Orthopedics insteuments
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
orthopedic surgical instruments overview
Finding Sources
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of common orthopedic surgical instruments, organized by category and function:
Orthopedic Surgical Instruments — Overview
1. Cutting Instruments
These instruments are used to cut, shape, or remove bone and soft tissue.
| Instrument | Description & Use |
|---|---|
| Osteotome | A chisel-like instrument used to cut or shape bone. Available in straight and curved designs. Used with a mallet. |
| Bone Saw (Oscillating/Reciprocating) | Power saw used for precise bone cuts, e.g., in joint arthroplasty (TKA, THA), amputations, and osteotomies. |
| Rongeur | Hinged, jaw-like instrument for nibbling/removing small pieces of bone or cartilage (e.g., in spinal surgery, joint debridement). |
| Bone Curette | Spoon-shaped instrument to scoop out bone or soft tissue from cavities; used in bone grafting and tumor excision. |
| Mallet | Heavy hammer used with osteotomes and chisels to deliver controlled force to bone. |
| Gigli Saw | Flexible wire saw used for cutting bone in tight spaces (e.g., amputation, pelvic osteotomy). |
| Periosteal Elevator | Flat-edged instrument to strip periosteum from bone surface before cutting or fixation. |

2. Holding & Grasping Instruments
Used to grip, hold, or stabilize bone fragments and tissue.
| Instrument | Description & Use |
|---|---|
| Bone-Holding Forceps | Self-retaining or handheld forceps used to grip bone fragments during reduction and fixation. |
| Reduction Forceps (Pointed / Ball-Spike Clamps) | Used to achieve and temporarily maintain fracture reduction before definitive fixation (e.g., in ORIF). |
| Towel Clamps | Used to hold drapes in place and occasionally to grasp bone. |
| Tissue Forceps (Adson, Allis) | For grasping soft tissue during exposure. |
3. Retractors
Used to retract soft tissue and maintain surgical exposure.
| Instrument | Description & Use |
|---|---|
| Hohmann Retractor | Angled retractor placed around bone to retract muscle; widely used in hip, knee, and fracture surgery. |
| Langenbeck Retractor | Handheld retractor for general soft tissue retraction. |
| Cobra Retractor | Curved retractor used around the acetabulum or femur in hip arthroplasty. |
| Taylor Retractor | Self-retaining spinal retractor for posterior approach surgeries. |
| Gelpi / Weitlaner Retractor | Self-retaining retractors for smaller incisions. |
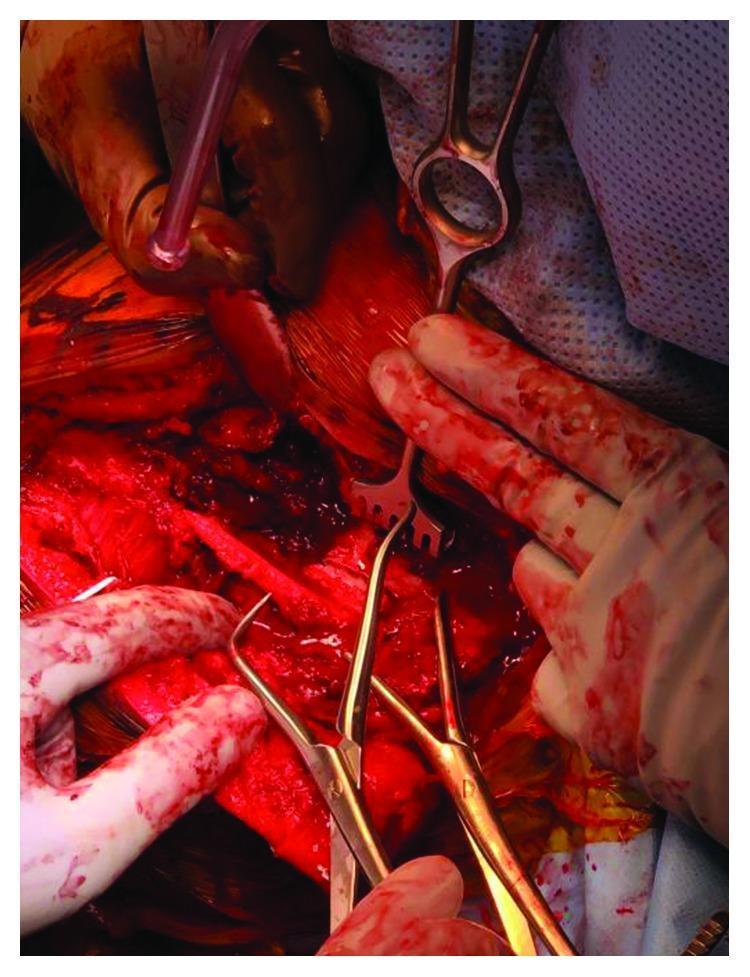
| Fork Retractor | Multi-tined retractor for bone exposure (as seen in the image above). |
⚠️ Note: Aberrant retractor placement is a recognized cause of neurovascular injury — e.g., peroneal nerve palsy in TKA and obturator vessel damage in hip arthroplasty. — Miller's Review of Orthopaedics, 9th Ed.
