Phacoemulsifi tion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of phacoemulsification based on Kanski's Clinical Ophthalmology (10th ed.).
Phacoemulsification
Overview
Phacoemulsification ('phaco') is the standard method of cataract extraction in high-income countries and in regional centres in most lower-income countries. It involves using a hollow titanium needle vibrating at ultrasonic frequency to emulsify the lens nucleus, which is then aspirated out of the eye through a small self-sealing corneal incision, after which a foldable intraocular lens (IOL) is inserted.
Phacodynamics - Key Parameters
Understanding machine settings is central to safe surgery:
| Parameter | Definition | Clinical Implication |
|---|---|---|
| Irrigating bottle height | Set above patient's eye | Maintains AC stability and IOP |
| Aspiration flow rate (AFR) | Volume of fluid removed (mL/min) | High AFR = faster lens removal but more surge risk; low settings safer for trainees |
| Vacuum (mmHg) | Generated during tip occlusion | Determines grip on lens fragments; high vacuum = less total power needed |
| Post-occlusion surge | Sudden outflow after tip occlusion breaks | Can cause capsular rupture; suppressed by modern machines |
Pump Types
- Peristaltic (flow) pump - Compresses tubing over rollers. Vacuum only builds at occlusion, then stops at set maximum. More predictable for trainees.
- Venturi (vacuum) pump - Uses compressed gas, vacuum and AFR are synchronized. Foot pedal depression directly increases vacuum independent of occlusion - always ready.
- Hybrid pumps - Offered by some modern machines, combining features of both.
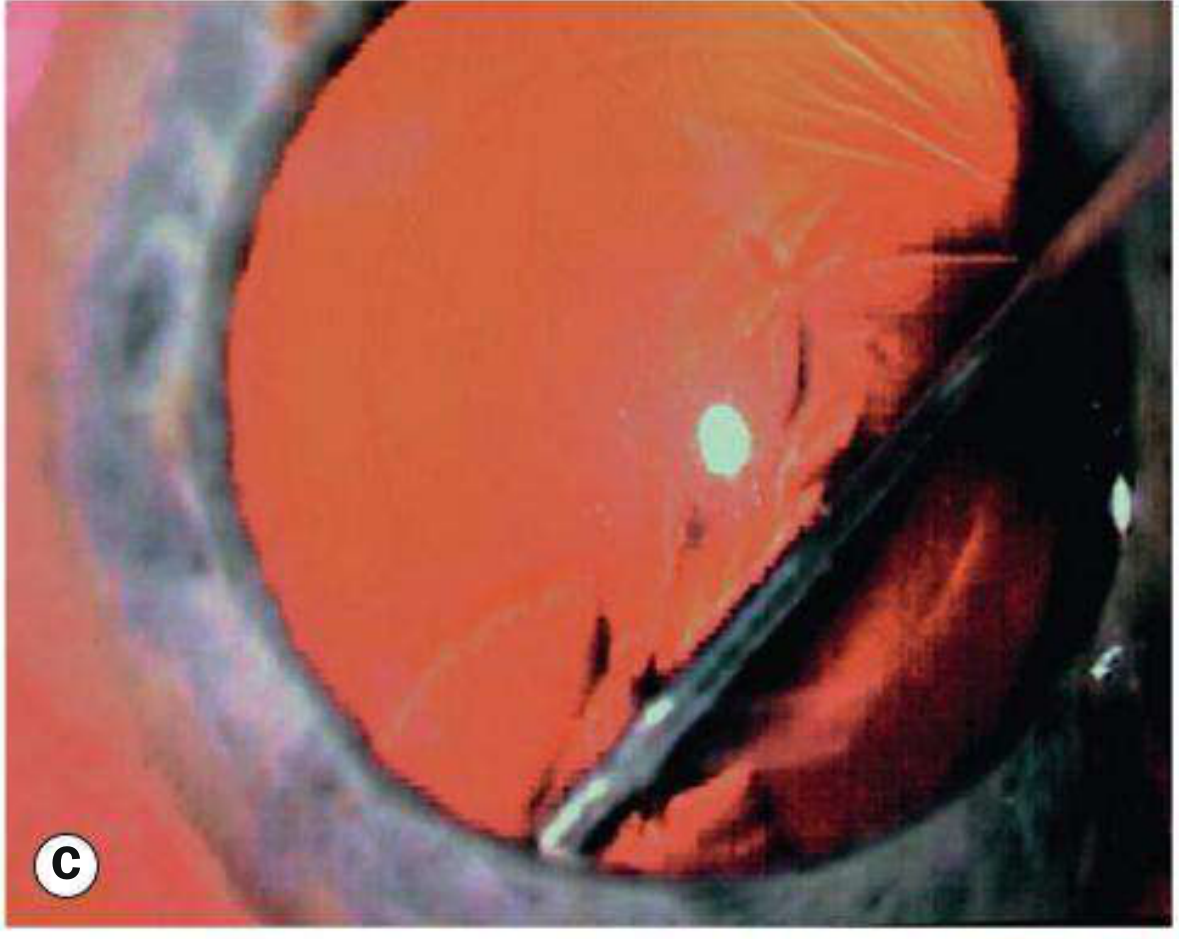
The Phaco Handpiece
The handpiece tip is a hollow titanium needle enclosed in a fluid-cooling sleeve (see image B above - capsulorhexis in progress with instruments in position). The emulsifying action is mediated by very high-frequency (ultrasonic) vibration producing:
- Jackhammer effect
- Cavitation
- Other mechanical effects
Variants include torsional phaco (less endothelial damage than longitudinal) and water jet-mediated systems. Tips differ in shape and size with different cutting/holding characteristics.
