Teach me all endoscopic urology instrument along with detail of each part of instrument in interesting and memorizable way... Teach me along with pics and mechanics of each instrument also teach me types , classification of each instrument all the from authentic sources
Reading File
Finding Sources
Finding Sources
Searching the Web
endoscopic urology instruments classification parts cystoscope ureteroscope resectoscope nephroscope
Finding Sources
Finding Sources
Reading Web Page
https://www.slideshare.net/slideshow/cystoscope-nephroscope-…
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Searching the Web
nephroscope PCNL parts resectoscope parts ureteroscope flexible digital parts classification urology endoscopy
Loading Image
Reading Web Page
https://besdatatech.com/ureteroscope-guide
Finding Sources
I now have comprehensive content from textbooks, web resources, and images. Let me compile the complete, detailed, memorable educational guide.
🔭 The Complete Guide to Endoscopic Urology Instruments
Sources: Bailey & Love's Short Practice of Surgery 28th Ed., Pfenninger & Fowler's Procedures for Primary Care 3rd Ed., Campbell-Walsh-Wein Urology, BESDATA Ureteroscope Guide, and clinical manufacturer catalogs (Karl Storz, Richard Wolf, Olympus).
🧠 MASTER MEMORY FRAMEWORK
Use this acronym to remember all major instruments:
"Can Urologists Really Navigate Pelvic Stones?"
- C - Cystoscope
- U - Ureteroscope
- R - Resectoscope
- N - Nephroscope
- P - Percutaneous Access Instruments (dilators, sheaths)
- S - Special instruments (urethrotome/VIU, lithotriptors, stent introducers)
⚙️ PART 1: THE CYSTOSCOPE
What is it?
The cystoscope is your gateway to the lower urinary tract - the first and most foundational endourological instrument. Think of it as a periscope for the bladder.
CLASSIFICATION: Rigid vs. Flexible
| Feature | Rigid Cystoscope | Flexible Cystoscope |
|---|---|---|
| Anaesthesia | General/spinal preferred | Local anaesthesia (lidocaine gel) |
