Diabetic foot syndrome surgery
Reading File
Finding Sources
Searching PubMed
"diabetic foot" AND surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive surgical content from multiple authoritative textbooks. Let me compile the full answer.
Diabetic Foot Syndrome: Surgical Management
Pathophysiology Driving Surgical Need
Diabetic foot syndrome (DFS) arises from a triad of peripheral neuropathy, ischemia (PAD), and infection. Neuropathy causes loss of protective sensation, motor imbalance (claw toes, hammer toes, fat pad migration), autonomic dysfunction (dry, fissured skin), and a blunted awareness of injury. PAD - disproportionately affecting tibial and pedal vessels in diabetics - leads to chronic limb-threatening ischemia (CLTI). The two compound each other: diabetic patients with PAD are nine times more likely to develop a foot ulcer.
- Current Surgical Therapy 14e, p. 1186
- Campbell's Operative Orthopaedics 15th Ed, p. 5054
Classification Systems Used Surgically
| System | Basis | Surgical Relevance |
|---|---|---|
| Wagner (0-5) | Ulcer depth + necrosis | Most widely used; grades 3-5 drive surgery |
| University of Texas | Depth + ischemia + infection | Predicts healing and amputation risk |
| WIfI (SVS) | Wound + Ischemia + foot Infection (0-3 each) | 64 permutations - guides revascularization timing and predicts major amputation risk at 1 year |
| IWGDF/IDSA PEDIS | Perfusion, Extent, Depth, Infection, Sensation | Grades 1-4; Grade 4 = systemic sepsis, mandates urgent surgery |
The WIfI classification is the current standard in vascular surgery practice, strongly correlating with wound healing time, amputation-free survival, and whether revascularization is required before or after debridement. - Current Surgical Therapy 14e, p. 1187
Preoperative Assessment
Before any surgical intervention, a full workup is mandatory:
Vascular assessment:
- Ankle-Brachial Index (ABI): normal 0.9-1.2; <0.5 = unlikely to heal without revascularization; >1.3 = non-compressible (falsely elevated due to calcification)
- Toe-Brachial Index (TBI): more reliable in diabetics; absolute toe pressure >40 mmHg needed for healing; >70 mmHg is normal
- CT angiography or duplex ultrasound to map lesions before bypass planning
Imaging:
- Plain X-ray: 3-view foot X-ray for all patients - assess for osteomyelitis (may be normal early), Charcot deformity, prior amputations, structural abnormalities
- MRI: most sensitive modality for osteomyelitis and deep soft tissue involvement
- Labeled WBC scan or dual Tc/Indium scan: more sensitive and specific for osteomyelitis than Tc scan alone
Laboratory:
- CBC, CRP, ESR, HbA1c (>7% or pre-op glucose >200 mg/dL raises complication risk)
- Albumin <2.5 g/dL, total protein <6.0 g/dL, WBC <1500/mm³ = poor healing potential
Microbiology:
-
Superficial swabs are unreliable - deep tissue biopsy or bone biopsy is gold standard
-
Probe-to-bone test + elevated inflammatory markers + abnormal X-ray = confirms osteomyelitis clinically
-
Miller's Review of Orthopaedics 9th Ed, p. 639; Bailey & Love 28th Ed, p. 628
Surgical Procedures