4. Drilling & Fixation Instruments
Used for creating holes in bone and applying implants.
| Instrument | Description & Use |
|---|---|
| Power Drill | Used to create drill holes for screws, K-wires, and implant anchors. Small-diameter drills (3.2–4.0 mm) used for core decompression in AVN. |
| Drill Bits | Various sizes; must match screw diameter. Metal debris from drill bits can contribute to polyethylene wear in joint replacements. |
| Cannulated Drill System | Drilled over a guidewire for percutaneous and minimally invasive fixation. |
| Kirschner Wire (K-Wire) Driver | Drives thin K-wires for temporary or definitive fixation (e.g., CRPP for distal radius, pediatric fractures). |
| Tap | Creates threads in a drill hole before screw insertion. |
| Screwdriver | Hex or cruciate drives for insertion of cortical, cancellous, or locking screws. |
| Bone Tamp | Curved instrument used to impact bone graft or reposition bone fragments (shown below). |
5. Implant Removal Instruments
| Instrument | Description & Use |
|---|---|
| Shoulder Hook | Long slender instrument with a curved hook tip used to lever implanted plates off bone. |
| Curved Bone Tamp | Used with a mallet to dislodge implants or bone grafts that have integrated with fibrous/osseous tissue. |
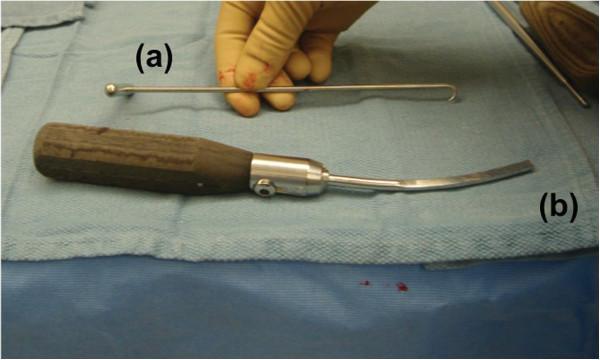
(b) Curved bone tamp — wooden handle with curved flat metallic blade
6. Measuring & Alignment Instruments
| Instrument | Description & Use |
|---|---|
| Caliper / Depth Gauge | Measures screw length after drilling. |
| Goniometer | Measures joint angles, used for alignment checks. |
| Cutting Jigs / Alignment Guides | Templates for precise bone cuts in arthroplasty (e.g., four-in-one cutting jig in TKA). Malposition leads to complications like femoral notching. |
| Trial Components | Temporary implant replicas used intraoperatively to verify sizing before definitive implant insertion. |
7. Specialty Instruments by Procedure
| Procedure | Key Instruments |
|---|---|
| Total Hip Arthroplasty (THA) | Cobra/Hohmann retractors, acetabular reamers, broaches, cup inserter, femoral rasp |
| Total Knee Arthroplasty (TKA) | Alignment rods, 4-in-1 cutting jig, tibial baseplate trial, gap balancer |
| Spinal Surgery | Pedicle awl, pedicle probe, nerve root retractor (Taylor), Kerrison rongeur |
| Fracture Fixation (ORIF) | Reduction clamps, lag screws, dynamic compression plate, locking plate system |
| Arthroscopy | Arthroscope, shaver, probe hook, basket punch forceps, cannulas |
Summary Classification
Orthopedic Instruments
├── Cutting → Osteotome, Saw, Rongeur, Curette, Gigli saw
├── Holding → Bone forceps, Reduction clamps
├── Retractors → Hohmann, Cobra, Langenbeck, Gelpi
├── Drilling/Fixation → Drill, K-wire driver, Tap, Screwdriver
├── Measuring → Caliper, Goniometer, Cutting jigs
└── Implant-specific → Reamers, Broaches, Rasps, Trials
Sources: Miller's Review of Orthopaedics, 9th Ed. | Rockwood and Green's Fractures in Adults, 10th Ed.
