I and D of Perianal Abscess
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
perianal abscess incision drainage technique anatomy
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a complete summary:
Incision & Drainage of Perianal Abscess
Pathophysiology & Classification
Most perianal abscesses originate from cryptoglandular infection at the dentate line — bacteria infect the anal crypts and spread through the path of least resistance into the perianal soft tissue spaces.
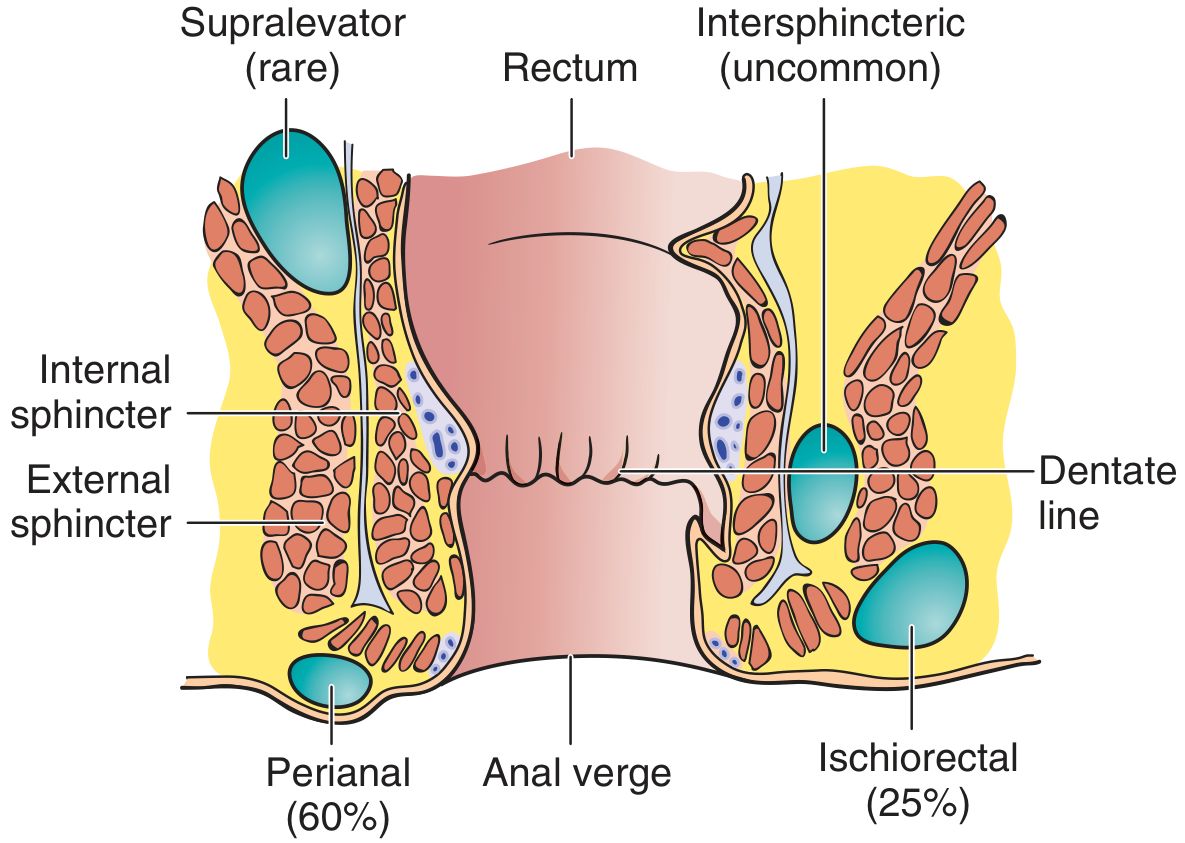
| Location | Incidence | Features |
|---|---|---|
| Perianal (adjacent to anal verge) | 60% | Most common; superficial; amenable to outpatient I&D |
| Ischiorectal (outside sphincters, 2–3 cm from verge) | 25% | Larger, may be bilateral ("horseshoe abscess") |
| Intersphincteric (between internal & external sphincters) | Uncommon | No external swelling; diagnosed on digital exam as fluctuant mass above anorectal ring |
| Supralevator / Pelvirectal | Rare | Must rule out intra-abdominal/pelvic source (appendicitis, diverticulitis, PID) |
Clinical Features
- Pain: Severe, throbbing, progressive perianal pain — worsened by sitting, coughing, sneezing, and straining
- Signs: Swelling, induration, erythema, tenderness near the anus
- Systemic: Fever and leukocytosis in more severe cases
- Microbiology: Mixed infection — anaerobes (B. fragilis), gram-negative enteric bacilli; consider MRSA in endemic areas
- WBC >10 × 10⁹/L in <50% of cases
Imaging: CT sensitivity is only ~77%; MRI is preferred when clinical suspicion is high but CT is non-diagnostic.
