50 year old male patient complaint of pain in right hypochondriac region since 8 days K/c/o dm since 2 years
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
right hypochondriac pain diabetic patient differential diagnosis management 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a comprehensive clinical answer.
Clinical Assessment: 50-Year-Old Male, Right Hypochondriac Pain x 8 Days, Known DM x 2 Years
Anatomical Structures in the Right Hypochondrium
The right hypochondriac region contains: gallbladder, right lobe of liver, hepatic flexure of colon, right kidney (upper pole), right adrenal, duodenum (1st part), and the right lower lung/pleura above.
Differential Diagnosis
MOST LIKELY (Top Priority in a Diabetic Male)
1. Acute / Subacute Cholecystitis (Most probable)
- 8 days of RHC pain in a middle-aged male fits perfectly
- DM is a well-established risk factor for complicated cholecystitis including gangrenous and emphysematous forms
- Classic triad: RUQ pain + fever + leukocytosis
- Pain radiates to right scapula/shoulder; Murphy's sign positive
- Nausea, vomiting common
- Jaundice in <50% of cases (mild if present, <5 mg/dL bilirubin)
"The triad of sudden onset of RUQ tenderness, fever, and leukocytosis is highly suggestive." - Harrison's Principles of Internal Medicine 22E, p. 2775
2. Emphysematous Cholecystitis (Must not miss - DM-specific emergency)
- Diabetes mellitus is the primary risk factor, along with elderly men
- Caused by gas-forming organisms: Clostridium perfringens/welchii, E. coli, Klebsiella
- Clinically indistinguishable from regular cholecystitis - but much more dangerous
- Complications: gangrene, perforation, sepsis, MODS
- Diagnosed by CT or plain X-ray (gas in GB wall)
- Requires emergency laparoscopic cholecystectomy + broad-spectrum antibiotics
"Diabetes mellitus has been cited as a risk factor. Gangrene and perforation commonly complicate the course." - Sleisenger & Fordtran's GI and Liver Disease, p. 1045
3. Biliary Colic (Cholelithiasis)
- Gallstones are the most common cause of RHC pain overall
- Cramping/colicky pain in RHC, may radiate to right back or shoulder
- Typically episodic; no fever if uncomplicated
- DM patients have higher risk of gallstone formation
4. Acute Cholangitis
- Charcot's triad: RUQ pain + fever/chills + jaundice
- Results from CBD obstruction (usually stone)
- More serious - requires urgent ERCP + antibiotics
5. Gallstone Pancreatitis
- Pain radiates to back; elevated serum lipase/amylase
- DM patients are predisposed
- Note: Glucose >200 mg/dL is part of the Ranson criteria (severity scoring)
IMPORTANT DIFFERENTIALS
| Condition | Key Feature |
|---|---|
| Pyogenic Liver Abscess | Swinging fever, rigors, tender hepatomegaly; DM is a risk factor |
| Hepatitis (viral/alcoholic) | Elevated transaminases, jaundice, tender liver |
| Perforated Duodenal Ulcer | Sudden excruciating pain, guarding; rigidity greater in RHC |
| Right Lower Lobe Pneumonia | Pain referred to RHC; always examine chest! |
| Right-sided Pyelonephritis | Costovertebral angle tenderness; dysuria; DM predisposes |
| Diabetic Ketoacidosis (DKA) | Abdominal pain can be the presenting feature of DKA itself - check glucose, ketones |
