COVID 19 2nd yr mbbs microbiology refer apurba sastri cover definiTION DIAGRAM OF VIRUS clinical manifestation virulence factor,pathogenesis symptoms suppurative complications, non suppurative complications, lab diagnosis treatment answer in details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Note: Apurba Sastri's microbiology textbook is not available in this digital library. The following answer is compiled from three authoritative microbiology and medical textbooks - Jawetz, Melnick & Adelberg's Medical Microbiology 28e, Medical Microbiology 9e, Robbins Basic Pathology, and Harrison's Principles of Internal Medicine 22e (2025) - which cover all the same topics as Apurba Sastri with comparable or greater depth.
COVID-19 (Coronavirus Disease 2019)
A Complete 2nd Year MBBS Microbiology Guide
1. DEFINITION
COVID-19 is an infectious disease caused by SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2), a strain responsible for the first great pandemic of the 21st century. It is predominantly a respiratory illness that ranges from asymptomatic infection to severe, progressive pneumonia and multi-organ failure.
- The name "COVID" = COronaVIrus Disease, 19 = year 2019 (first identified)
- Causative agent: SARS-CoV-2, a Betacoronavirus
- The disease was declared a global pandemic by WHO on March 11, 2020
2. THE VIRUS - CLASSIFICATION & PROPERTIES
Classification
- Order: Nidovirales
- Family: Coronaviridae
- Subfamily: Coronavirinae
- Genus: Betacoronavirus
- Species: SARS-CoV-2
There are six coronaviruses that infect humans:
- Alpha-coronaviruses: 229E, NL63 (mild cold-like illness)
- Beta-coronaviruses: OC43, HKU1, SARS-CoV, MERS-CoV (and now SARS-CoV-2)
Important Properties (Table Format)
| Property | Description |
|---|---|
| Morphology | Spherical/pleomorphic, 80-160 nm diameter |
| Nucleocapsid | Helical symmetry |
| Genome | Single-stranded, positive-sense RNA (+ssRNA), linear, 27-32 kb |
| Genome features | Capped, polyadenylated, non-segmented, infectious |
| Envelope | Enveloped virus - lipid bilayer derived from host ER/Golgi |
| Surface projections | Club/petal-shaped glycoprotein spikes (give "corona"/crown appearance) |
| Replication site | Cytoplasm; particles mature by budding into ER and Golgi |
| Special feature | High frequency of recombination and mutation |
The club-shaped surface projections resemble a solar corona (crown) - hence the name "coronavirus."
