Teach me oxygen dissociation curve from basic to advance and clinical
Reading File
Finding Sources
Finding Sources
Searching PubMed
"oxygen dissociation curve" hemoglobin physiology
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the material needed for a comprehensive, well-illustrated answer. Let me compose it.
The Oxygen Dissociation Curve: Basic to Advanced to Clinical
1. Why Oxygen Needs a Carrier
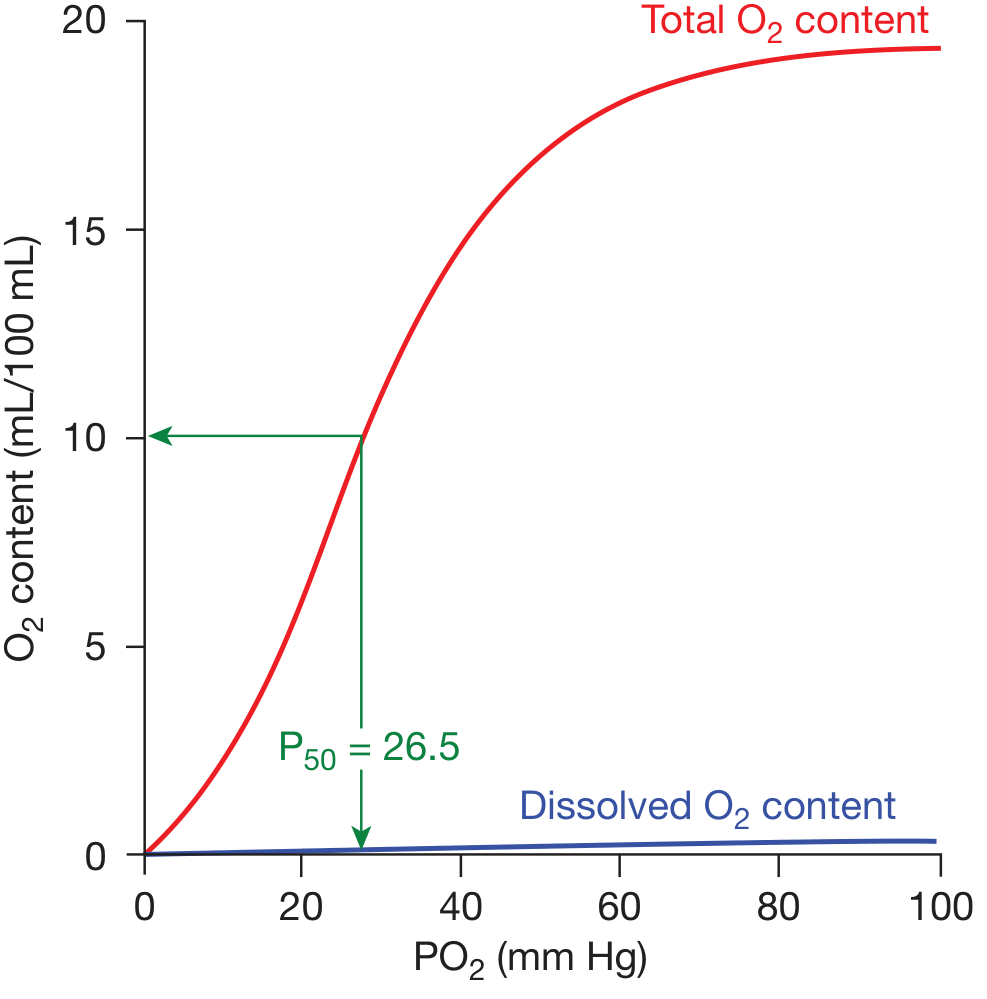
Oxygen is poorly soluble in plasma. At a normal arterial PO₂ of 100 mm Hg, dissolved O₂ contributes only ~0.3 mL/100 mL blood - completely inadequate for tissue demands. Hemoglobin (Hb) solves this: at 15 g/dL Hb, blood can carry ~20 mL O₂/100 mL blood. The oxygen dissociation curve (ODC) describes the relationship between PO₂ and the amount of O₂ bound to Hb (or % saturation).
