Here's my current information:
- Version: Orris (powered by Claude Sonnet 4.5)
- Current date: Friday, June 26, 2026
- Current time: 11:10 AM
How can I help you today?
Define version
Version
A version is a specific form or variant of something, distinguished from earlier or later forms by changes, updates, or differences.
Common uses:
Software/Technology
A numbered release of a program or system that reflects updates, bug fixes, or new features (e.g., "version 2.0"). Higher numbers typically indicate newer iterations.
General meaning
A particular form of something that differs from other forms of the same thing - such as a translated version of a book, a director's cut of a film, or a revised edition of a document.
Versioning systems typically use formats like:
Major.Minor.Patch(e.g., 3.1.4) - where major = breaking changes, minor = new features, patch = small fixes- Date-based (e.g., 2026.06) - used by some software to indicate release date
- Named releases (e.g., "Orion", "Bionic Beaver")
Etymology
From Latin versio ("a turning"), from vertere ("to turn") - the idea of something being "turned" or transformed into a new form.
Version in obg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Version in Obstetrics & Gynecology
Version is a obstetric procedure in which the fetus is manually turned from a malpresentation (breech or transverse lie) into a more favorable presentation - almost always cephalic (vertex/head-down) - to facilitate vaginal delivery or reduce the need for cesarean section.
There are two main types:
1. External Cephalic Version (ECV)
The most commonly performed type. The fetus is manipulated entirely from outside through the maternal abdomen.
Timing
Performed at 36 weeks' gestation (not before, to avoid preterm birth; not too late, to maximize success before engagement).
Success Rate
Approximately 65% at 36 weeks. Success rate for transverse lie approaches 90%.
Technique
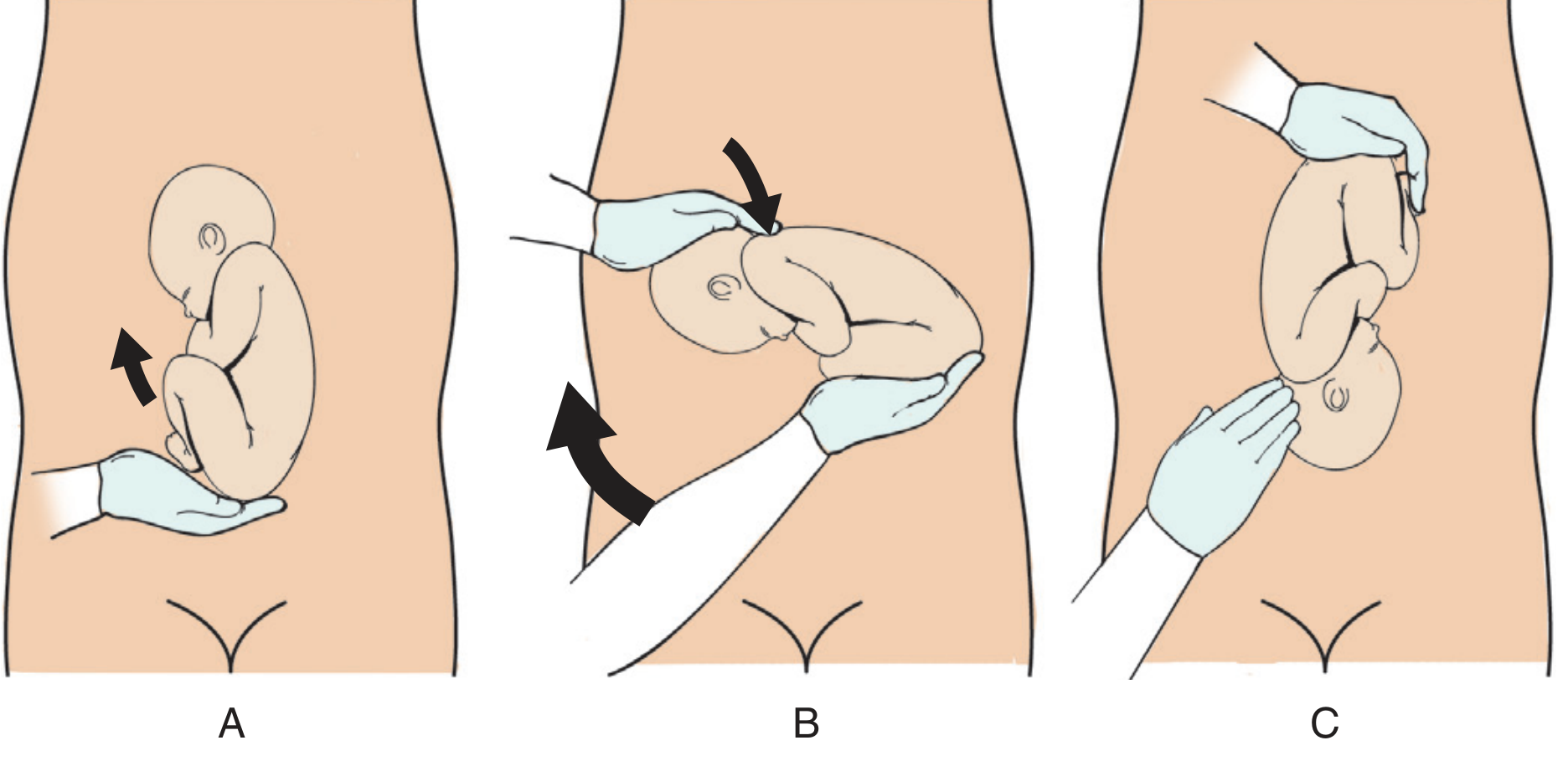
Figure: External cephalic version using the classic forward roll. A: Breech is mobilized. B & C: Breech pushed upward while the head is directed into the pelvis.
- Confirm breech presentation by real-time ultrasound; rule out oligohydramnios, multiple gestation, fetal anomalies
- Perform a reactive non-stress test (NST)
- Administer a tocolytic (terbutaline 0.25 mg SC) to relax the uterus
- Apply mineral oil to the abdomen to facilitate hand movement