3. DIAGRAM OF VIRUS STRUCTURE
Virion Structure (from Medical Microbiology, Murray/Sherris):
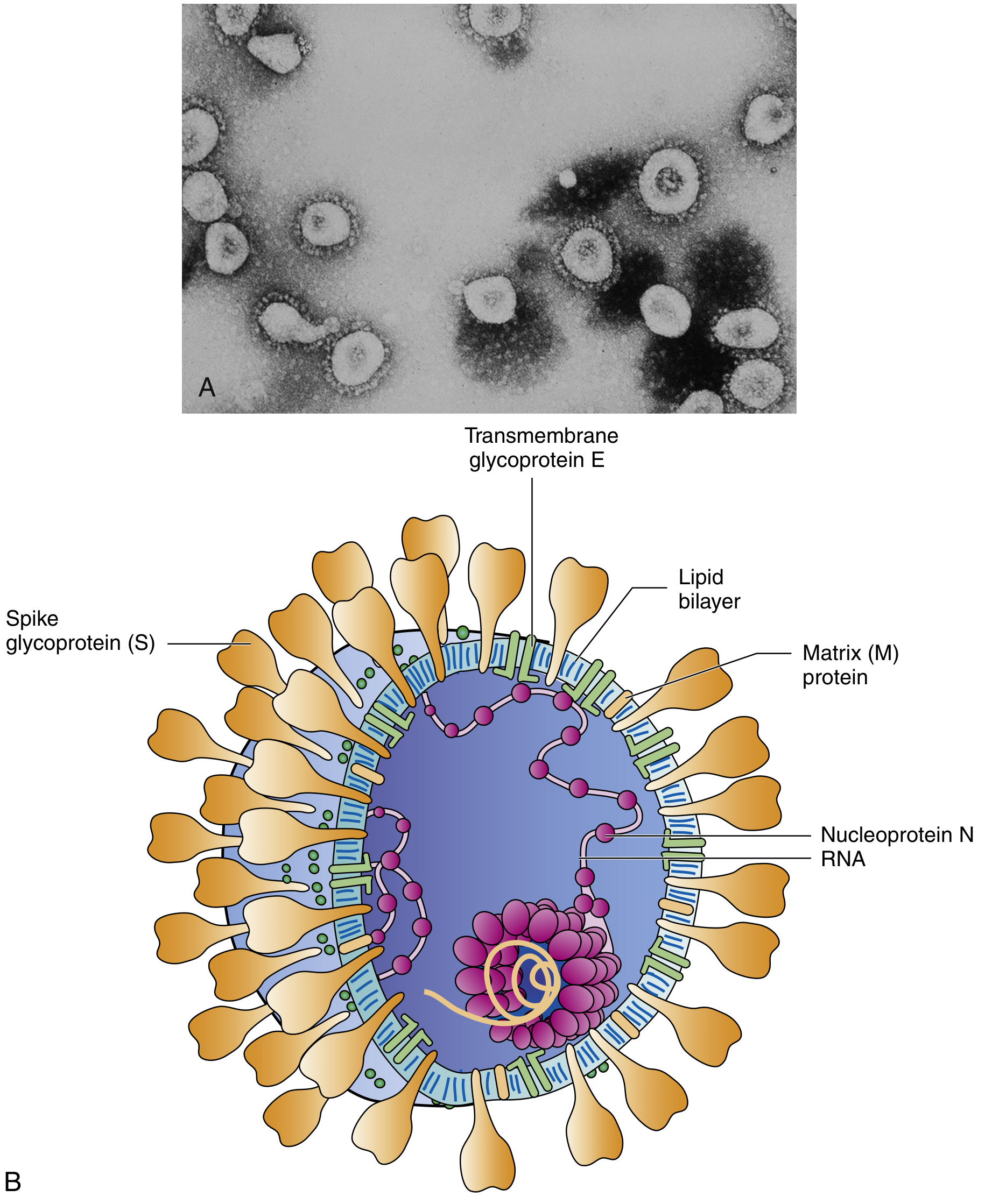
Fig: (A) Electron micrograph of coronavirus (×90,000x). (B) Model of coronavirus virion showing all structural components.
Alternate detailed diagram (Sherris & Ryan's Medical Microbiology):
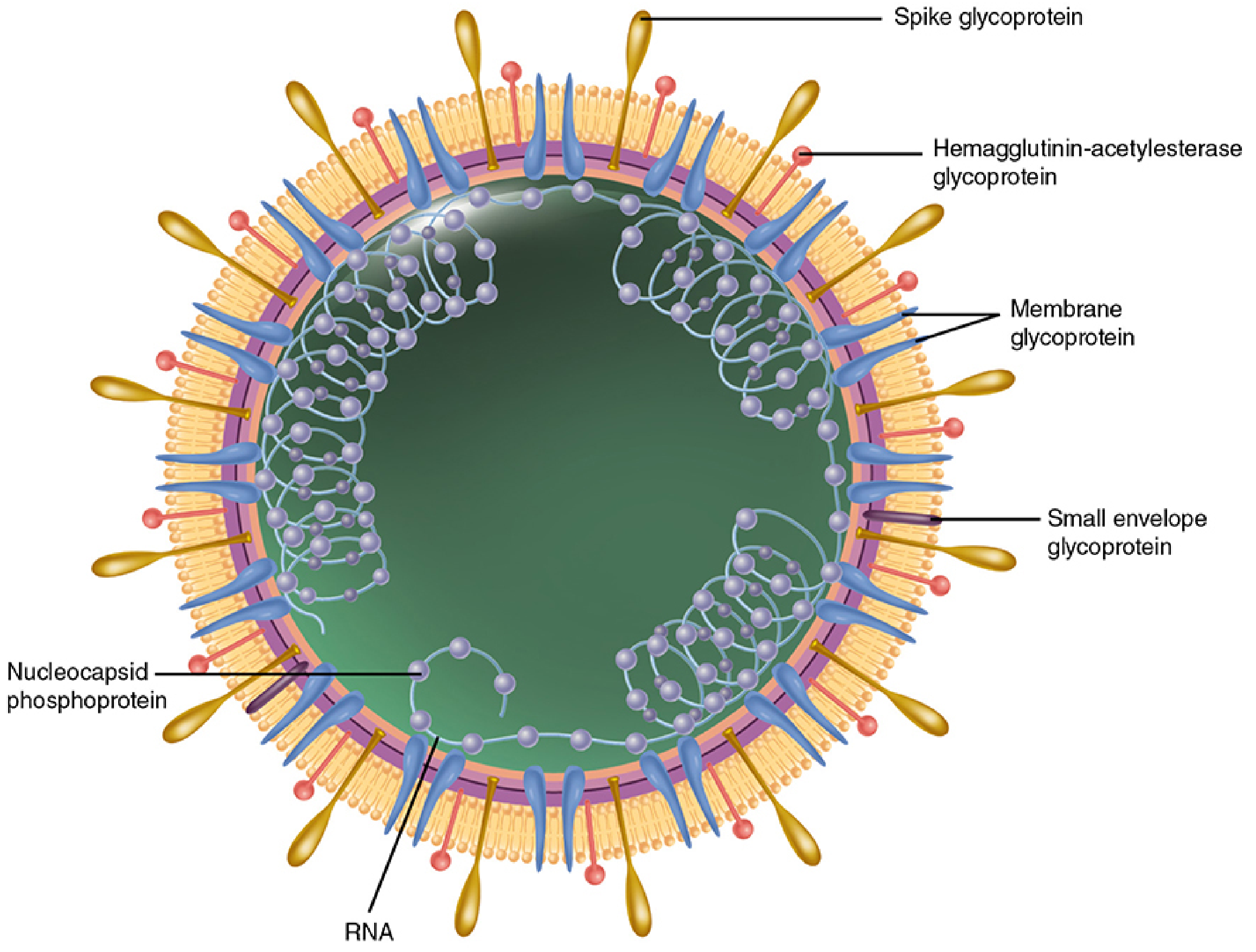
Structural Proteins (SMEN mnemonic):
| Protein | Abbreviation | Function |
|---|---|---|
| Spike glycoprotein | S | Binds ACE2 receptor; mediates entry; target of neutralizing antibodies |
| Membrane glycoprotein | M | Transmembrane matrix protein; maintains envelope shape |
| Small Envelope protein | E | Ion channel; important for viral assembly and budding |
| Nucleocapsid protein | N | Binds RNA to form helical nucleocapsid; phosphoprotein |
| Hemagglutinin-esterase | HE | Present in some strains; aids attachment and release |
Genome Organization Diagram (SARS-CoV):

Fig: Genomic organization of SARS-CoV (~29.7 kb). Yellow = structural proteins (S, E, M, N); Lavender = non-structural proteins (ORF1a/1b encode nsp1-16: RNA polymerase, helicase, proteinases, etc.)