| Optics | Hopkins rod-lens system | Fiberoptic bundles / CCD chip |
| Irrigation | Separate in/outflow taps on sheath | Integrated single channel |
| Lens change | Remove & swap telescopes | Entire scope must be removed |
| Patient position | Lithotomy (legs up) | Supine (comfortable) |
| Procedures | Full range - biopsy, resection, catheter, stents | Limited - surveillance, stent removal, small biopsies |
| Image quality | Superior | Adequate for diagnosis |
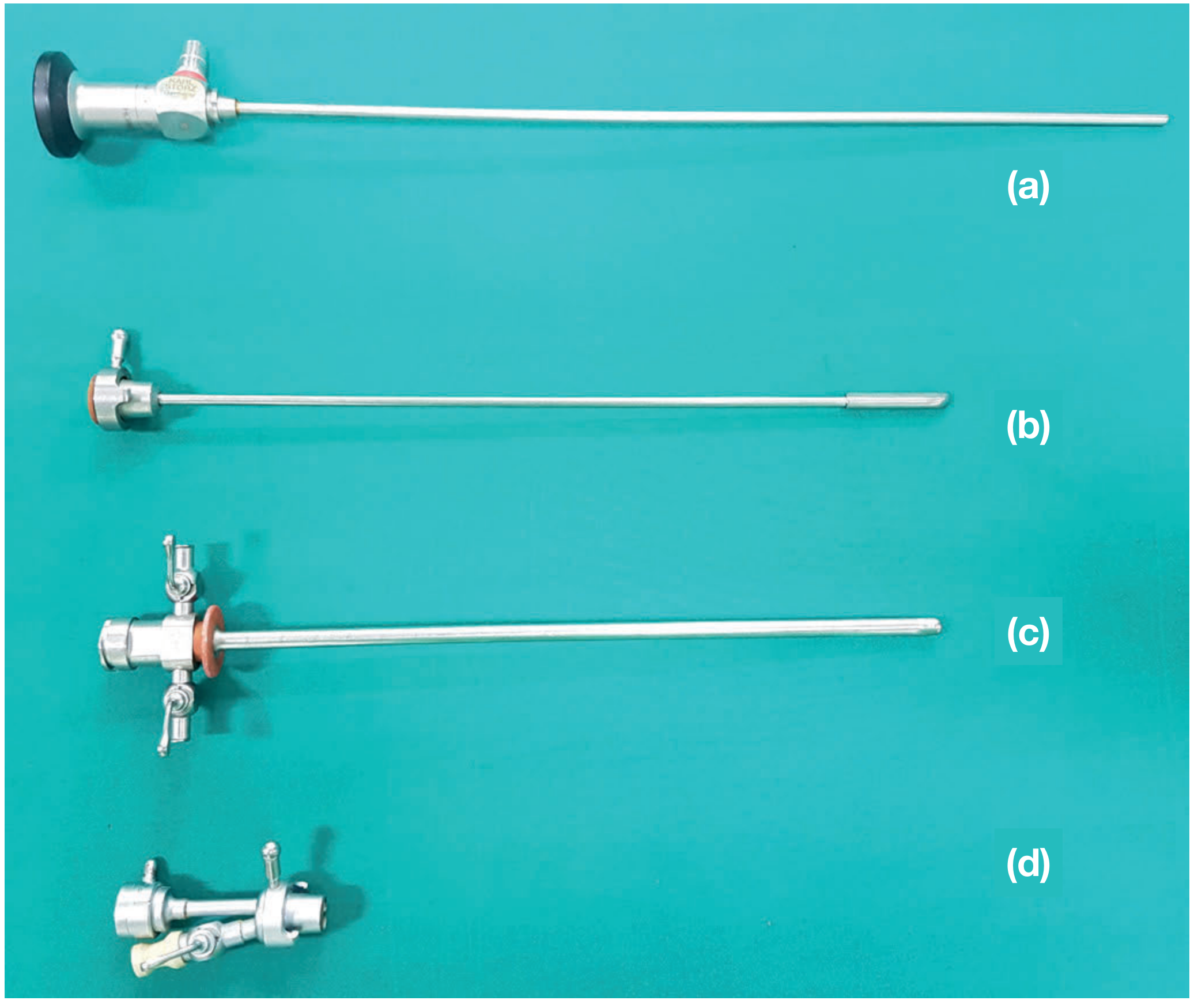
PARTS OF THE RIGID CYSTOSCOPE (The "TOBS" System)
Memory trick: "The Old Bridge Speaks" = Telescope - Obturator - Bridge - Sheath
1. TELESCOPE 🔭
- The optical core - contains the Hopkins rod-lens system (invented by Prof. Harold Hopkins, revolutionizing urology)
- Size: 4 mm diameter, 30 cm length (fits all sheaths)
- Light post: connects to external fibreoptic light cable
- Eyepiece/camera port: top of the telescope; camera head attaches here
Classified by VIEWING ANGLE:
| Angle | Name | Use | Memory Trick |
|---|---|---|---|
| 0° | Forward/Straight | Urethroscopy (straight ahead) | "0 = go straight" |
| 12° | Forward oblique | Urethra & bladder neck | "12 = slight detour" |
| 30° | Forward oblique | Base & anterolateral bladder, ureteral orifices | "30 = standard workhorse" |
| 70° | Lateral | Bladder dome & lateral walls | "70 = look sideways up" |
| 120° | Retrograde/Retrospective | Anterior bladder neck from inside | "120 = look backwards" |
Clinical Pearl: With flexible cystoscopes rising in popularity, the 70° and 120° rigid telescopes are becoming obsolete. The 30° is the most commonly used. (Pfenninger & Fowler, p.799)
How the Hopkins Rod-Lens System works:
Traditional scopes used air-filled tubes with small glass lenses. Hopkins reversed this - he used long glass rods with air spaces in between. More glass = more light transmission = brighter, clearer image. This was the single greatest optical revolution in endourology.
