Anti hiv drugs pharmacology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Goodman & Gilman. Let me compile the full pharmacology answer:
Anti-HIV Drugs: Pharmacology
Overview
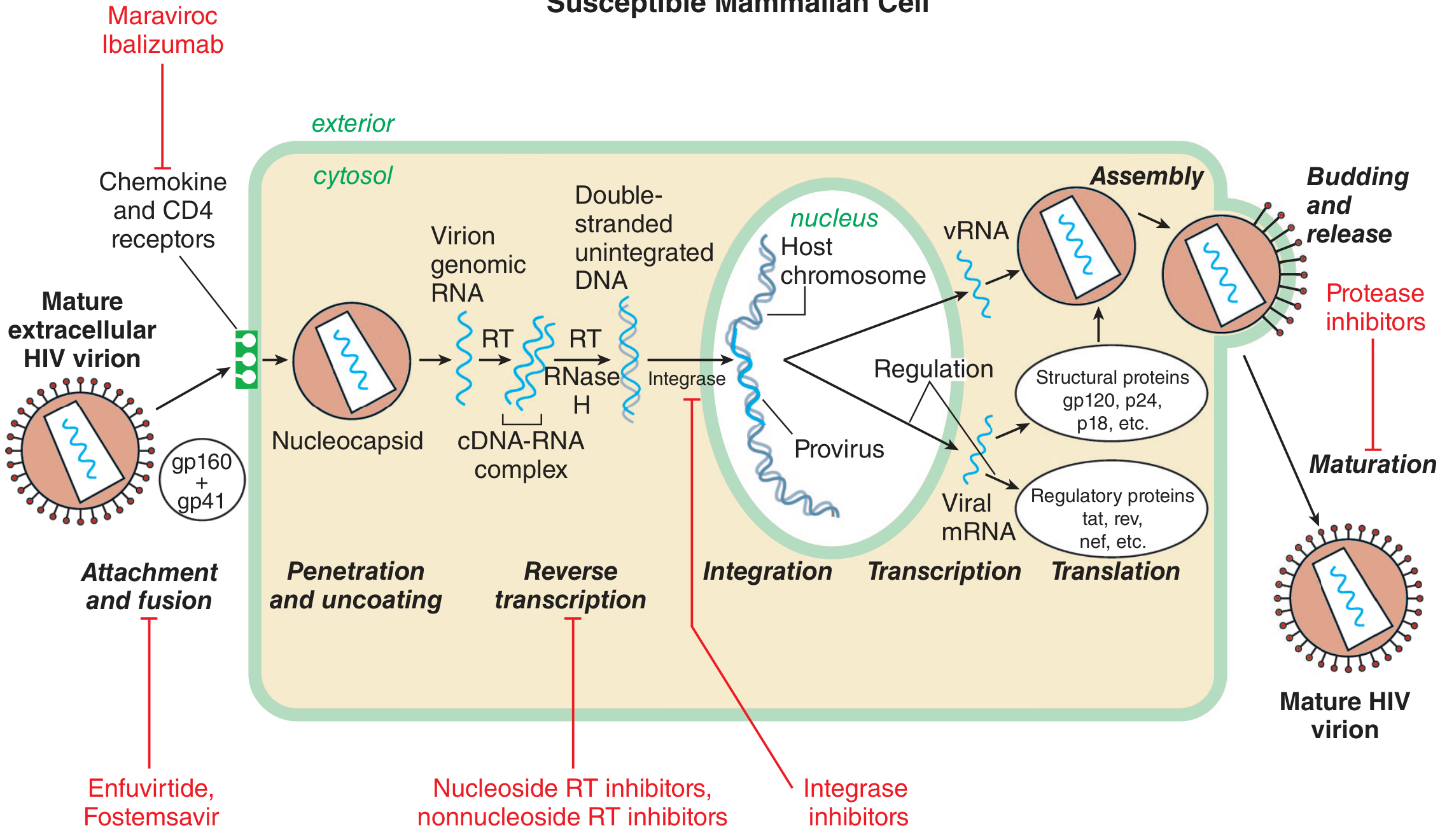
HIV is a lentivirus (retrovirus) with a 9,300 base-pair RNA genome. Its life cycle involves attachment, fusion, reverse transcription, integration, transcription, translation, assembly, budding, and maturation - each step a potential drug target. More than 30 approved antiretroviral drugs exist, and treatment requires lifelong combination therapy (typically 2-3 drugs simultaneously) to suppress viral replication and prevent resistance. The goal is an undetectable viral load (<50 copies/mL) within 24 weeks of starting therapy.