2. The Standard ODC - Shape and Key Points
Standard conditions: pH 7.40, temperature 37°C, atmospheric pressure 760 mm Hg
The curve is sigmoidal (S-shaped), not hyperbolic. This shape is physiologically critical.
Key Landmarks
| PO₂ (mm Hg) | SpO₂ | Physiological site |
|---|---|---|
| 100 | ~97-98% | Arterial blood / lungs |
| 60 | ~90% | "Cliff edge" - lower is dangerous |
| 40 | ~75% | Mixed venous blood at rest |
| 26.5 | 50% | P50 - standard reference point |
| 20-10 | 35-20% | Active tissues / exercising muscle |
The P50 is the PO₂ at which 50% of hemoglobin is saturated. Normal adult P50 = 26.5 mm Hg. Changes in P50 reflect shifts in oxygen affinity.
Why Sigmoidal, Not Hyperbolic?
This is where biochemistry meets physiology. Hemoglobin is a tetramer (α₂β₂) with cooperative binding:
- Hb starts in the T (tense/deoxy) conformation - low O₂ affinity
- As the first O₂ binds, it induces a conformational change that makes the next heme group bind O₂ more easily (T → R transition)
- The R (relaxed/oxy) conformation has ~300× higher O₂ affinity than T
- The net effect: the last O₂ bound is held ~300× more tightly than the first
This cooperative binding makes the curve sigmoid. In contrast, myoglobin is a monomer with no cooperativity - its curve is hyperbolic (like a rectangular hyperbola), with a P50 of ~1 mm Hg. It holds O₂ tightly and will not release it at tissue PO₂ levels - perfect for an O₂ storage molecule in muscle, useless as a transport molecule.
