



+4 more
Lesions in an 55 year old female present with itching and mild burning sensation on bilateral limbs what could it be
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Searching PubMed
lichen planus pigmentosus diagnosis treatment
Loading Image
Reading File
Reading File
Loading Image
I now have enough information for a thorough, well-sourced response. Let me compile it.
Most Likely Diagnosis: Lichen Planus (LP) with Lichen Planus Pigmentosus (LPP) features
What the images show
Analyzing all four photos together:
| Image | Findings | Significance |
|---|---|---|
| Shoulder/upper arm | Single smooth, shiny, pearlescent oval raised plaque | Classic LP plaque or morphea-like LP |
| Dorsal hand #1 | Multiple small skin-colored to pink papules + hypopigmented patch | Classic LP papules on dorsal hand (a hallmark site) |
| Forearm (blurry) | Multiple oval, dark violaceous-brown macules arranged in a linear/grouped pattern | Lichen planus pigmentosus or resolving LP with post-inflammatory hyperpigmentation |
| Wrist/dorsal hand #2 | Small discrete papules on xerotic skin background | Active LP papules |
The bilateral, symmetric distribution on the limbs, the violaceous papules on dorsal hands, and the dark hyperpigmented oval macules on the forearms in a middle-aged woman fit LP and LPP very well.
Lichen Planus - Core Features
LP is a T-cell mediated inflammatory dermatosis with increased Th1 cytokine expression at the basement membrane zone.
Classic lesion: Small, flat-topped, polygonal, violaceous papules with a glistening surface. Wickham striae (white/gray streaks on surface) are pathognomonic. Lesions start pinpoint and expand to 0.5-1.5 cm plaques.
Predilection sites: Flexor wrists, dorsal hands, medial thighs, shins, trunk - exactly matching this patient's distribution.
Symptoms: Pruritus is prominent and often disproportionate to the visible lesion load. Patients typically rub rather than scratch. Mild burning sensation is also reported.
Symmetry: Bilateral and relatively symmetric distribution is characteristic.
- Andrews' Diseases of the Skin, p. 259
Here is what koebnerized LP looks like on a limb (note the linear shiny plaque - very similar to image 1):

Lichen Planus Pigmentosus (LPP) - Explaining the Dark Macules
LPP is a recognized variant of LP, particularly common in darker-skinned, South/Southeast Asian and Middle Eastern individuals.
Features:
- Symmetrical brown to gray-brown poorly demarcated macules and patches
- Mainly photoexposed sites (face, neck, dorsal hands/arms) but also flexural folds
- The dark oval macules seen on the forearm in image 3 match this perfectly
- Associated with mustard oil and amla oil use (worth asking about)
- Histology: epidermal atrophy, basal vacuolation, perivascular lymphocytic infiltrate, melanophages in superficial dermis
Here is a textbook example of LPP on the neck (note the coalescing hyperpigmented macules):