| Subphrenic Abscess | High fever, raised diaphragm on X-ray; may follow upper GI pathology |
| Carcinoma of Hepatic Flexure | Weight loss, change in bowel habits, occult blood; lump may be palpable |
| Fitz-Hugh-Curtis Syndrome | Perihepatitis in women (less relevant here) |
Why DM Makes This Case Special
Diabetic patients with RHC pain deserve extra vigilance because:
- Atypical presentation - autonomic neuropathy may blunt pain and fever, masking severity
- Higher risk of complicated cholecystitis - gangrenous, emphysematous, acalculous forms
- DKA can itself cause abdominal pain - always check blood glucose
- Impaired immune response - infections progress faster; organisms include unusual/anaerobic bacteria
- Mesenteric ischemia - DM-related vascular disease increases risk
- Acalculous cholecystitis - DM is a recognized risk factor even without stones
Investigations to Order
Bedside / Immediate
- Blood glucose (rule out DKA, assess glycemic control)
- Urine ketones
- Urine routine/microscopy (pyelonephritis)
Blood Work
| Test | Why |
|---|---|
| CBC with differential | Leukocytosis (10,000-15,000 with left shift in cholecystitis) |
| LFTs (AST, ALT, ALP, GGT, bilirubin) | Hepatitis, cholestasis |
| Serum amylase + lipase | Rule out pancreatitis |
| Blood urea, creatinine, electrolytes | Renal function; electrolyte balance |
| HbA1c | Assess long-term glycemic control |
| Blood culture x 2 | If fever - sepsis screen |
| Serum albumin | Nutritional/liver status |
Imaging
| Investigation | Priority |
|---|---|
| Ultrasound abdomen (RUQ) | First-line - detects gallstones in 90-95%, GB wall thickening, pericholecystic fluid, CBD dilation; Murphy's sign on USG |
| CT abdomen (contrast) | If USG inconclusive or to detect emphysematous cholecystitis, abscess, perforation |
| Chest X-ray (PA) | Rule out right lower lobe pneumonia, free air under diaphragm |
| Plain X-ray abdomen | May show gallstones (10-15% are radio-opaque), gas in GB wall (emphysematous) |
Special
- HIDA (hepatobiliary iminodiacetic acid) scan: if USG negative but clinical suspicion high
- ERCP: if CBD stone suspected (choledocholithiasis or cholangitis)
Management Approach
Initial Stabilization
- IV access + IV fluids (correct dehydration, electrolytes)
- NPO (nil per os)
- Strict blood glucose monitoring + insulin sliding scale (DM control is essential)
- Analgesia: IV NSAIDs (diclofenac 75 mg) or opioids (morphine/tramadol) for pain relief
- Antiemetics as needed
If Acute Cholecystitis Confirmed
IV Antibiotics (bile culture organisms: E. coli, Klebsiella, Streptococcus, Clostridium):
- Mild-moderate: IV Cefazolin or Amoxicillin-Clavulanate
- Severe/DM: IV Piperacillin-Tazobactam or Meropenem + Metronidazole (anaerobic cover)
Surgery:
- Early laparoscopic cholecystectomy (within 72 hours) is the preferred definitive treatment
- Meta-analyses show early surgery has shorter total hospital stay (9.6 days vs 17.8 days), lower mortality, and prevents recurrence
"Early operation is preferable because the total length of hospitalization and costs are reduced, morbidity is less, and deaths related to progressive acute cholecystitis are prevented." - Sleisenger & Fordtran's GI and Liver Disease
If unfit for surgery (high-risk patient): Percutaneous cholecystostomy (drainage) as a bridge.