3. The Two Critical Zones of the Curve
Upper flat portion (PO₂ 60-100 mm Hg):
- Small drops in PO₂ produce minimal drops in saturation
- This is the "safety buffer" - lung disease or altitude can drop alveolar PO₂ significantly before SpO₂ falls below 90%
- The body can tolerate PaO₂ declining from 100 → 60 mm Hg with only a ~8% drop in saturation
Steep portion (PO₂ 20-60 mm Hg):
- Small drops in PO₂ release large amounts of O₂ to tissues
- This is the "working zone" - tissues operate here
- Maintains tissue O₂ tension high enough to drive diffusion from capillary to mitochondria
This is why Fishman's Pulmonary Diseases describes the steep portion as a "slippery slope" that clinicians should always keep in mind when managing respiratory insufficiency.
4. Factors That Shift the ODC
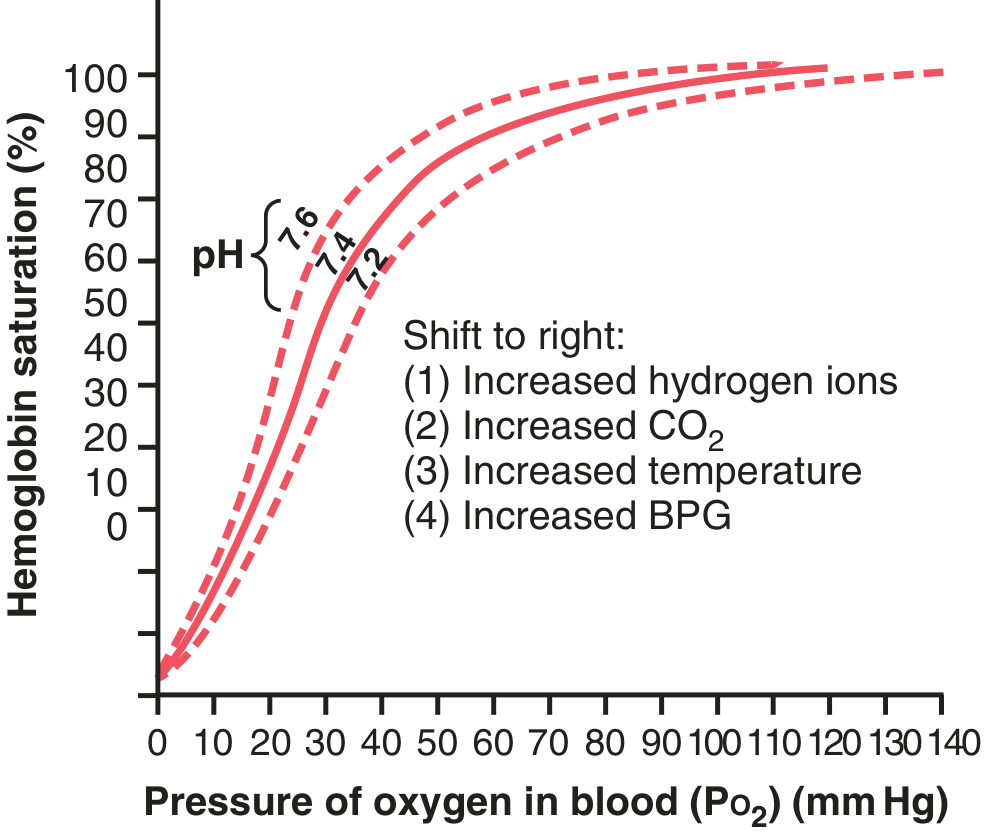
The mnemonic "CADET face Right" captures right-shifting factors:
CO₂ ↑, Acid ↑ (pH ↓), 2,3-DPG ↑, Exercise/Temperature ↑ → Right shift
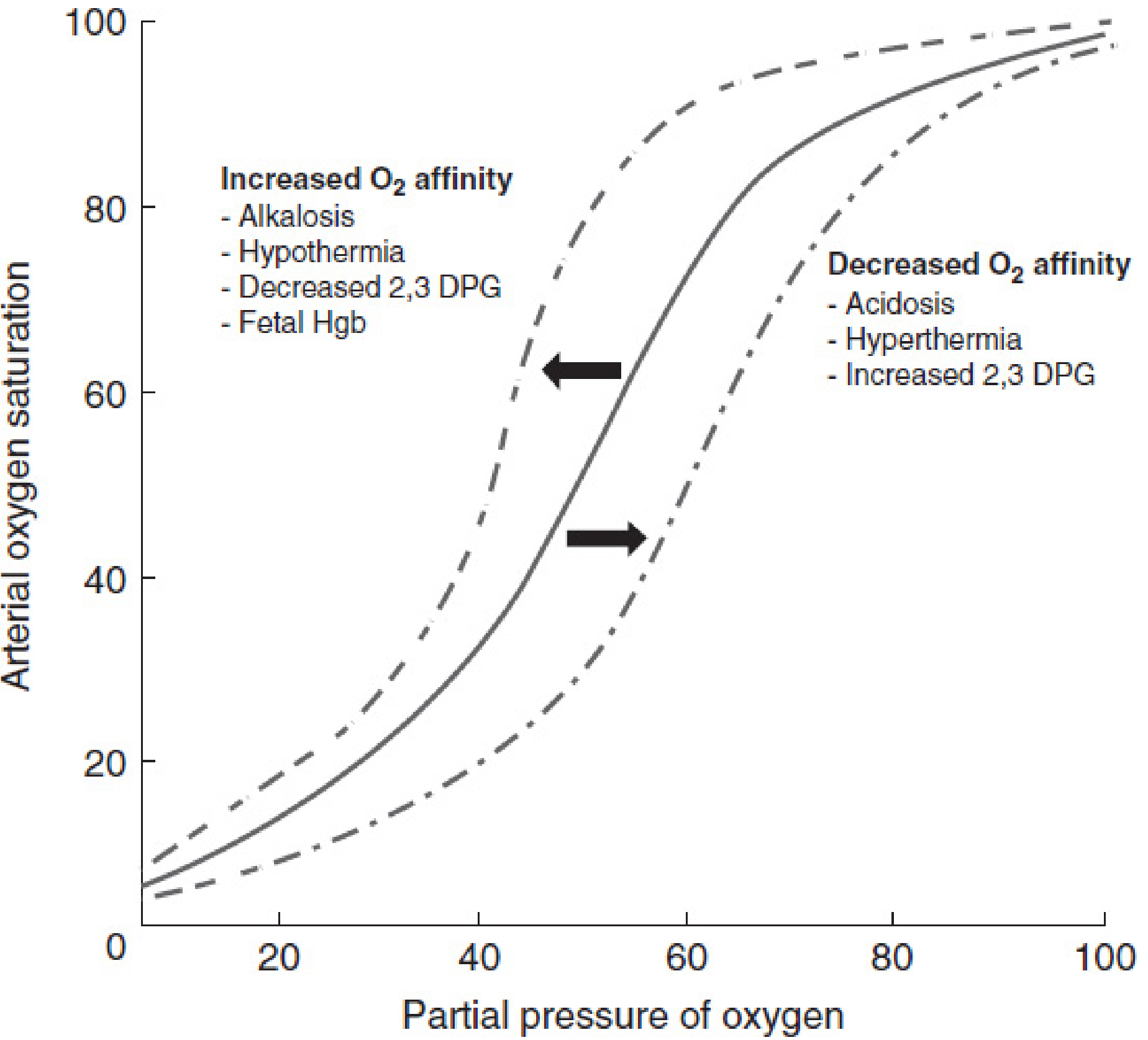
| Factor | Right Shift (↓ affinity, ↑ P50) | Left Shift (↑ affinity, ↓ P50) |
|---|---|---|
| pH | Decreased (acidosis) | Increased (alkalosis) |
| CO₂ | Increased | Decreased |
| Temperature | Increased (hyperthermia) | Decreased (hypothermia) |
| 2,3-BPG | Increased | Decreased |
| Hemoglobin type | HbS (slightly) | HbF (fetal Hb), HbCO, MetHb |
| CO | - | Left shift (see below) |