4. VIRULENCE FACTORS
| Virulence Factor | Role |
|---|---|
| Spike (S) protein | Binds ACE2 on host cells; critical for cell entry; tropism determinant |
| ACE2 binding affinity | SARS-CoV-2 has 10-20x higher ACE2 affinity than SARS-CoV-1 |
| Furin cleavage site | Unique to SARS-CoV-2; allows S protein to be pre-activated, enhancing infectivity |
| RNA-dependent RNA polymerase (RdRp) | Encoded by ORF1b; enables rapid replication |
| Interferon antagonism | Suppresses type I IFN signaling (via nsp1, nsp3, ORF6); allows immune evasion |
| High mutation rate | Generates variants (Alpha, Delta, Omicron); immune escape |
| High recombination frequency | Unusual for non-segmented RNA viruses; drives evolution of new strains |
| Cytokine storm induction | Triggers excessive IL-6, IFN-gamma, TNF production |
| ACE2 downregulation | After entry, virus downregulates ACE2 → excess angiotensin II → lung injury |
5. PATHOGENESIS
Route of Transmission
- Primarily via respiratory droplets and aerosols (coughing, sneezing, talking, singing)
- Indoors in poorly ventilated spaces = highest risk
- Fomite transmission possible but less significant
- Fecal-oral route also described (unlike most enveloped viruses, coronaviruses can survive GI conditions due to their "corona" structure)
Step-by-Step Pathogenesis
Step 1 - Entry:
- SARS-CoV-2 Spike (S) protein binds ACE2 receptor on nasopharyngeal epithelium and type 2 alveolar pneumocytes
- TMPRSS2 (transmembrane serine protease) primes the S protein, facilitating membrane fusion
- Virus is internalized by endocytosis
Step 2 - Replication:
- Viral (+)ssRNA is directly translated to produce a polyprotein
- RNA-dependent RNA polymerase (RdRp) generates negative-sense template RNA
- New viral genomes and 5-7 subgenomic mRNAs are produced
- Viral proteins assemble; new virions bud into ER/Golgi and are released
Step 3 - Initial Immune Response:
- Innate immune response: Type I interferons (IFN-alpha, IFN-beta) attempt to suppress replication
- SARS-CoV-2 actively suppresses type I IFN signaling - this allows viral escape and high early viral load
- Presymptomatic individuals are most infectious (viral load peaks before symptoms)
Step 4 - Progression to Severe Disease (Cytokine Storm):
- In susceptible individuals (elderly, comorbidities, genetic variants in IFN pathway), viral replication is uncontrolled
- High viral loads in alveolar type 2 cells cause direct cytopathic damage
- Massive immune activation: elevated IL-6, IFN-gamma, TNF-alpha, IL-1beta = "cytokine storm"
- Resembles Systemic Inflammatory Response Syndrome (SIRS)
- Cytokine storm damages not just lungs but kidneys, heart, liver (multi-organ involvement)
Step 5 - Coagulation Activation:
- Pro-inflammatory state activates coagulation cascade
- Endothelial injury + platelet activation → microthrombi in pulmonary vasculature
- D-dimer elevated; DIC may develop
- High propensity for thromboembolism (distinguishing feature of severe COVID-19)
Step 6 - ARDS:
- Diffuse alveolar damage (DAD) - hallmark of severe disease
- Exudative phase: hyaline membranes, fibrin exudate, alveolar edema
- Progressive hypoxia → Acute Respiratory Distress Syndrome (ARDS)
- Results in respiratory failure requiring mechanical ventilation
Risk Factors for Severe Disease (from Robbins Basic Pathology)
- Age >75 years (most important risk factor)
- Comorbidities: obesity, diabetes, smoking, chronic cardiac/pulmonary/renal disease
- Male sex (higher risk than females)
- Race: African Americans, Hispanics, South Asian Americans (largely due to health disparities)
- Laboratory markers: lymphopenia, thrombocytopenia, coagulopathy, raised liver enzymes
- Genetic factors: Blood group A; germline mutations in type I IFN pathway genes
- Immunosuppression: reduces ability to mount effective adaptive immune response
6. CLINICAL MANIFESTATIONS & SYMPTOMS
Incubation Period
- Typically 4-5 days (range: 2-14 days)
- Individuals are infectious 1-2 days before symptom onset
Spectrum of Disease
| Category | Features |
|---|---|
| Asymptomatic | ~30% of infected; no symptoms but can transmit |
| Mild disease | Fever, cough, sore throat, myalgia - NO pneumonia |
| Moderate disease | Pneumonia with SpO2 >94%; dyspnea |
| Severe disease | Pneumonia + SpO2 ≤94%, RR >30/min, >50% lung involvement |
| Critical disease | Respiratory failure, mechanical ventilation, MODS, shock |
Core Symptoms
Respiratory:
- Dry cough (most common)
- Dyspnea / shortness of breath
- Sore throat
Systemic:
- Fever (>38°C)
- Myalgia (muscle pain)
- Fatigue / malaise
- Headache
Distinctive Symptoms:
- Anosmia (loss of smell) - sudden onset
- Dysgeusia (loss/change of taste) - sudden onset
- These often resolve in weeks-months but are characteristic of COVID-19
Gastrointestinal:
- Nausea, vomiting, diarrhea (more common in later variants)
Dermatological:
- "COVID toes" (pernio-like lesions on digits)
- Urticaria, maculopapular rash, vesicular eruptions
Neurological:
- Encephalopathy, delirium (in severe cases)
- Cognitive impairment ("brain fog")
- Seizures, ataxia, motor deficits (rare but reported)
Long COVID
A chronic condition present for at least 3 months after infection, with varied symptoms including fatigue, neuropsychiatric disorders, cognitive deficits, respiratory and metabolic changes.