Dhs plate
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
DHS dynamic hip screw plate fixation intertrochanteric fracture
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of the DHS (Dynamic Hip Screw) Plate:
DHS Plate (Dynamic Hip Screw / Sliding Hip Screw)
What is it?
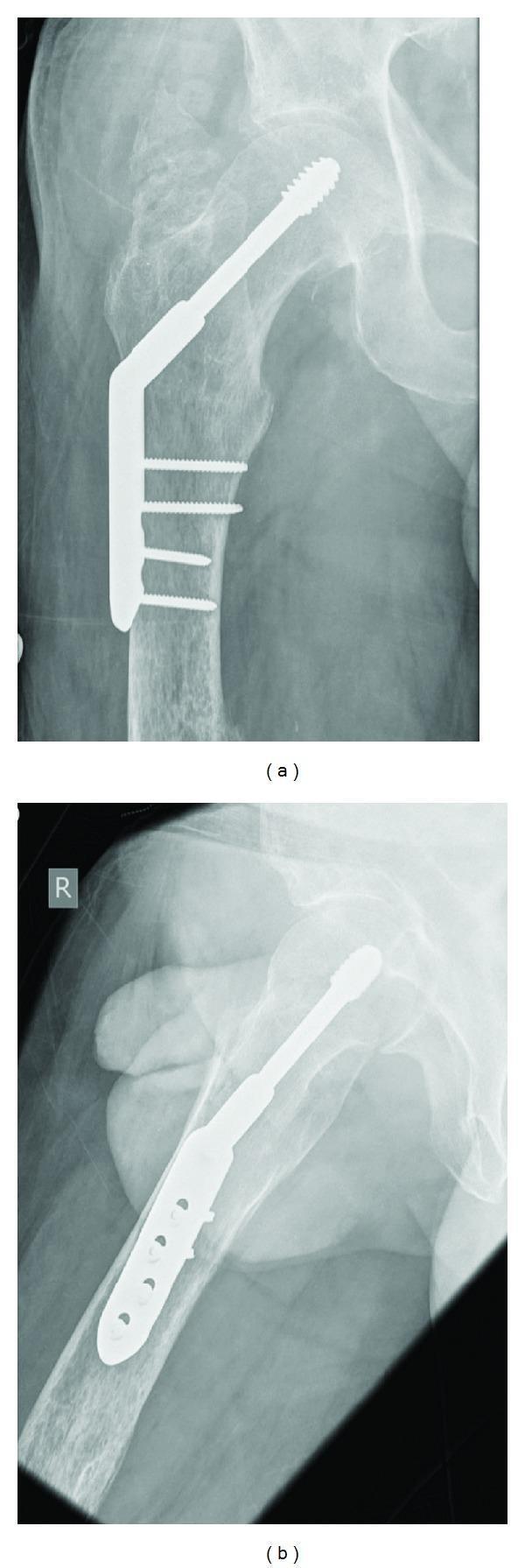
The DHS plate — also called the Sliding Hip Screw or Compression Hip Screw (name varies by manufacturer) — is an extramedullary implant used to fix proximal femoral fractures. It was first developed in the 1950s and remains the gold standard for stable trochanteric (A1) hip fractures.