2. SHEATH (Outer Tube) 🧪
- The metal tube that goes into the patient - it is the vehicle
- Size: 17-26 French (Fr) diameter (1 Fr = 0.33 mm)
- Has inflow and outflow ports (stopcocks/taps) for irrigation fluid
- Beak of the sheath: the distal tip, designed to be atraumatic (bulbous dorsally, smooth)
- Has calibration markings to measure prostatic urethral length
- A sheath with beak can be passed without an obturator; without beak (e.g., VIU/resectoscope sheath), it needs an obturator
Measuring prostatic urethral length with the sheath:
- Insert scope fully → note external meatus marking (Point A)
- Withdraw to bladder neck → note marking (Point B)
- Withdraw further to verumontanum → note marking (Point C)
- Distance B-C = prostatic urethral length
Irrigation fluids:
- Saline or Ringer's lactate: for procedures without electrocautery
- Non-conducting solutions (glycine, sorbitol, mannitol, sterile water): required for monopolar electrocautery to avoid current dissipation
3. OBTURATOR 🔵
- The blunt solid inner rod that occupies the sheath during blind insertion
- Prevents trauma by replacing the sharp telescope during passage
- Used in females (shorter urethra, blind insertion possible) and when the sheath beak doesn't allow direct vision insertion
- Memory trick: "Obturator = Obstacle-remover" - it smoothens entry
4. BRIDGE 🌉
- The connector between the telescope and sheath - like a bridge joining two shores
- Provides an extra length (the bridge adds the "male extra length" because male urethra is longer)
- Has working channel ports - typically 1 or 2 channels
- One-channel bridge: passage of a single 5-7 Fr instrument
- Two-channel bridge: simultaneous use of 2 instruments (e.g., catheter + forceps)
- The bridge also seals the scope-sheath assembly to maintain irrigation pressure
PARTS OF THE FLEXIBLE CYSTOSCOPE
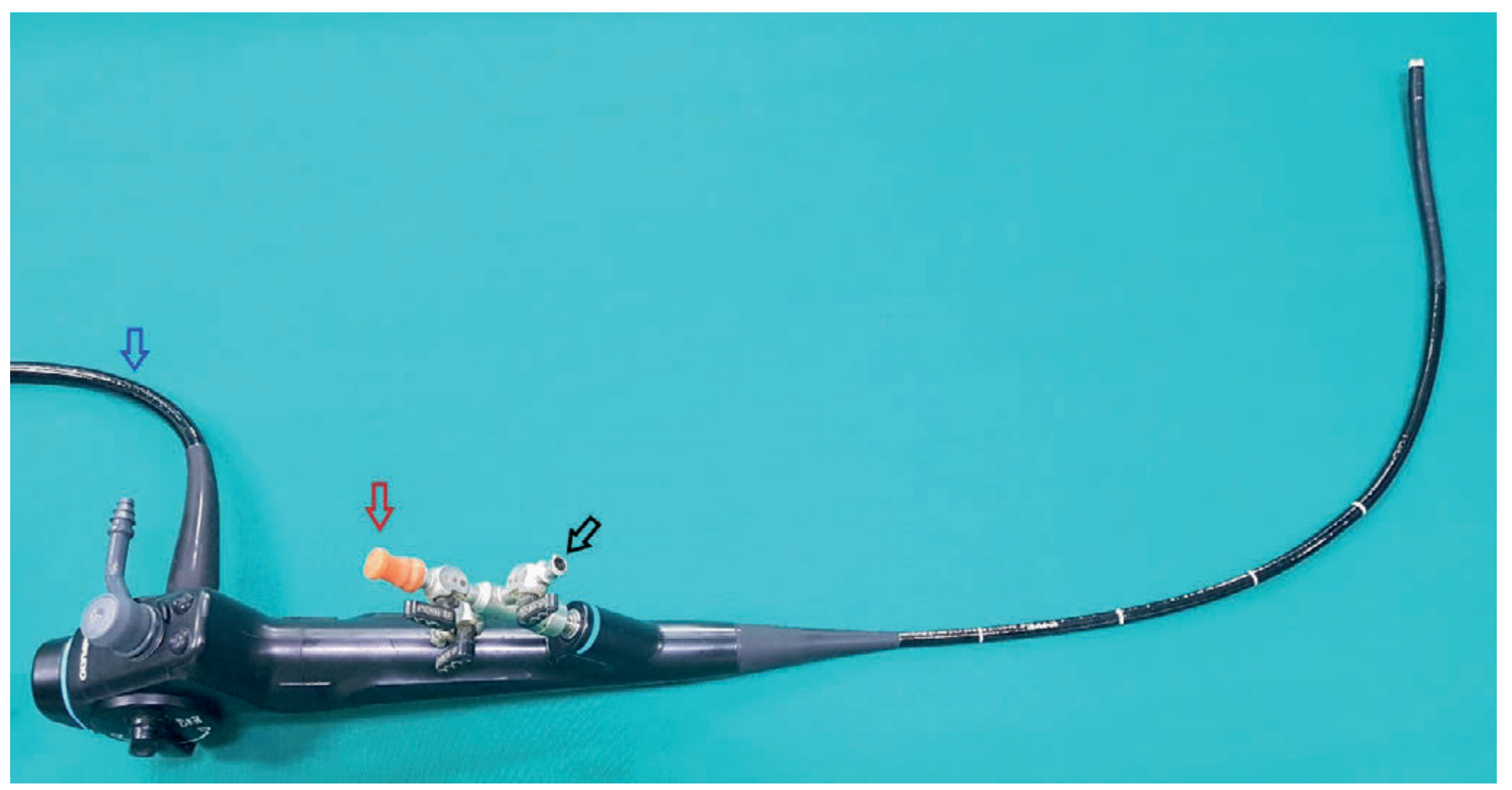
The flexible scope is an integrated single-unit - no separate sheath or bridge. Its parts:
| Part | Function |
|---|---|