Right Shift = Easier O₂ Delivery to Tissues
Hb gives up O₂ more readily. P50 increases. Good in exercising muscle, harmful in the lungs (incomplete loading if severe).
Left Shift = Tighter O₂ Binding
Hb loads O₂ more easily in lungs but releases it less readily to tissues. Good in the placenta (fetal Hb), harmful when it means tissues don't get O₂.
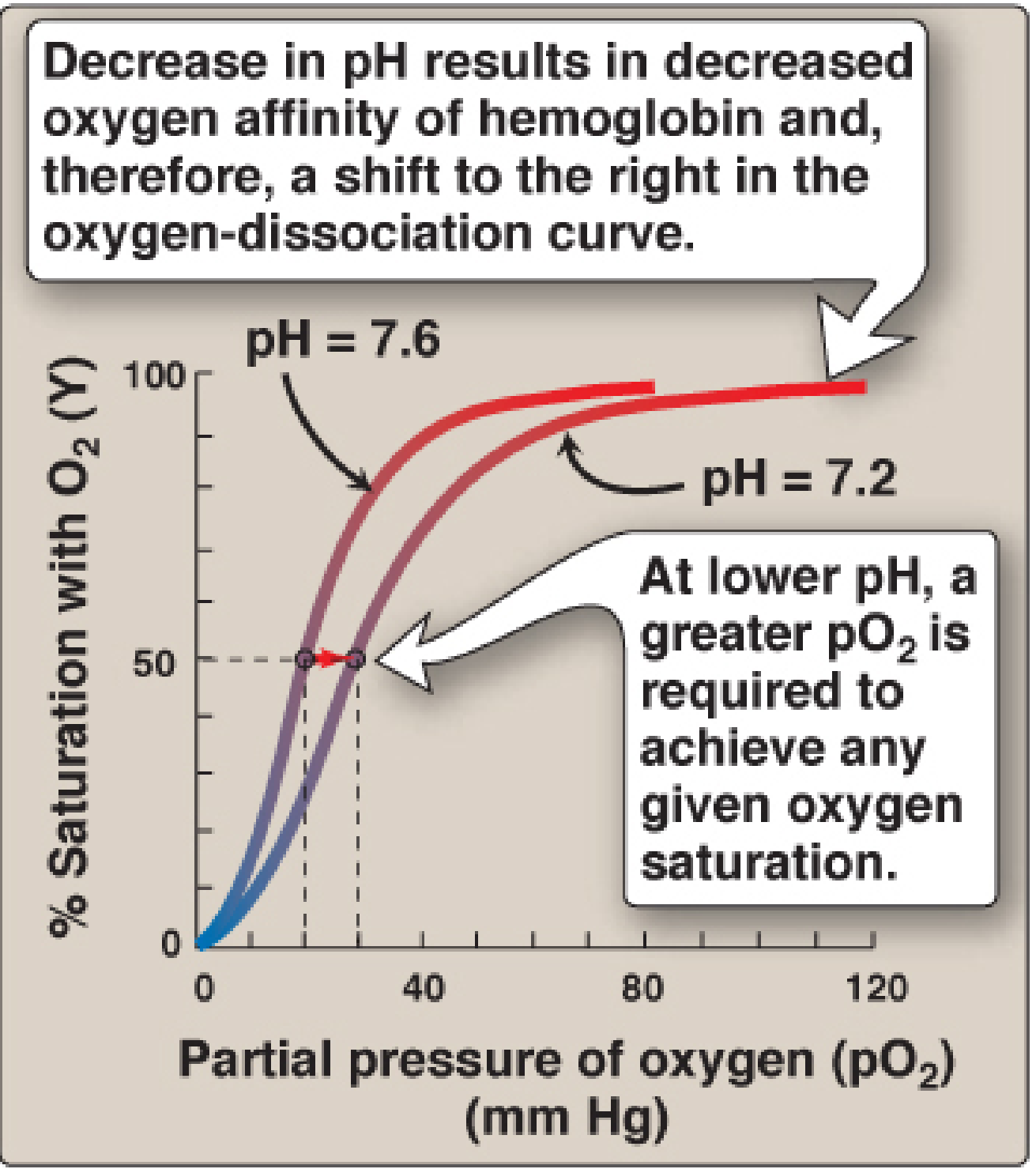
5. The Bohr Effect (pH and CO₂)
The Bohr effect is the shift caused by CO₂ and H⁺ - a beautifully efficient physiological mechanism.
In peripheral tissues:
- Cells produce CO₂ → carbonic anhydrase converts it: CO₂ + H₂O → H₂CO₃ → HCO₃⁻ + H⁺
- Rising CO₂ and falling pH shift the ODC right → Hb unloads O₂ to the tissues that need it most
In the lungs:
- CO₂ diffuses out → pH rises → curve shifts left → Hb loads O₂ more efficiently
The molecular mechanism: deoxyhemoglobin has a greater affinity for H⁺ than oxyhemoglobin. Specific histidine residues (particularly His-146 of the β-chain) form salt bridges when protonated, stabilizing the T conformation. This is represented as:
HbO₂ + H⁺ ⇌ HbH⁺ + O₂
The Bohr effect also explains why CO₂ itself (independent of its pH effect) shifts the curve - CO₂ binds to the N-terminal amino groups of Hb chains forming carbaminohemoglobin, stabilizing the T (deoxy) conformation directly.
6. The 2,3-Bisphosphoglycerate (2,3-BPG) Effect