7. COMPLICATIONS
A. Suppurative Complications (Bacterial/Fungal Secondary Infections)
COVID-19 primarily causes viral damage, but secondary infections occur especially in severe/critical cases:
| Complication | Details |
|---|---|
| Secondary bacterial pneumonia | Esp. with prolonged ICU stay, mechanical ventilation |
| Ventilator-associated pneumonia (VAP) | S. aureus, Gram-negative rods (Klebsiella, Pseudomonas) |
| Bacteremia/Septicemia | Secondary to invasive procedures or gut translocation |
| COVID-19 Associated Pulmonary Aspergillosis (CAPA) | Invasive aspergillosis in ICU patients; high mortality |
| Mucormycosis | "Black fungus" - especially in diabetics on steroids (seen prominently in Indian patients during Delta wave) |
| Lung abscess | Due to secondary bacterial superinfection |
| Hospital-acquired infections | UTI, CLABSI, wound infections from prolonged ICU stay |
Note: Bacteria are an uncommon primary complication of COVID-19; antibiotics are not routinely indicated unless bacterial co-infection is confirmed/strongly suspected.
B. Non-Suppurative Complications (Immune-Mediated & Systemic)
These are the more characteristic and numerous complications of COVID-19:
Respiratory:
- ARDS (Acute Respiratory Distress Syndrome) - major cause of mortality
- Progressive hypoxic respiratory failure
- Pulmonary fibrosis (post-COVID)
Cardiovascular:
- Myocarditis and myocardial injury (troponin elevation)
- Heart failure
- Arrhythmias (AF, VT)
- Pericarditis, pericardial effusion
Thromboembolic (very characteristic):
- Deep vein thrombosis (DVT)
- Pulmonary embolism (PE)
- Arterial thrombosis: acute stroke, limb ischemia
- Disseminated Intravascular Coagulation (DIC)
- Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) - rare platelet-activating antibody to platelet factor 4, mimicking HIT; predilection for venous/cerebral sinus thrombosis
Renal:
- Acute Kidney Injury (AKI) - due to direct viral infection of tubular cells (ACE2 expressed in kidney), cytokine-mediated, hemodynamic compromise
Neurological:
- Encephalopathy and delirium
- Acute ischemic stroke
- Guillain-Barre syndrome (GBS)
- Transverse myelitis (rare)
- Post-COVID cognitive impairment, depression, anxiety, PTSD
Multisystem Inflammatory Syndrome (MIS-C/MIS-A):
- Kawasaki-like disease in children (MIS-C)
- High fever, rash, conjunctival injection, elevated inflammatory markers
- Cardiac involvement (coronary artery dilation, myocarditis)
- Temporally related to SARS-CoV-2 infection
Hepatic:
- Elevated liver enzymes (ALT, AST)
- Mechanism: direct cytopathic effect + immune response damage
Endocrine:
- New-onset diabetes mellitus
- Thyroiditis (SARS-CoV-2-induced thyroiditis)
- Adrenal insufficiency (rare)
Ophthalmic:
- Conjunctivitis, uveitis (rare)
8. LABORATORY DIAGNOSIS
A. Specific Tests (Confirm COVID-19)
1. Molecular Tests - Gold Standard
| Test | Details |
|---|---|
| RT-PCR (Reverse Transcriptase PCR) | Most sensitive and specific; detects viral RNA; nasopharyngeal swab; processed in laboratory; not rapid |
| NAAT (Nucleic Acid Amplification Tests) | Broader category including RT-PCR, LAMP |
| Targets | N gene, RdRp gene, E gene (ORF1b/E/N gene combinations) |
| Sensitivity | ~95% (depends on timing and sample quality) |
| Limitation | Cannot be done at home; requires laboratory; detects RNA for up to 90 days post-infection |
Procedure: Viral RNA extracted → Reverse transcribed to cDNA → PCR amplification → Detection by fluorescent probes
2. Antigen Detection Tests (Rapid Antigen Test - RAT)
- Detects SARS-CoV-2 proteins (usually N protein or S protein) in nasopharyngeal sample
- Rapid results (15-30 minutes); can be done at home
- Less sensitive than RT-PCR especially in asymptomatic or pre-symptomatic individuals