| Body/Handle | Held by surgeon; contains deflection lever, working channel port, irrigation taps |
| Deflection lever | Controls tip angulation - up to 290° in a single plane |
| Working channel port | Entry for 5-6 Fr instruments (smaller than rigid) |
| Light post | Connects fibreoptic light cable |
| Video connection | Connects to camera/monitor system |
| Insertion tube (shaft) | Long flexible shaft housing fibers, working channel, deflection wires |
| Distal tip | Houses objective lens or CCD chip; deflects actively |
Two subtypes of flexible cystoscopes:
- Fiberoptic (conventional): Image transmitted via glass fiber bundles; has eyepiece
- Digital (videoscope): CCD/CMOS chip at the tip sends electronic signals directly to monitor; superior resolution; no fiber "pixelation"
⚙️ PART 2: THE URETEROSCOPE
What is it?
An ureteroscope is a longer, narrower cystoscope designed to travel past the bladder and up into the ureter and renal pelvis. Think of it as a deep-sea explorer going into increasingly narrow territory.
History:
- 1979: First dedicated ureteroscope designed by Richard Wolf Medical Instruments
- 1985: First fiberoptic ureteroscope by ACMI
- 2000s: Digital (chip-on-tip) flexible ureteroscopes introduced
CLASSIFICATION: Three Main Types
TYPE 1: RIGID URETEROSCOPE
- Completely inflexible shaft
- Best for distal/lower ureter (straight anatomical segments)
- Optics: rod-lens or fiberoptic
- Largely replaced by semirigid but still used in some settings
TYPE 2: SEMI-RIGID URETEROSCOPE
- Most commonly used in current practice
- Has slight inherent bendability but no active deflection
- Sizing is expressed as two numbers (e.g., 7/8.5):
- First number = tip diameter (7 Fr)
- Second number = shaft diameter (8.5 Fr)
- Common sizes: 6/7.5, 7/8.5, 8/9.5
- Length: Short = 35 cm (females); Long = 45 cm (males)
- All modern semirigid URS have optical fibers
- Working channel: straight (for pneumatic lithotripsy) or oblique (for laser - "uretero-laser scope")
TYPE 3: FLEXIBLE URETEROSCOPE
- Actively deflecting tip (180-270°+ deflection)