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 64
Drug Classes
1. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs / NtRTIs)
Mechanism: HIV reverse transcriptase converts viral RNA into proviral DNA. NRTIs are prodrugs - they are phosphorylated by host cell enzymes to their active triphosphate forms, which then competitively inhibit reverse transcriptase and cause chain termination (they lack a 3'-hydroxyl group needed for chain elongation). They act on newly infecting cells; they do NOT eradicate virus from cells already harboring integrated proviral DNA.
Drugs:
| Drug | Key Points |
|---|---|
| Zidovudine (AZT) | First antiretroviral; thymidine analogue; bone marrow toxicity (anemia, granulocytopenia), myopathy, lactic acidosis |
| Lamivudine (3TC) | Very well tolerated; also active against HBV; rapid high-level resistance with monotherapy |
| Emtricitabine (FTC) | Similar to lamivudine; long intracellular half-life (39 h); also anti-HBV |
| Tenofovir DF (TDF) | Nucleotide (already has one phosphate); also anti-HBV and anti-herpesvirus; nephrotoxicity risk |
| Tenofovir AF (TAF) | Prodrug of tenofovir; lower plasma levels = less renal/bone toxicity than TDF |
| Stavudine (d4T) | Thymidine analogue; significant mitochondrial toxicity, peripheral neuropathy, lipodystrophy |
| Didanosine (ddI) | High risk of pancreatitis, peripheral neuropathy; largely obsolete |
| Abacavir (ABC) | Requires HLA-B*5701 screening; hypersensitivity reaction (potentially fatal if rechallenged) |
Toxicity class effect: Older NRTIs (AZT, d4T, ddI) inhibit mitochondrial DNA polymerase gamma → mitochondrial toxicity (lactic acidosis, hepatic steatosis, lipodystrophy, myopathy, peripheral neuropathy). Newer NRTIs (emtricitabine, lamivudine, tenofovir) have minimal mitochondrial affinity and better tolerability.
PK: Not major CYP substrates; dosed once or twice daily. Intracellular active metabolites are eliminated more slowly than plasma parent drug.
2. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
Mechanism: Bind directly to a hydrophobic pocket on reverse transcriptase (distinct from the substrate binding site), causing allosteric inhibition. They do NOT require phosphorylation. Active only against HIV-1 (no activity against HIV-2). A single point mutation can confer high-level resistance rapidly.
Drugs:
| Drug | Key Points |
|---|---|
| Nevirapine | First NNRTI; induces CYP3A4 (drug interactions); serious rash/Stevens-Johnson syndrome, hepatotoxicity (especially in women with CD4 >250 and men >400) |
| Efavirenz | Most widely used historically; CNS effects (vivid dreams, dizziness, dysphoria) in up to 53%; once-daily; teratogenic in primates; moderate CYP3A4 inducer/weak inhibitor; t1/2 allows once-daily dosing |
| Rilpivirine | Better CNS tolerability than efavirenz; must be taken with food; not for high viral load (>100,000 copies/mL) or low CD4 <200 |
| Doravirine | Newest; fewer drug interactions; no food effect; good CNS profile |
| Etravirine | Active against many efavirenz-resistant strains; used in treatment-experienced patients |
3. HIV Protease Inhibitors (PIs)
Mechanism: Competitively inhibit HIV aspartyl protease, a homodimer that cleaves Gag and Gag-Pol polyproteins to produce mature, functional viral proteins. Without protease, virions are non-infectious (immature). They act at the budding/maturation step (post-integration), so they can also reduce virus production from already-infected cells.
Pharmacokinetic "Boosting": All PIs are CYP3A4 substrates. Ritonavir (at low dose 100-200 mg) or cobicistat (150 mg) is co-administered as a pharmacokinetic booster - they potently inhibit CYP3A4, increasing the AUC and t1/2 of co-administered PIs, allowing reduced doses and once-daily administration.
- Cobicistat is a ritonavir analogue with NO antiretroviral activity, used purely as a PK enhancer. It blocks tubular creatinine secretion, causing a small reversible rise in serum creatinine (not true nephrotoxicity).
Drugs:
| Drug | Key Points |
|---|---|
| Ritonavir | Rarely used therapeutically now; used as booster; potent CYP3A4 inhibitor; GI intolerance, hyperlipidemia |
| Lopinavir/r | Co-formulated with ritonavir; GI side effects; high lipid effects |
| Atazanavir/r | Once daily; unique side effect - indirect hyperbilirubinemia/jaundice (inhibits UGT1A1); requires acidic pH for absorption (avoid PPIs) |
| Darunavir/r | Currently preferred PI; once daily; active against many resistant strains; sulfonamide allergy caution |
| Fosamprenavir | Prodrug of amprenavir |
| Saquinavir | First PI approved |
| Indinavir | Nephrolithiasis (requires high fluid intake); largely obsolete |
| Nelfinavir | Only PI metabolized primarily by CYP2C19 (major metabolite then cleared by CYP3A4) |
Class toxicities: Metabolic syndrome - dyslipidemia (raised triglycerides, LDL), insulin resistance/diabetes, lipodystrophy, cardiovascular risk. These are less pronounced with newer boosted PIs.