- Used as screening tests; positive result is reliable; negative result should be confirmed with PCR if clinical suspicion high
3. Serology (Antibody Tests)
- Detects IgM and IgG against SARS-CoV-2 (typically S or N antigens)
- IgM: appears ~7-10 days post-infection; indicates acute/recent infection
- IgG: appears ~14 days; persists; indicates past infection or vaccination
- Not used for acute diagnosis (antibodies not present in early disease)
- Useful for sero-surveillance, retrospective diagnosis
B. Non-Specific (General) Lab Investigations
| Investigation | Finding in COVID-19 |
|---|---|
| CBC | Lymphopenia (hallmark!), thrombocytopenia, leukopenia or normal WBC |
| CRP | Markedly elevated |
| Ferritin | Elevated (cytokine storm marker) |
| IL-6 | Elevated (cytokine storm) |
| D-dimer | Elevated (coagulopathy, thrombosis risk) |
| PT/aPTT | Elevated (coagulopathy, DIC) |
| Liver enzymes (ALT, AST, LDH) | Elevated |
| Troponin, CPK | Elevated in myocardial injury |
| Creatinine | Elevated in AKI |
| Procalcitonin | Usually normal/mildly elevated (helps distinguish from bacterial pneumonia) |
C. Imaging
Chest X-Ray (CXR):
- Bilateral peripheral/lower zone consolidation and ground-glass opacities (GGO)
- May be normal early in disease despite respiratory compromise
High-Resolution CT Chest (HRCT):
- Most sensitive imaging
- Classic findings: bilateral ground-glass opacification (GGO), pleural thickening, interlobular septal thickening, consolidation, air bronchograms
- Findings systematically classified as typical, indeterminate, or atypical for COVID-19
- HRCT more sensitive than CXR but should be used for disease management, NOT as primary diagnostic tool
Lung Ultrasound:
- Bedside tool; detects B-lines (subpleural consolidations); useful in resource-limited settings
9. TREATMENT
A. Outpatient Management (Mild-Moderate Disease)
| Intervention | Details |
|---|---|
| Supportive care | Hydration, rest, fever control |
| Antipyretics | Acetaminophen (paracetamol) preferred; NSAIDs generally avoided or limited to low doses |
| Nirmatrelvir/ritonavir (Paxlovid) | Oral protease inhibitor; first-line for high-risk outpatients; given within 5 days of symptom onset |
| Molnupiravir | Oral RdRp inhibitor; alternative for outpatients; mutagenic mechanism |
| Remdesivir | IV nucleotide analog (adenosine analog); inhibits RNA polymerase; given for 3 days in early outpatient high-risk patients |
| Isolation | Infection control; mask use |
B. Inpatient Management (Moderate-Severe Disease)
Indications for hospitalization:
- SpO2 <94% on room air
- RR >30 breaths/min
- PaO2/FiO2 <300 mmHg
- Lung infiltrates >50% of lung fields
| Intervention | Details |
|---|---|
| Oxygen therapy | Titrated to maintain SpO2 ≥94%; low-flow → high-flow → NIV → mechanical ventilation |
| Remdesivir | IV antiviral (5-10 day course); for patients on supplemental oxygen |
| Dexamethasone (6 mg/day x 10 days) | Anti-inflammatory; reduces mortality in patients requiring oxygen/ventilation (RECOVERY trial); suppresses cytokine storm |
| Anticoagulation | Therapeutic-dose LMWH for all hospitalized COVID-19 patients to prevent VTE |
| Baricitinib (JAK inhibitor) | Immunomodulation + possible antiviral effect; for patients escalating on oxygen despite remdesivir + dexamethasone |
| Tocilizumab | Anti-IL-6 receptor monoclonal antibody; blocks IL-6 signaling; for severe COVID with elevated inflammatory markers |
| Abatacept/Infliximab | Alternative immunomodulators if first-line not available |
| Acetaminophen | Preferred antipyretic in hospital |
| Continue chronic medications | Aspirin, statins, ACEi/ARBs should generally be continued |
Antibiotics: NOT routinely recommended - bacterial complications are uncommon. Start empirically only when bacterial pneumonia is strongly suspected.