1. Debridement and Wound Care Surgery
The most common intervention. Indicated for all infected ulcers with necrosis, deep abscess, or osteomyelitis.
Principles:
- Debride all nonviable tissue back to healthy bleeding margins
- Wounds are generally left open to drain and heal by secondary intention
- Incision for abscess drainage should allow full access while minimizing wound burden - especially critical in PAD patients
- Probe the wound to rule out deep space extension or sinus tracts from bone
Urgent (emergency) debridement indications:
- Necrotizing fasciitis or gas gangrene (all diseased soft tissue, muscle, and bone to healthy margins)
- Deep space abscess
- Compartment syndrome
- Limb-threatening ischemia with sepsis
Early debridement is associated with lower rates of major amputation. - Sabiston Textbook of Surgery, p. 643
2. Osteomyelitis Surgery
Osteomyelitis is present in 67% of foot ulcerations that reach bone. - Miller's Review of Orthopaedics
Options:
- Conservative (antibiotics alone): 6-week IV antibiotics if perfusion is adequate and bone involvement is limited; bone resection may be avoidable in ~2/3 of patients
- Limited bone resection/sequestrectomy: Excise infected bone while preserving foot architecture; excess bone resected to allow tension-free skin closure
- Ray resection: Removal of a metatarsal + digit as a unit when bone/joint is involved
- Transmetatarsal amputation (TMA): When forefoot osteomyelitis is widespread; elevated HbA1c increases failure risk
Superficial osteitis (bone exposure from skin loss without true medullary invasion) may be managed with glycemic control, pressure offloading, and vascular optimization rather than resection. - Bailey & Love 28th Ed, p. 628
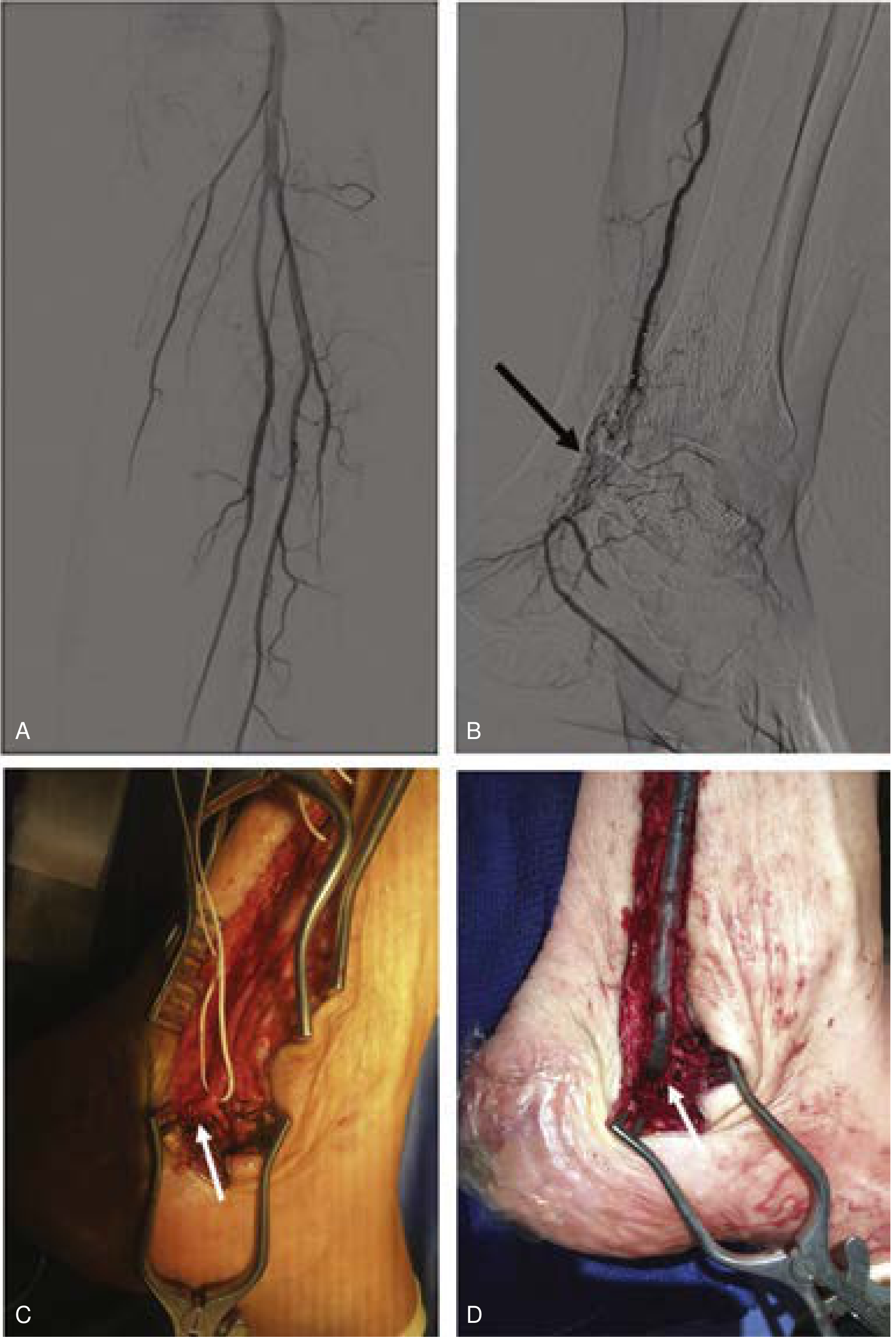
3. Revascularization
Mandatory when ischemia is contributing and the wound is not healing with maximal wound care.
Indications:
- WIfI ischemia grade 1+ in most wound types
- Toe pressure 60-80 mmHg with wound not healing at 4-6 weeks
- All grade 2+ ischemia
Sequencing rule:
- If wound is frankly infected → debridement first, then angiography
- If subacute/chronic infection → angiography first to prevent ischemic necrosis post-debridement
Techniques:
- Endovascular (PVI): First-line for most tibial lesions; lower perioperative complications; decreased patency below the knee vs. open bypass
- Open bypass: Preferred for long-segment occlusions, heavily calcified non-crossable lesions; uses single-segment great saphenous vein (or arm vein); tibial bypasses performed in translocated (non-reversed) fashion with valve lysis
- Both approaches show equivalent amputation-free survival at 4 years in experienced centers
Last resort: Hyperbaric oxygen (HBO) for osteomyelitis, gangrene, or inadequately perfused open wounds not amenable to revascularization. - Current Surgical Therapy 14e, p. 1188
4. Amputation Levels
Amputation in diabetic foot disease is particularly challenging because healing can be unreliable due to ischemia and neuropathy. The principle is to resect all infected material with enough bone to allow tension-free skin closure.