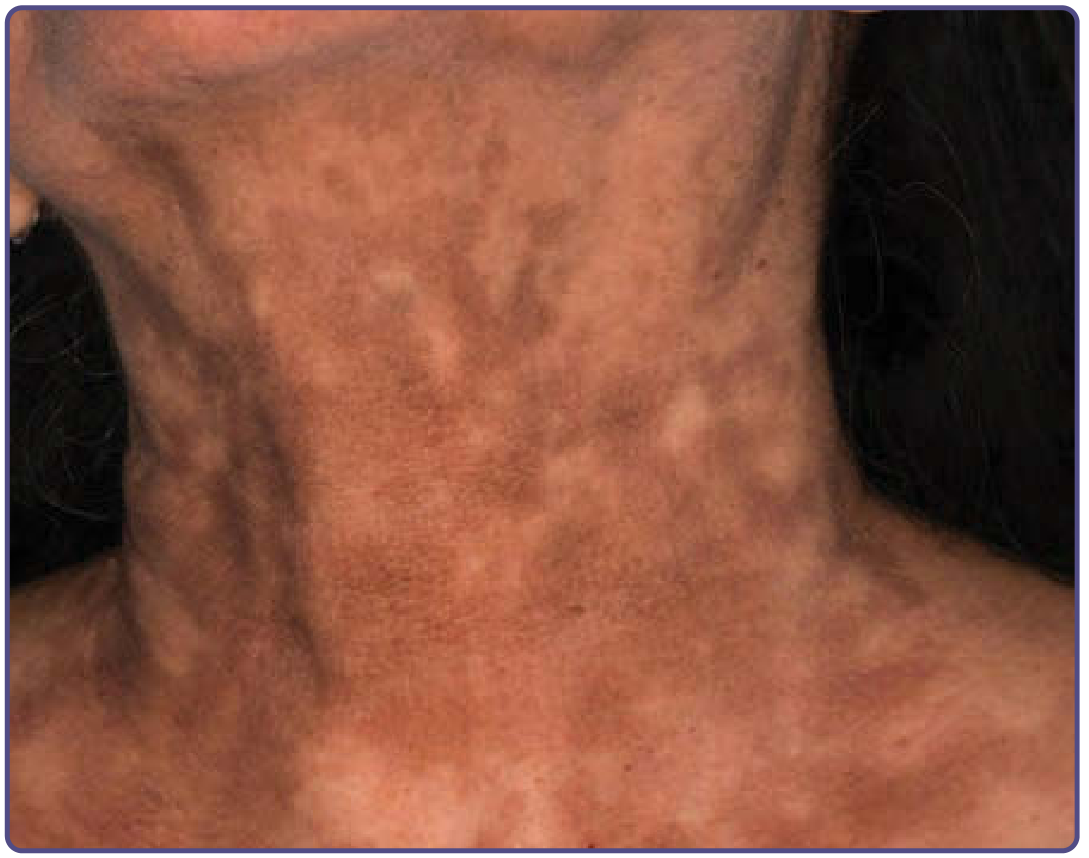
- Fitzpatrick's Dermatology, p. 1415
Differential Diagnoses to Consider
| Condition | Points for | Points against |
|---|---|---|
| Lichen Planus | Bilateral limbs, papules on dorsal hands/wrists, pruritus, burning, age group | Need Wickham striae confirmation |
| Lichen Planus Pigmentosus | Dark oval macules, darker skin, bilateral arms | Typically less pruritic |
| Prurigo Nodularis | Papules, pruritus | Usually more excoriated, dome-shaped nodules |
| Fixed Drug Eruption | Oval hyperpigmented macules | Usually fewer, recur at same site with drug exposure |
| Erythema Dyschromicum Perstans (Ashy Dermatosis) | Gray-brown macules, similar histology | Tends to involve trunk more |
| Morphea | The shiny shoulder plaque (image 1) | Morphea typically ivory/white, non-pruritic |
What to do next
- Dermoscopy - look for Wickham striae (white lines/dots) on the papules, confirms LP in most cases
- Skin biopsy - especially of a papule and a hyperpigmented macule separately - shows lichenoid tissue reaction (band-like lymphocytic infiltrate at DEJ, basal vacuolation, colloid bodies)
- Drug history - many drugs cause lichenoid reactions (ACE inhibitors, thiazides, NSAIDs, antimalarials, beta-blockers)
- Ask about mustard oil/amla oil use (LPP association)
- Check oral mucosa - up to 70% of LP patients have oral involvement (reticulate white patches on buccal mucosa)
- Hepatitis C serology - LP has a well-established association with HCV
Management (once confirmed)
- First-line: Topical corticosteroids (mid-to-high potency, e.g., betamethasone valerate, clobetasol) for active papules
- Pruritus: Oral antihistamines, topical tacrolimus or pimecrolimus for sensitive areas
- Widespread disease: Systemic steroids (short course), acitretin, hydroxychloroquine, cyclosporine, or methotrexate
- LPP pigmentation: Sunscreen, topical retinoids, azelaic acid - note that treatments give only minimal improvement in established pigmentation per Fitzpatrick's
- A 2026 systematic review in Dermatol Surg found laser therapy (Q-switched Nd:YAG, fractional) may offer benefit for LPP pigmentation (PMID: 40965050)
Bottom line: This 55-year-old woman most likely has Lichen Planus with Lichen Planus Pigmentosus features - a T-cell mediated inflammatory condition. The bilateral symmetric distribution, violaceous papules on dorsal hands/wrists, dark hyperpigmented oval macules on the forearms, pruritus, and mild burning are all characteristic. Biopsy and dermoscopy would confirm the diagnosis. A drug and oil exposure history plus hepatitis C serology should be obtained.
Disclaimer: This is educational clinical analysis, not a substitute for in-person examination and diagnosis by a licensed dermatologist. Please refer the patient for formal evaluation and biopsy.
This is a shared conversation. Sign in to Orris to start your own chat.