Components
The DHS construct has three main parts:
| Component | Description |
|---|---|
| Lag Screw | Large-diameter cannulated screw inserted up the femoral neck into the femoral head. The serrated/threaded tip grips bone in the femoral head. |
| Barrel/Plate | Angled side plate with a cylindrical barrel at the top. The lag screw slides freely inside the barrel — this is the key "dynamic" feature. |
| Cortical Screws | 3–4 screws fix the side plate to the lateral femoral shaft. |
The barrel angle is typically 135° or 130° relative to the plate shaft. A lesser angle risks lag screw jamming; a higher angle causes a superior screw position with increased cutout risk.
Mechanism of Action (Why "Dynamic"?)
Unlike older fixed/static nail-plates (Jewett, Thornton, McLaughlin plates) where fracture collapse caused the screw to penetrate the hip joint, the DHS allows:
- The lag screw to slide within the barrel as the fracture collapses
- Controlled dynamic compression at the fracture site during weight-bearing
- Fracture healing through impaction rather than fixation failure
Indications
| Indication | Notes |
|---|---|
| Stable intertrochanteric fractures (AO/OTA A1) | Primary indication — gold standard |
| Basicervical femoral neck fractures | Some surgeons prefer DHS |
| Undisplaced intracapsular fractures (Garden 1 & 2) | Used in younger patients (<60 yrs) |
| Subtrochanteric osteotomy fixation | With appropriate plate angle |
Not recommended for:
- Unstable A2/A3 fractures → prefer cephalomedullary nail
- Reversed/transverse (A3) fractures → the DHS cannot allow longitudinal sliding; Medoff plate or nail preferred
Surgical Technique (Step-by-Step)
- Patient supine on fracture table, traction applied
- Fracture reduced under image intensifier (AP + lateral views)
- 5–7 cm lateral incision just distal to the greater trochanter
- Divide fascia lata, reflect or split vastus lateralis to expose lateral femur
- Insert guidewire using angle guide (135° most common)
- Position: central-to-low on AP, central on lateral
- Measure guidewire depth → select lag screw length
- Tip should be 5 mm from subchondral bone of femoral head
- Not too far from joint → increases cutout risk
- Tap femoral head bone (prevents rotation of head during screw insertion)
- Insert lag screw — prevent femoral head rotation (place finger on anterior femoral neck or use anti-rotation pin)
- Attach side plate to femur; insert cortical screws (usually 4-hole plate)
- Ensure lateral end of lag screw is 5 mm from lateral side of barrel so initial sliding is within the barrel (avoids protrusion into soft tissue)
- Close fascia lata → skin with absorbable subcuticular sutures + pressure dressing

DHS X-ray Appearance

Modifications of the Sliding Hip Screw
| Modification | Indication | Feature |
|---|---|---|
| Lateral Trochanteric Stabilizing Plate | Disrupted lateral femoral wall (A2 fractures) | Clips to side of standard DHS; resists femoral medialization; reconstructs greater trochanter |
| Medoff Plate | Reversed/transverse A3 fractures | Two interdigitating femoral plates allowing two-way sliding (along lag screw AND along femoral axis) |
Complications
| Complication | Cause |
|---|---|
| Screw cutout (most common) | Poor lag screw position (superior/peripheral placement); tip >10 mm from joint; varus malreduction |
| Screw jamming | Lag screw at too-low angle; screw tip too far from barrel end |
| Lateral protrusion of lag screw | Excessive fracture collapse; screw too far lateral in barrel initially |
| Femoral medialization | Unstable fractures without stabilizing plate |
| Infection / wound dehiscence | Higher risk in obese patients |
| Fixation failure / non-union | Unstable fracture pattern treated with DHS instead of nail |
DHS vs. Cephalomedullary Nail
| Feature | DHS (Sliding Hip Screw) | Cephalomedullary Nail |
|---|---|---|
| Best for | Stable A1 fractures | Unstable A2, A3, subtrochanteric |
| Implant position | Extramedullary (lateral plate) | Intramedullary |
| Load sharing | No (load bypass) | Yes |
| Reoperation rate | Higher for unstable fractures | Lower for unstable fractures |
| Surgical access | Lateral incision, more exposure | Smaller, minimally invasive |
Sources: Rockwood and Green's Fractures in Adults, 10th Ed., 2025 | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.