C. Critical Care (ICU)
| Intervention | Details |
|---|---|
| Mechanical ventilation | For respiratory failure; prone positioning reduces mortality in ARDS |
| ECMO | Extracorporeal membrane oxygenation for refractory hypoxia |
| High-dose immunomodulators | Baricitinib or tocilizumab continued/started in ICU |
| Vasopressors | For septic shock/cytokine storm hemodynamic compromise |
| Renal replacement therapy | For severe AKI/oliguric renal failure |
D. Antibody-Based Therapies
- Convalescent plasma - blood plasma from recovered patients; effectiveness limited by variant evolution
- Monoclonal antibodies (mAbs) - neutralizing antibodies against Spike protein (e.g., sotrovimab); effectiveness varies by variant
E. Prevention
| Method | Details |
|---|---|
| mRNA vaccines | BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna); encode Spike protein |
| Viral vector vaccines | ChAdOx1 (AstraZeneca), Ad26.COV2.S (J&J) |
| Inactivated virus vaccines | Covaxin (Bharat Biotech), CoronaVac (Sinovac) |
| Protein subunit vaccines | NVX-CoV2373 (Novavax) |
| Non-pharmacological | Masking, hand hygiene, ventilation, social distancing |
QUICK REVISION TABLE - COVID-19 at a Glance
| Feature | Key Point |
|---|---|
| Virus | SARS-CoV-2, Betacoronavirus |
| Genome | +ssRNA, 29.7 kb |
| Size | 80-160 nm |
| Receptor | ACE2 |
| Entry co-factor | TMPRSS2 |
| Key virulence factor | Spike (S) protein |
| Incubation | 4-5 days (up to 14) |
| Peak infectivity | Pre-symptomatic / early symptomatic |
| Lab hallmark | Lymphopenia + elevated D-dimer + elevated IL-6 |
| Gold standard diagnosis | RT-PCR |
| Imaging hallmark | Bilateral GGO on HRCT chest |
| Antiviral drug | Remdesivir (IV), Nirmatrelvir/ritonavir (oral) |
| Anti-inflammatory | Dexamethasone (6mg/day) |
| Anti-IL-6 | Tocilizumab |
| JAK inhibitor | Baricitinib |
| Major complication | ARDS |
| Characteristic complication | Thromboembolic disease + cytokine storm |
| MIS-C | Kawasaki-like illness in children |
Sources:
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed, Chapter 41 (Coronaviruses)
- Medical Microbiology 9e (Murray), Chapter 47 (Coronavirus Structure and Replication)
- Sherris & Ryan's Medical Microbiology, 8th Ed, Chapter 9 (Virion Structure)
- Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 11 (COVID-19 Pathogenesis)
- Harrison's Principles of Internal Medicine, 22nd Ed (2025), Chapter 205 (COVID-19 Clinical Manifestations, Diagnosis, Treatment)
- Goldman-Cecil Medicine, International Edition (COVID-19 Thrombotic Complications)
This is a shared conversation. Sign in to Orris to start your own chat.