Ophthalmic Viscosurgical Devices (OVDs)
OVDs (viscoelastics) are bio-polymers critical to modern phaco surgery:
| Type | Properties | Uses |
|---|---|---|
| Cohesive (e.g., Healon) | High viscosity; easily removed | Maintain space, push iris back in small pupil |
| Dispersive (e.g., Viscoat) | Coats surfaces; harder to remove | Protect corneal endothelium, plug posterior capsular tears |
| Adaptive | Mixed characteristics | Versatile; some dilate and maintain pupil |
'Soft shell' technique: Inject outer dispersive layer + inner cohesive nucleus before capsulotomy - used routinely or in high-risk eyes (e.g., cornea guttata).
Surgical Technique - Step by Step
1. Preparation
- Topical anaesthetic applied
- Povidone-iodine 5% (or chlorhexidine) instilled into conjunctival sac; leave for minimum 3 minutes
- Eyelids cleaned, careful draping to exclude lashes and lid margins, speculum placed
2. Corneal Incision
- A small, self-sealing, clear corneal incision is made (typically 2.2-2.8 mm)
- Side-port incision made for the second instrument
3. Capsulorhexis
- Continuous curvilinear capsulorhexis (CCC) created in the anterior capsule
- Trypan blue stains the anterior capsule in dense cataracts with poor red reflex
- If rhexis starts running peripherally, inject cohesive OVD to flatten capsule and redirect centrally
4. Hydrodissection
- Balanced salt solution (BSS) injected under the anterior capsule to free cortical attachments
- Creates a fluid wave that separates cortex from capsule
5. Nucleus Emulsification
The nucleus is cracked and emulsified. Common techniques include:
- Divide and conquer - nucleus cracked into 4 quadrants, each emulsified
- Phaco chop - a chopper instrument is used to split the nucleus
- Nuclear hardness (brunescence) dictates power needed; black/dense nuclei require significantly more energy
6. Cortical Aspiration
- Residual cortex aspirated using bimanual automated technique or Simcoe cannula
- Meticulous removal prevents posterior capsular opacification (PCO)
7. IOL Implantation
- Capsular bag filled with OVD
- Foldable IOL injected through the small incision and positioned in the capsular bag
- OVD thoroughly removed
Complications
Intraoperative
- Posterior capsular rupture (PCR) - Most feared. Manifests as sudden change in AC depth and momentary pupil dilatation.
- Management: inject dispersive OVD, consider conversion to ECCE, use vitrector if vitreous prolapse
- Post-occlusion surge - Capsular rupture risk; minimized by machine settings
- Corneal endothelial damage - More with dense nuclei requiring high energy; torsional phaco reduces risk vs. longitudinal phaco
Postoperative
- Corneal decompensation - From dense nucleus requiring high phaco energy, or pre-existing corneal disease (e.g., Fuchs endothelial dystrophy; triple procedure considered: phaco + DSAEK/DMEK)
- Retinal detachment - Uncommon after uncomplicated phaco; risk factors include lattice degeneration, retinal breaks, high myopia, intraoperative vitreous loss
- Posterior capsular opacification (PCO) - Commonest late complication; treated with Nd:YAG laser capsulotomy
- Endophthalmitis - Prevented by intracameral antibiotic at end of surgery
Comparison: Phaco vs. MSICS vs. ECCE
| Feature | Phaco | MSICS | ECCE |
|---|---|---|---|
| Incision size | 2.2-2.8 mm (corneal) | ~6 mm (sclero-corneal tunnel) | 8-10 mm (limbal) |
| Closure | Self-sealing | Self-sealing | Sutures required |
| Technology | Expensive | Minimal | Minimal |
| Astigmatism | Least | Low | Higher |
| Setting | High-income, any | High-volume/low-income | Older technique |
| Visual rehab | Excellent | Comparable to phaco | Good |
Femtosecond Laser-Assisted Cataract Surgery (FLACS)
Femtosecond lasers (used in refractive surgery for years) have been adopted to replace several manual steps of phaco with automated processes - including the corneal incision, capsulorhexis, and initial nucleus fragmentation. This reduces ultrasound energy needed but adds cost and has not been shown to produce superior visual outcomes in uncomplicated cases.
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, pp. 321-340
This is a shared conversation. Sign in to Orris to start your own chat.