- Reaches the entire upper urinary tract including all renal calyces
- Fiberoptic vs Digital (video) subtypes:
| Fiberoptic URS | Digital URS | |
|---|---|---|
| Image capture | Fiber bundles → eyepiece → camera | CCD/CMOS chip at tip |
| Image quality | Good but "pixelated" fiber pattern | High definition, superior |
| Durability | Less durable (fragile fibers) | More durable |
| Cost | Less expensive | More expensive |
| Single-use variants | Available | Growing category |
PARTS OF THE URETEROSCOPE
Memory trick: "HELLO WIDE" = Handle - Eyepiece/LED - Light post - Lever (deflection) - Optical system - Working channel - Insertion tube - Distal tip - Extension
| Part | Detail |
|---|---|
| Eyepiece (Fiberoptic) | Ocular lens; magnifies and makes image visible; has focusing ring |
| Handle/Body | Proximal; ergonomic grip; houses working channel port, irrigation inlets |
| Deflection lever (flexible) | Moves tip up-down; some scopes have 4-way deflection |
| Light post | Connects fibreoptic light source cable |
| Working channel | 1 or 2 channels; most have single ~3.6 Fr channel (or dual smaller channels) |
| Insertion tube/shaft | Long slim shaft; the "corridor" into the ureter |
| Distal tip | Tapered for atraumatic entry; houses lens/sensor and channel exit; laser-resistant materials at channel opening |
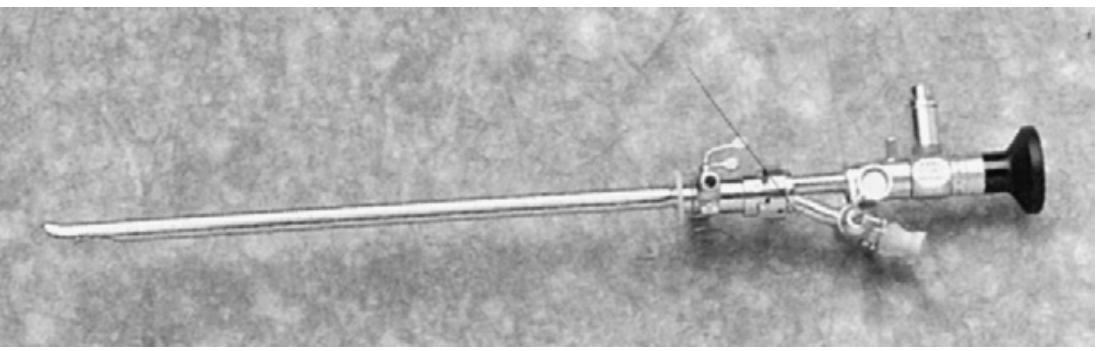
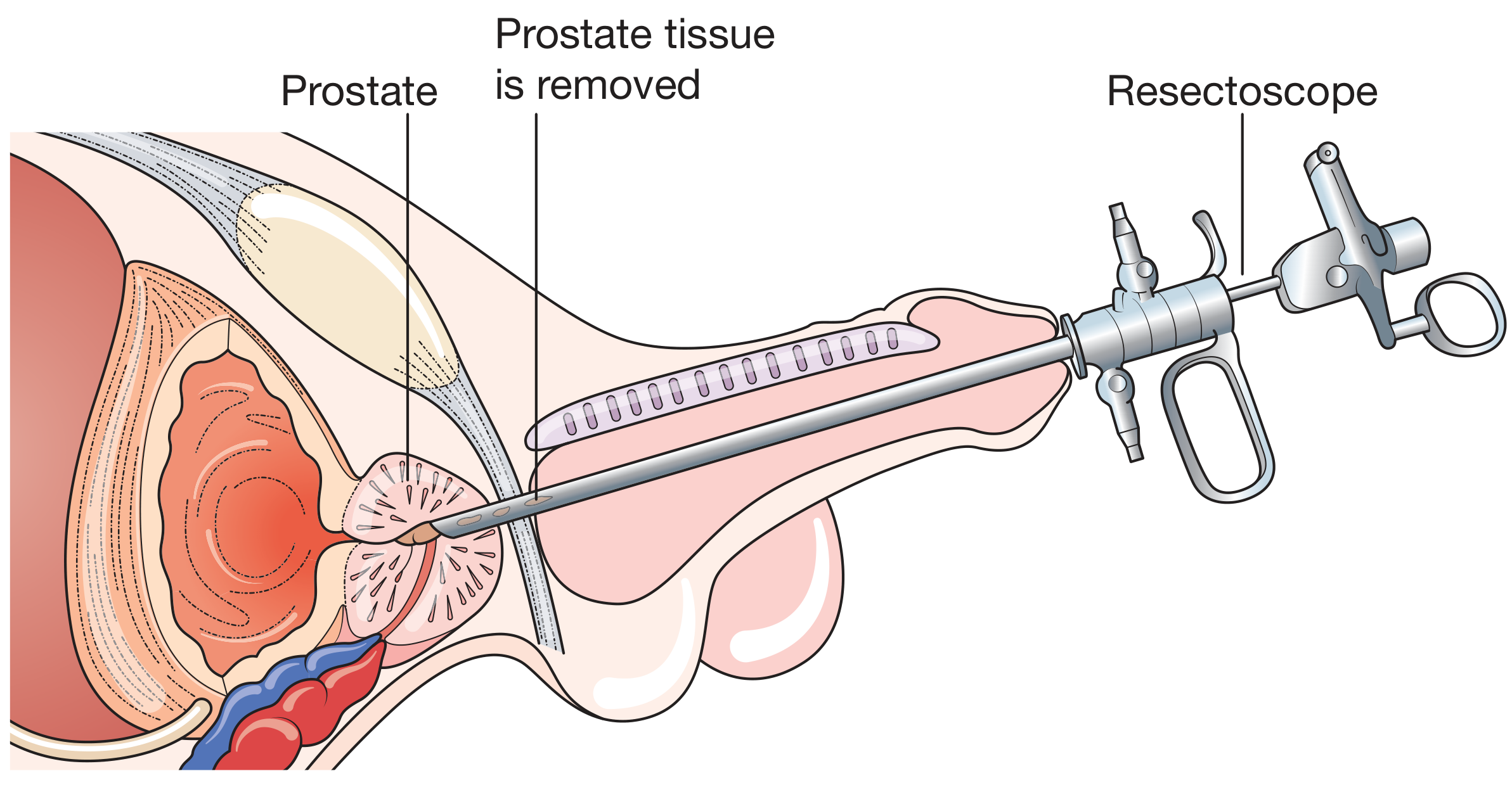
⚙️ PART 3: THE RESECTOSCOPE
What is it?
The resectoscope is the surgical workhorse of endourology - it is what removes prostate tissue in TURP and cuts bladder tumors in TURBT. Think of it as a lawnmower inside the bladder.
Historical note: The greatest advance was Prof. Harold Hopkins' rigid lens system - the same that transformed cystoscopes. His fibreoptic-illuminated lenses provide unparalleled visualization. (Bailey & Love's, p.1550)
CLASSIFICATION
By Current Type:
| Type | Irrigant Used | Mechanism | Risk of TURP Syndrome |
|---|---|---|---|
| Monopolar (conventional) | Non-conducting (glycine 1%, sorbitol, mannitol) | Current passes patient → return plate | Yes (hyponatremia risk) |