| Level | Indication | Key Points |
|---|---|---|
| Toe amputation | Isolated digit gangrene/osteomyelitis | Preserves most foot function |
| Ray resection | Metatarsal + digit infection | Narrows forefoot; structural issues |
| Transmetatarsal amputation (TMA) | Forefoot gangrene not extending to midfoot | Requires good heel/ankle perfusion; HbA1c elevation = failure risk |
| Chopart amputation | Midfoot disease | Anterior tibialis transferred to talus (prevents varus) + Achilles lengthening (prevents equinus) to prevent deformity |
| Syme amputation | Forefoot/midfoot disease with intact heel pad | Requires intact heel pad; end-bearing stump |
| Transtibial (below-knee) | Extensive foot disease, failed foot salvage | 25% more energy expenditure (traumatic), 40% more energy (vascular) vs. baseline; preferred over transfemoral when possible |
| Transfemoral (above-knee) | Failed below-knee, proximal disease | 68-100% more energy expenditure; significantly worse rehabilitation |
Key principle: If there is extensive peripheral neuropathy, a below-knee amputation in a zone with better sensation may be preferable to complex foot reconstruction. - Bailey & Love 28th Ed; Miller's Review of Orthopaedics
5. Structural/Deformity Correction Surgery
Wounds caused by structural deformity (bunion, claw toe, hammer toe, equinus) have a high recurrence rate with wound care alone. Surgical correction addresses the underlying mechanical cause.
Procedures:
- Achilles tendon lengthening (ATL): Reduces forefoot peak pressure; indicated with gastrocnemius/equinus contracture
- Flexor tenotomy: Relieves tip-of-toe ulcers from claw deformity
- Metatarsal head resection: For metatarsal head plantar ulcers
- Calcaneal osteotomy / exostectomy: For calcaneal pressure ulcers
6. Charcot Neuroarthropathy Surgery
Charcot foot (acute neuropathic arthropathy) can lead to progressive midfoot collapse, rocker-bottom deformity, and subsequent ulceration/osteomyelitis.
Non-operative first: Total contact casting (TCC) is first-line for acute Charcot (offloading until quiescence).
Surgical indications:
- Unstable or unbraceable deformity
- Recurrent ulceration despite offloading
- Osteomyelitis in the Charcot foot
Procedures:
-
Exostectomy: Resection of plantar bony prominence causing ulceration
-
Midfoot/hindfoot arthrodesis: Corrects deformity and provides a stable, braceable, plantigrade foot
-
Tibiotalocalcaneal (TTC) arthrodesis with intramedullary (IM) rod: Gold standard for unstable hindfoot Charcot; IM rod provides internal stability and can be left indefinitely; even radiographic nonunion often leaves patients pain-free
-
External fixator (multiplanar): Alternative to IM rod but removed after healing
-
Miller's Review of Orthopaedics 9th Ed, p. 639
Multidisciplinary Team (MDT) Approach
The development of dedicated MDT programs has been shown to reduce LEA rates through early recognition and risk factor management. The ideal team includes:
- Vascular surgeon (revascularization, limb threat assessment)
- Orthopaedic/podiatric surgeon (deformity correction, amputation)
- Infectious disease specialist (antibiotic stewardship)
- Endocrinologist/diabetologist (glycemic control)
- Wound care nurse / prosthetist
- Rehabilitation medicine
Postoperative and Wound Care Adjuncts
- Negative pressure wound therapy (NPWT/VAC): Meta-analysis (PMID 39241769) supports NPWT for diabetic foot ulcer healing in RCTs
- Offloading: Total contact cast is gold standard; irremovable devices are superior to removable ones per IWGDF 2023 guidelines (PMID 37226568)
- HBO therapy: For wounds with tcPO₂ <40 mmHg and non-revascularizable ischemia
- Glycemic optimization: HbA1c control is linked to fewer complications, less neuropathy progression, and better healing post-arthrodesis
Key Surgical Pearls (High-Yield)
- Osteomyelitis is present in 67% of ulcers probing to bone
- HbA1c >7% or pre-op glucose >200 increases risk of TMA failure, nonunion, and wound breakdown
- Syme amputation requires an intact heel pad
- Chopart amputation requires anterior tibialis transfer to talus + Achilles lengthening
- Superficial swabs are unreliable - use deep tissue or bone biopsy for culture
- Vascular assessment is mandatory before any surgical foot intervention
- Debridement before angiography if frank infection; angiography before debridement if subacute/chronic infection
- 5-year survival after major amputation drops from 70% to 43% - foot salvage is always the priority
This is a shared conversation. Sign in to Orris to start your own chat.