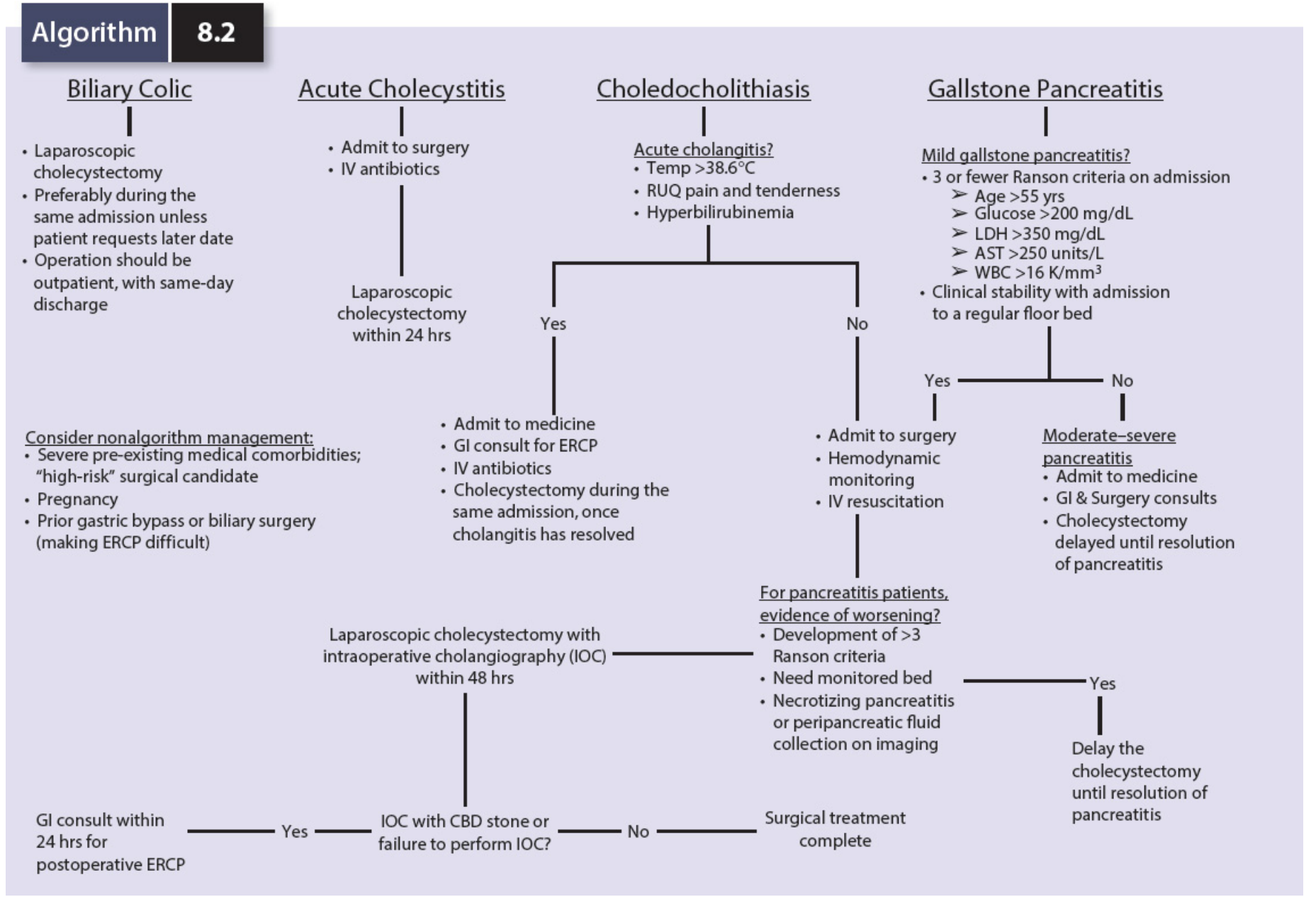
Biliary Infection Algorithm (Mulholland & Greenfield's Surgery)
Key Clinical Pearls for This Patient
- 8 days of pain - this is subacute. The gallbladder may have walled off, or the patient may be masking severity due to diabetic neuropathy.
- Always check glucose first - DKA can present with abdominal pain and mimic an acute abdomen.
- RUQ ultrasound is mandatory - it is the gold standard first-line imaging.
- Murphy's sign on examination (inspiratory arrest during subcostal palpation) strongly supports cholecystitis.
- Emphysematous cholecystitis is a surgical emergency - if CT shows gas in the GB wall, operate urgently.
- Gangrene of the gallbladder is more common in DM due to vasculitis and ischemia of the GB wall.
- DM patients should have blood glucose tightly controlled perioperatively.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Sleisenger & Fordtran's Gastrointestinal and Liver Disease, S. Das Manual on Clinical Surgery 13th Ed, Mulholland & Greenfield's Surgery 7E, Tintinalli's Emergency Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.