| Bipolar (modern) | Normal saline | Current flows loop → adjacent electrode | No (saline = physiological) |
Resection time limit: Monopolar TURP is limited to 1 hour due to risk of fluid resorption with glycine. Bipolar TURP with saline has no such time constraint and allows larger prostates to be resected safely. (Bailey & Love's, p.1550)
By Procedure:
- TURP (Transurethral Resection of Prostate)
- TURBT (Transurethral Resection of Bladder Tumour)
- Bladder neck incision (Collins knife)
PARTS OF THE RESECTOSCOPE
Memory trick: "SLOW TRIP" = Sheath - Loop electrode - Optical telescope - Working element - Telescope (30°) - Roller/Rollerball - Irrigation ports - Passive/active mechanism
| Part | Detail |
|---|---|
| Outer sheath | 24-28 Fr; fits transurethrally; has large inflow/outflow ports for continuous irrigation |
| Inner sheath (Albarran/deflector) | Optional; can deflect instruments |
| Resectoscope body/handle | Pistol-grip mechanism; thumb moves working element back and forth |
| Working element | The "gun trigger" - moves the loop forward (cut) and back (passive/spring return) |
| Telescope (30°) | Standard is 30° forward oblique lens for TURP; gives best view of lateral lobes |
| Diathermy loop | Tungsten wire loop; activated by high-frequency current; cuts and coagulates |
| Rollerball/roller electrode | Used for coagulation only (not cutting); rolls over bleeding points |
| Irrigation ports | Inflow = bring clear fluid in; Outflow = carry "chips" and blood out; continuous flow = constant clear field |
How the resection works (step by step):
- Loop is extended forward past the tissue
- Current is activated (cutting mode)
- Loop is drawn back through the tissue → a strip ("chip") is cut
- Coagulation current stops bleeding
- Chips accumulate → periodically washed out with an Ellik evacuator
- Procedure ends when adequate channel is created through the prostate
Resection rate: Approximately 1 gram of prostate per minute in experienced hands.