2,3-BPG (also called 2,3-DPG) is an intermediate of glycolysis produced only in RBCs by the Rapoport-Luebering shunt.
Mechanism:
- 2,3-BPG binds in the central cavity formed by the two β-globin chains of deoxyhemoglobin (T form)
- The cavity contains positively charged amino acids (Val-1, His-2, Lys-82, His-143 of β chains) that form ionic bonds with 2,3-BPG's negatively charged phosphate groups
- Oxygenation (R conformation) narrows this cavity → 2,3-BPG is expelled
- By preferentially stabilizing the T form, 2,3-BPG shifts the ODC right, lowering O₂ affinity and promoting O₂ release
Clinical relevance of 2,3-BPG:
- Chronic hypoxia (COPD, high altitude): 2,3-BPG levels rise → rightward shift → more O₂ delivered per unit PO₂ drop - an adaptive compensation
- Chronic anemia: Same adaptation - elevated 2,3-BPG helps squeeze more O₂ from fewer RBCs
- Stored blood (transfusion medicine): After 1-2 weeks of storage, RBC 2,3-BPG is nearly depleted → ODC shifts left → transfused RBCs bind O₂ but don't release it well for ~24 hours until 2,3-BPG regenerates (clinically significant in massive transfusion)
7. Special Hemoglobins and Their Curves
Fetal Hemoglobin (HbF - α₂γ₂)
HbF has γ-chains instead of β-chains. The γ-chain has a serine at position 143 (vs. histidine in the β-chain), which interacts less strongly with 2,3-BPG. Since HbF binds 2,3-BPG less avidly, it remains in the R (oxy) conformation more readily, giving it a higher O₂ affinity (P50 ~19 mm Hg vs adult 26.5).