Indications for I&D
Nearly every perianal abscess requires I&D — this is the treatment of choice, not antibiotic therapy alone. The only exception is if spontaneous drainage has clearly provided adequate drainage (though loculations must still be assessed manually).
⚠️ Delaying I&D risks necrotizing fasciitis or perineal sepsis (pain + fever + inability to void). This is especially urgent in diabetic, immunocompromised, or steroid-dependent patients.
Contraindications / Special Cases
- Hematologic malignancy (leukemia, lymphoma, granulocytopenia): The infecting organisms differ; some authorities recommend conservative antibiotics ± local radiotherapy. If surgery is needed, do NOT attempt in an outpatient setting — refer.
- Only small, well-defined perianal abscesses without deeper extension are suitable for outpatient I&D. All others (ischiorectal, intersphincteric, supralevator) should be drained in the OR.
Equipment
- 2% lidocaine with epinephrine; 27- or 30-gauge needle
- Hemostats
- No. 11 scalpel blade
- 4×4 gauze
- Penrose drain or iodoform gauze packing (½-inch)
- Suction (for large abscesses)
- Surgical electrocautery (for hemostasis in hyperemic tissue)
- Ives slotted anoscope or Hill-Ferguson rectal retractors
Procedure — Step by Step
Before the Incision
- Anoscopy first (before I&D): With gentle pressure on the abscess, look for pus expressed from an internal opening at the dentate line — this confirms an associated anal fistula. The fistula-in-ano rate with perianal abscess is at least 50%.
- Anesthesia: Local anesthesia (2% lidocaine with epinephrine) is often only marginally effective because the acidic infected tissue resists local anesthetics. Spinal or general anesthesia may be required for larger abscesses.
Incision
- Make a radial incision over the most fluctuant area, directed radially toward the anal canal. This orientation allows easy extension for fistulotomy if a fistula is identified.
- Alternative: excise an ellipse of tissue large enough to admit a finger for cavity exploration and loculation breakdown.
- Another option: cruciate (cross) incision — preferred by some because a simple linear incision risks premature closure without adequate drainage.
- Express all purulence. Break down loculations with a gloved finger or hemostats. Cultures are obtained here if warranted (see below).
Irrigation & Drainage
- Irrigate the abscess cavity.
- Place a Penrose drain loosely in the cavity, sutured at the skin edge — remove at 24–48 hours (Penrose drain does not adhere, making removal painless).
- Alternative: pack with ½-inch iodoform gauze; replace at 48-hour intervals until granulation tissue appears (usually 4–6 days).
Temporizing Measure (if OR unavailable)
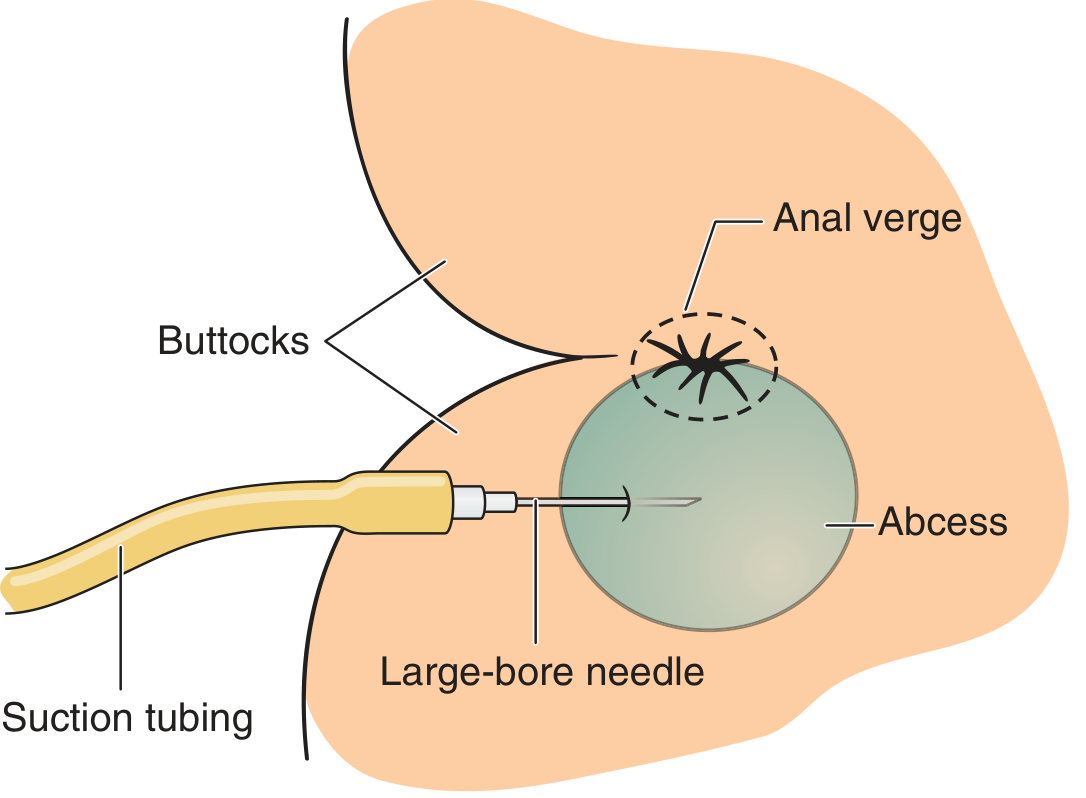
- A 16-gauge or larger needle + suction can temporarily decompress the abscess and provide dramatic pain relief. Disadvantage: makes fistula evaluation more difficult.