4. Integrase Strand Transfer Inhibitors (InSTIs / INSTIs)
Mechanism: Inhibit the catalytic activity of HIV integrase. Integrase inserts viral double-stranded DNA into the host chromosome via a "strand transfer" reaction. InSTIs chelate the Mg²⁺ ion in the integrase active site and block this step. They are now the preferred class for initial therapy due to high efficacy, tolerability, and high barrier to resistance (especially dolutegravir and bictegravir).
Drugs:
| Drug | Key Points |
|---|---|
| Raltegravir | First InSTI; twice-daily dosing; metabolized by UGT1A1 (not CYP); chelated by Mg²⁺/Al³⁺ antacids (take 6h apart); myopathy, rhabdomyolysis reported |
| Elvitegravir | Requires cobicistat boosting; available only in fixed-dose combinations (Stribild, Genvoya); CYP3A4-metabolized; cross-resistance with raltegravir |
| Dolutegravir | Preferred first-line agent; twice-daily unboosted; high barrier to resistance; inhibits tubular creatinine secretion (raise serum Cr without true renal injury); neural tube defect risk periconceptionally (use with caution in women planning pregnancy) |
| Bictegravir | Available only in Biktarvy (BIC/FTC/TAF); once-daily; high barrier to resistance; no known clinically relevant resistance |
| Cabotegravir | Also available as long-acting injectable (with rilpivirine) for monthly/every-2-month dosing |
5. Entry Inhibitors
a. Fusion Inhibitors
- Enfuvirtide (T-20): Synthetic 36-amino-acid peptide that mimics the HR2 region of gp41, blocking the conformational change required for viral-cell membrane fusion. Only available as subcutaneous injection (twice daily). Injection site reactions are universal. Used only in treatment-experienced patients.
- Fostemsavir: Prodrug of temsavir; attachment inhibitor that binds directly to gp120, blocking attachment to CD4+ T cells. For multidrug-resistant HIV. QTc prolongation risk at high doses.
b. Co-receptor Antagonists (CCR5 Antagonists)
- Maraviroc: Blocks CCR5 chemokine co-receptor, preventing gp120 binding. Active only against CCR5-tropic virus. Requires tropism testing before use - no activity against CXCR4-tropic or dual-tropic virus. Hepatotoxicity risk; many drug interactions (CYP3A4 substrate).
c. Post-Attachment Inhibitors
- Ibalizumab: Humanized monoclonal antibody binding CD4 domain 2, causing steric hindrance of gp120-CD4 conformational change needed for fusion (but does not block gp120 attachment). Given IV every 2 weeks. Reserved for multidrug-resistant HIV in heavily treatment-experienced adults.
First-Line Preferred Regimens (Current Standard)
The current standard of care is to start treatment in ALL HIV-infected individuals regardless of CD4 count. Preferred initial regimens typically combine:
- 2 NRTIs + 1 InSTI (most common backbone)
- Examples: BIC/FTC/TAF (Biktarvy), DTG/ABC/3TC (Triumeq), DTG + FTC/TDF
- Two-drug regimens (e.g., dolutegravir + lamivudine) are also increasingly used as initial therapy
Resistance
- NRTIs: High-level resistance develops slowly (except lamivudine/emtricitabine - rapid single mutation K65R or M184V). Thymidine analogue mutations (TAMs) accumulate over time.
- NNRTIs: Single point mutation confers high-level class resistance (e.g., K103N for efavirenz/nevirapine).
- PIs: Multiple mutations required for high-level resistance; boosted PIs have a higher barrier.
- InSTIs: Raltegravir and elvitegravir have lower barriers; dolutegravir and bictegravir have very high barriers (multiple mutations needed).
Key Drug Interactions Summary
| Interaction | Mechanism | Examples |
|---|---|---|
| Rifampin reduces PI/NNRTI levels | CYP3A4 induction | Avoid rifampin with most PIs; prefer rifabutin |
| Ritonavir/cobicistat increase PI levels | CYP3A4 inhibition | Beneficial "boosting" |
| Antacids reduce InSTI absorption | Chelation of Mg²⁺ | Space by 6h for raltegravir |
| Atazanavir requires acid for absorption | Reduced dissolution at pH > 4 | Avoid PPIs |
| Dolutegravir/bictegravir inhibit OCT2 | Tubular creatinine transport | Apparent rise in serum creatinine (not nephrotoxicity) |
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 64 - Antiretroviral Agents and Treatment of HIV Infection
This is a shared conversation. Sign in to Orris to start your own chat.