Clinical significance: In the placenta, maternal arterial blood PO₂ (~100 mm Hg) and intervillous PO₂ (~40 mm Hg) would be insufficient to transfer O₂ if fetal blood didn't have a left-shifted curve. HbF loads O₂ even at low PO₂, then releases it to fetal tissues (even lower PO₂). This double gradient drives O₂ from mother to fetus.
During the postnatal transition: rising 2,3-BPG and mild acidosis shift the neonatal curve rightward, facilitating tissue O₂ delivery as metabolic demands increase.
Carboxyhemoglobin (HbCO) - CO Poisoning
Carbon monoxide binds hemoglobin with 240× the affinity of O₂. Two effects:
- Reduces O₂-carrying capacity - binding sites occupied by CO
- Left-shifts the ODC for remaining oxygenated Hb - the remaining Hb holds O₂ tighter and won't release it to tissues (Haldane effect)
- CO has even higher affinity for HbF - fetuses and neonates are at particular risk
HbCO clinical levels:
| HbCO (%) | Clinical findings |
|---|---|
| 0.4-2% | Normal nonsmoker |
| 2-6% | Normal smoker |
| 10-20% | Dyspnea on exertion |
| 20-50% | Headache, lethargy, loss of consciousness |
| >50% | Coma and death |
Treatment with 100% O₂ competitively displaces CO (half-life of HbCO: 5 hrs on room air, 60-90 min on 100% O₂, 20-30 min in hyperbaric O₂).
Methemoglobin (MetHb)
Methemoglobin contains Fe³⁺ (oxidized iron) instead of Fe²⁺. Fe³⁺ cannot bind O₂. It also causes a left-shift of the remaining normal Hb - same tissue hypoxia mechanism as CO, but without CO's cellular toxicity. Treatment: methylene blue (activates NADPH-methemoglobin reductase).
Hemoglobin Variants with Altered Affinity
- High-affinity Hbs (Hb Chesapeake, Yakima, Rainier): Left-shifted ODC, low P50. The tissue hypoxia drives compensatory erythrocytosis (polycythemia). These are detected by measuring the P50 directly.
- Low-affinity Hbs (Hb Kansas, Beth Israel): Right-shifted ODC. Presents with cyanosis and anemia because Hb unloads O₂ at high PO₂ (incomplete loading in lung) and appears cyanotic even though O₂ delivery may be adequate.
8. Clinical Applications
A. The "Safe" SpO₂ Threshold of 90% (PaO₂ ~60 mm Hg)
The flat top of the curve gives a false sense of security. Once PaO₂ drops below 60 mm Hg, you are on the steep portion - further small drops cause precipitous desaturation. This is the physiological basis for keeping target PaO₂ ≥ 60 mm Hg or SpO₂ ≥ 90% in clinical practice.
B. Pulse Oximetry Limitations
SpO₂ measures O₂ saturation, not PaO₂. The flat part of the curve means:
- A patient can have SpO₂ 98% with PaO₂ of 80 or 150 mm Hg - very different clinical states
- SpO₂ cannot distinguish HbCO from oxyHb (both absorb similarly at 660 nm) → normal SpO₂ in CO poisoning despite severe tissue hypoxia
- Co-oximetry (measures all Hb species) is needed in suspected CO or MetHb
C. Exercise Physiology
During heavy exercise, active muscle becomes:
- Hot (temperature ↑)
- Acidic (lactate, CO₂ ↑, pH ↓)
- 2,3-BPG increases
All three shift the ODC right simultaneously - a synergistic adaptation that delivers up to 3× more O₂ to exercising tissue than at rest.