- One operator elevates/displaces the breech; a second guides the head in the opposite direction
- Attempt a forward roll first; if unsuccessful, try a backward roll
- Monitor fetal heart rate with Doppler throughout; continue external monitoring for 1 hour post-procedure
- Administer RhoGAM to Rh-negative mothers
Note: A common error is attempting to turn the fetus before mobilizing the breech out of the pelvis.
Pre-procedure Equipment Needed
- Fetal heart rate monitor
- Ultrasound machine
- Examination table (Trendelenburg capable)
- Tocolytic agent
- RhoGAM (for Rh-negative patients)
2. Internal Podalic Version (IPV)
The operator inserts a hand into the uterus, grasps one or both fetal feet, and turns the fetus to a breech presentation for delivery. This is now rarely performed and mainly reserved for:
- Delivery of a non-vertex second twin
- Certain emergency situations
Factors Predicting Success vs. Failure
| Favorable (Success) | Unfavorable (Failure) |
|---|---|
| Multiparity (most consistent) | Engaged presenting part* |
| Adequate amniotic fluid (higher AFI = higher success) | Difficulty palpating fetal head* |
| Transverse lie (up to 90% success) | Uterus tense to palpation* |
| Unengaged fetal part | Maternal obesity |
| Earlier gestational age at attempt | Anterior placenta |
| Cervical dilation | |
| Decreased AFI |
*If all three asterisked factors are present, success rate is essentially 0%. If none are present, success exceeds 90%.
Contraindications to ECV
- Uterine anomalies
- Third-trimester bleeding
- Multiple gestation
- Oligohydramnios
- Evidence of uteroplacental insufficiency
- Nuchal cord identified on ultrasound
- Previous cesarean delivery or significant uterine surgery
- Obvious cephalopelvic disproportion (CPD)
Outcomes & Complications
- ECV reduces the risk of cesarean delivery by ~50% in patients with breech presentation at 36 weeks
- Serious complications (placental separation, cord compression requiring immediate delivery) occur in 1-2%
- Transient fetal bradycardia occurs in ~20% of attempts but almost always resolves when manipulation ceases
- Spontaneous reversion to breech after successful ECV: ~7%
- Even after successful ECV, patients have higher rates of instrumental and emergency cesarean delivery compared to primary vertex presentations
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Pfenninger and Fowler's Procedures for Primary Care, Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.