Clinical Photographs
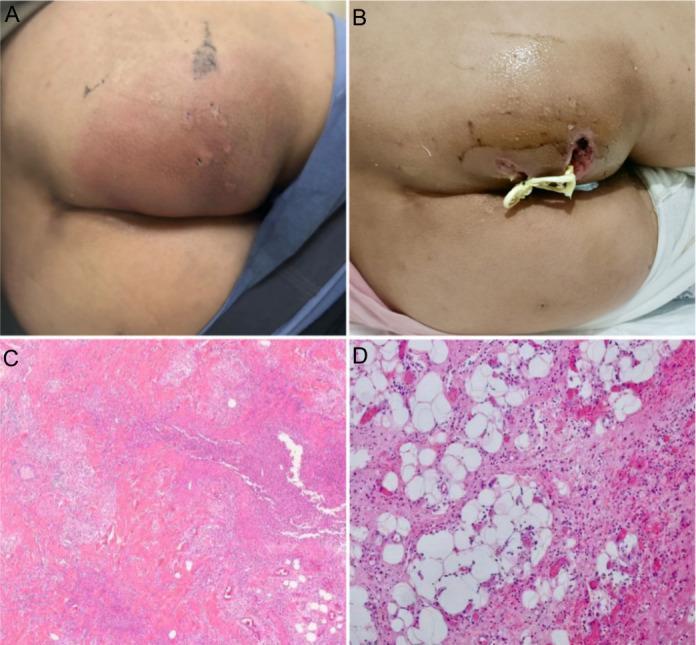
(A) Pre-op: tense, erythematous perianal mass. (B) Post-I&D with Penrose drain. (C–D) Histology: dense neutrophilic infiltrate, tissue necrosis confirming acute abscess.
Anesthesia Decision Guide
| Abscess Type | Setting | Anesthesia |
|---|---|---|
| Small, superficial perianal | Outpatient | Local (may be marginal) |
| Larger perianal / uncertain extent | ED or outpatient OR | Local + sedation or spinal |
| Ischiorectal / intersphincteric / supralevator | OR | Spinal or general |
Antibiotics
Postoperative antibiotics are generally NOT required after adequate I&D.
Consider antibiotics in:
- Immunocompromised patients
- Extensive surrounding cellulitis
- Sepsis
- Valvular heart disease
- Diabetes with systemic signs
- Patients on multiple prior antibiotic courses
Cultures: Not routinely needed. Useful in the above groups and to distinguish cryptoglandular abscess (colonic flora) from perianal skin abscess (staphylococcal).
Complications
| Complication | Notes |
|---|---|
| Recurrence (most common) | Usually due to unrecognized fistula-in-ano — evaluate all recurrences for fistula |
| Fistula-in-ano | Chronic sequela; patient should be referred for definitive fistulotomy |
| Crohn's disease | Consider in recurrent or atypical cases |
| Necrotizing fasciitis / Fournier's gangrene | If I&D is delayed; perirectal abscesses can serve as portal of entry |
| Bleeding | Uncommon |
| Sepsis / death | Associated with delay, inadequate drainage, and systemic disease |
Postprocedure Care
- Sitz baths 10–15 minutes, 2–4 times/day, starting 24 hours after surgery
- Wound must heal from inside out — prevent premature skin-edge closure
- Daily wound irrigations if no gauze packing is used
- Follow up to rule out fistula-in-ano, inflammatory bowel disease
Sources:
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed., Chapter 107
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Mulholland and Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.