⚙️ PART 4: THE NEPHROSCOPE
What is it?
The nephroscope is a thick, short, sturdy scope used via a surgically created track into the kidney (percutaneous route). If the cystoscope is a periscope and the ureteroscope is a deep-sea explorer, the nephroscope is a drill-and-tunnel engineer accessing a kidney stone from outside.
Used for: Percutaneous Nephrolithotomy (PCNL) - removal of large kidney stones (>20mm) that cannot pass or be broken with ESWL.
CLASSIFICATION
By Size:
| Type | Sheath Size | Use |
|---|---|---|
| Standard PCNL | 24-30 Fr | Large staghorn/complex stones |
| Mini-PCNL | 14-20 Fr | Medium stones, reduced morbidity |
| Ultra-mini/Micro-PCNL | 8-14 Fr | Small calyceal stones, pediatrics |
| Micro-PCNL | 4.8-8 Fr | Exclusively for stone dusting |
By Optics:
- Standard nephroscope (30° lens, rod-lens system)
- Flexible nephroscope (used in difficult calyceal positions)
- Combined cysto-nephroscope (flexible dual-purpose scopes, e.g., Olympus CYF-VH)
PARTS OF THE NEPHROSCOPE
| Part | Detail |
|---|---|
| Telescope | Typically 12° or 0° forward-oblique; rod-lens system; 4 mm diameter |
| Sheath | Short (15-20 cm), wide (24-30 Fr) to accommodate large instruments; designed for PCNL tract |
| Obturator | Solid rod used to introduce sheath into the established tract |
| Working channels | Large (up to 8 Fr); accepts nephroscopy forceps, ultrasonic/pneumatic probes, laser fibers |
| Irrigation ports | High-flow inflow and outflow; essential to maintain clear vision during stone fragmentation |
| Instrument arm | Angled working arm allows tools to be directed toward the stone |
The PCNL Setup Sequence:
- Percutaneous needle puncture into renal calyx (under fluoroscopy/ultrasound)
- Guidewire passed through needle
- Track dilated (Alken metal dilators, Amplatz dilators, or one-step balloon dilator)
- Amplatz sheath (30 Fr) placed to maintain tract
- Nephroscope introduced through the sheath
- Stone fragmented with pneumatic, ultrasonic, or laser lithotriptor
- Fragments removed with nephroscopy forceps/basket
⚙️ PART 5: THE URETHROTOME (VIU Sheath)
What is it?
Used for Visual Internal Urethrotomy (VIU) - cutting urethral strictures under direct vision. It is similar to a cystoscope sheath but the sheath requires an obturator (no beak design), and a cold knife or Otis urethrotome is passed through the working channel.
Key difference from cystoscope sheath: VIU sheath has no atraumatic beak, so it MUST be passed with an obturator.
⚙️ PART 6: THE UROLOGY STACK & ACCESSORIES
Every endourological procedure depends on a surrounding system - the urology stack. Think of it as the mission control for endoscopy.