D. High Altitude Adaptation
Acute (hours to days): Hyperventilation → respiratory alkalosis → left shift (bad, reduces O₂ delivery). This is the initial maladaptation.
Chronic (days to weeks): 2,3-BPG production increases → right shift compensates, restoring (and surpassing) normal O₂ delivery. Polycythemia (erythropoietin-driven) also increases total O₂-carrying capacity.
E. Hypothermia and Cardiac Surgery
Hypothermia (e.g., during cardiopulmonary bypass) left-shifts the ODC - Hb holds O₂ tightly. This actually provides some protection during circulatory arrest because tissues consume less O₂ at low temperatures. However, blood gas values must be corrected for temperature (alpha-stat vs pH-stat management).
F. Sepsis and ARDS
Sepsis causes:
- Fever → right shift (compensatory)
- Acidosis → right shift (compensatory)
- Increased 2,3-BPG in chronic states
The net effect is usually a rightward shift, which helps tissue O₂ delivery despite low cardiac output or low Hb. However, if alkalosis is induced (aggressive sodium bicarbonate, over-ventilation), a left shift can reduce tissue O₂ delivery paradoxically.
G. Sickle Cell Disease
HbS slightly right-shifts the ODC (lower O₂ affinity), which alone would be helpful for O₂ delivery. The pathology lies elsewhere - HbS polymerizes when deoxygenated, causing sickling. The ODC shift is a minor consideration compared to the vaso-occlusive and hemolytic mechanisms.
H. Transfusion Triggers
The ODC explains why transfusion triggers focus on hemoglobin concentration (O₂-carrying capacity) rather than just SpO₂:
- A patient with Hb 7 g/dL may have normal SpO₂ (97%) but only ~14 mL O₂/100 mL blood total capacity
- The ODC also explains why transfusing stored (low 2,3-BPG) blood may initially worsen tissue O₂ delivery despite raising Hb concentration
9. Summary: Left vs. Right - Clinical Memory Map
LEFT SHIFT (↑ affinity, ↑ P50 decreases → binds tightly, releases less)
Mnemonic: "COLD FLAB"
Cold (hypothermia)
Low CO₂
Alkalosis (high pH)
Fetal Hb
Low 2,3-BPG
Altitude (acute, via alkalosis)
Blood storage (old blood)
Clinical effect: Hb loads O₂ well, won't release to tissues → tissue hypoxia
RIGHT SHIFT (↓ affinity, ↑ P50 → releases more O₂)
Mnemonic: "ATCH"
Acidosis / ↑ H⁺
Temperature ↑
CO₂ ↑
High 2,3-BPG
Clinical effect: Hb delivers O₂ better to tissues
10. Quick Reference Values
| Parameter | Normal value |
|---|---|
| P50 (adult HbA) | 26.5 mm Hg |
| P50 (fetal HbF) | ~19 mm Hg |
| Arterial PaO₂ | 80-100 mm Hg |
| Arterial SpO₂ | 97-99% |
| Mixed venous PO₂ | ~40 mm Hg |
| Mixed venous SpO₂ | ~75% |
| O₂ extraction at rest | ~25% |
| Maximum O₂ extraction | ~75-80% (in exercise/shock) |
| Dissolved O₂ contribution | 0.003 mL/dL per mm Hg PO₂ |
Recent literature note: A 2025 scoping review (Haller et al., Eur J Clin Pharmacol, PMID 39585422) catalogued how drugs shift the ODC - including volatile anesthetics (reviewed by Kumar et al., 2025, PMID 39991860) - confirming this remains an active clinical research area. No evidence has emerged to overturn the classical physiological principles above.
Sources: Lippincott's Illustrated Reviews: Biochemistry 8e | Guyton & Hall Medical Physiology | Fishman's Pulmonary Diseases | Miller's Anesthesia 10e | Mulholland & Greenfield's Surgery 7e | Quick Compendium of Clinical Pathology 5e
This is a shared conversation. Sign in to Orris to start your own chat.