| Component | Function |
|---|---|
| Light source | Xenon or LED 300W; supplies bright white light via fibreoptic cable |
| Fibreoptic light cable | Transmits light from source to telescope; must never be kinked |
| Camera head | Attaches to telescope eyepiece; converts optical image to digital signal |
| Monitor (HD/4K) | Displays the operative field; allows documentation |
| Image processor | Processes camera signal; may include NBI/narrow-band imaging |
| Irrigation system | Hanging bags (500 mL-3 L) on IV pole; controlled via stopcocks |
| Electrocautery/diathermy unit | Generator for monopolar or bipolar current; essential for resection/coagulation |
⚙️ PART 7: ACCESSORY INSTRUMENTS (passed through working channels)
These are the tools that work through the cystoscope, ureteroscope, or nephroscope:
| Instrument | Size | Function |
|---|---|---|
| Biopsy forceps | 5 Fr, 43 cm (rigid) / flexible variants | Take tissue samples |
| Grasping forceps | 3-5 Fr | Retrieve foreign bodies, stone fragments |
| Ureteral catheters | 3-6 Fr | Retrograde pyelography, stent guidance |
| Dormia basket / Stone basket | 3-5 Fr | Capture and extract ureteral stones |
| Balloon dilator | 4-7 Fr | Dilate ureteral orifice / PCNL tract |
| Laser fiber | 200-600 µm | Holmium, Thulium, or TFL laser lithotripsy |
| Pneumatic lithotripsy probe | Straight channel only | Mechanical stone fragmentation |
| Roller electrode | 24+ Fr sheath | Bladder fulguration, TURBT hemostasis |
| Collins knife | Resectoscope sheath | Bladder neck incision |
| Ellik evacuator | Post-resection | Wash out prostate chips from bladder |
🗺️ ANATOMICAL ROUTE MAP: Which Scope Goes Where?
EXTERNAL MEATUS
↓ [Cystoscope sheath enters here]
URETHRA ← Cystoscope (0° lens), VIU/urethrotome
↓
BLADDER ← Cystoscope (30° & 70° lens), Resectoscope (TURP/TURBT)
↓
URETERAL ORIFICE ← Cystoscope identifies, guides ureteroscope
↓
URETER ← Semi-rigid Ureteroscope (lower/mid ureter)
↓
RENAL PELVIS ← Flexible Ureteroscope (URS)
↓
RENAL CALYCES ← Flexible URS or Nephroscope (percutaneous track)
↑
EXTERNAL FLANK
Nephroscope enters via PCNL track
🎓 QUICK COMPARISON TABLE
| Feature | Cystoscope | Ureteroscope (semirigid) | Resectoscope | Nephroscope |
|---|---|---|---|---|
| French size | 17-26 Fr | 6-9 Fr tip | 24-28 Fr | 24-30 Fr |
| Length | 30 cm | 35-45 cm | 30 cm | 15-20 cm |
| Telescope angle | 0°, 30°, 70°, 120° | 0° | 30° | 12° |
| Working channel | 5-7 Fr | 3.6-4 Fr | Large (loop) | 6-10 Fr |
| Irrigation | In/out taps | Single port | Continuous flow | High-flow in/out |
| Access route | Transurethral | Transurethral → ureter | Transurethral | Percutaneous flank |
| Key use | Diagnosis, stents, biopsies | Stone, stricture, tumour (ureter/kidney) | TURP, TURBT | Large renal stones (PCNL) |
📌 HIGH-YIELD EXAM FACTS
- French size = 3 × diameter in mm (e.g., 24 Fr = 8 mm diameter)
- Hopkins rod-lens system = more glass than air → brighter image = revolution in endourology
- 30° telescope = most used for cystoscopy; 0° = urethroscopy
- Bipolar TURP uses saline; monopolar uses glycine/sorbitol → risk of dilutional hyponatremia (TURP syndrome)
- Semirigid URS sizing: First number = tip Fr, second = shaft Fr (e.g., 7/8.5)
- Flexible ureteroscope deflects up to 290° in a single plane
- Obturator is needed for sheaths without an atraumatic beak (VIU, resectoscope sheath); not needed if beak is present (cystoscope sheath)
- Resection rate: ~1 g prostate/min; monopolar TURP max duration = 1 hour
- Ellik evacuator is used to wash out chips after TURP
- Cystoscope components mnemonic = TOBS (Telescope - Obturator - Bridge - Sheath)
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition, pp. 1474, 1550
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Edition, pp. 799-801
- Campbell-Walsh-Wein Urology, Percutaneous Nephrolithotomy sections
- BESDATA Ureteroscope Guide (clinical classification)
- Karl Storz & Richard Wolf instrument catalogs
This is a shared conversation. Sign in to Orris to start your own chat.