What are the standard test for diagnosis of anemia
Reading File
Searching the Web
standard diagnostic tests for anemia CBC iron studies
Finding Sources
Searching PubMed
"anemia" AND "diagnosis" AND "laboratory tests"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have sufficient information from Harrison's Principles, Goldman-Cecil Medicine, and the Quick Compendium of Clinical Pathology to provide a thorough, well-structured answer. Let me compile it:
Standard Tests for the Diagnosis of Anemia
The diagnostic workup for anemia follows a step-wise approach, moving from basic screening tests to more specific confirmatory tests depending on the initial findings.
1. Complete Blood Count (CBC)
This is always the first and most important test. It is performed by electronic cell counters and provides:
| Index | Formula | Normal Range | What it tells you |
|---|---|---|---|
| Hemoglobin (Hgb) | Directly measured | Male: >13.5 g/dL; Female: >12 g/dL | Confirms anemia |
| Hematocrit (Hct) | RBC × MCV | Male: ~41-53%; Female: ~36-46% | Reflects red cell mass |
| MCV (Mean Corpuscular Volume) | Hct/RBC × 10 | 85-95 fL | Classifies anemia by cell size |
| MCH (Mean Corpuscular Hemoglobin) | Hgb/RBC × 10 | 28.5-32.3 pg | Varies with MCV |
| MCHC (Mean Corpuscular Hgb Concentration) | Hgb/Hct × 100 | 33.8-34.2 g/dL | Detects hypochromia |
| RDW (Red Cell Distribution Width) | — | 11.5-14.5% | Reflects anisocytosis (variation in cell size) |
| RBC count | Directly measured | — | Useful in distinguishing iron deficiency from thalassemia |
MCV is the cornerstone of classifying anemia:
- Microcytic (MCV <80 fL): Iron deficiency, thalassemia, anemia of chronic disease, sideroblastic anemia
- Normocytic (MCV 80-100 fL): Aplastic anemia, renal disease, endocrinopathies, early iron deficiency
- Macrocytic (MCV >100 fL): B12/folate deficiency, liver disease, hypothyroidism, alcohol use, myelodysplasia
(Harrison's Principles of Internal Medicine 22E, p. 488)
2. Peripheral Blood Smear
A direct examination of red cell morphology - described by Harrison's as "a crucial part of any evaluation for anemia." It identifies:
| Morphology | Significance |
|---|---|
| Hypochromia / microcytosis | Iron deficiency, thalassemia, sideroblastic anemia |
| Macro-ovalocytes | B12/folate deficiency, myelodysplasia |
| Schistocytes (cell fragments) | Microangiopathic hemolysis (TTP, HUS), valve hemolysis |
| Spherocytes | Autoimmune hemolytic anemia, hereditary spherocytosis |
| Sickle cells | Sickle cell disease |
| Target cells | Liver disease, thalassemia, hemoglobinopathies |
| Basophilic stippling | Thalassemia, lead poisoning |
| Teardrop cells (dacrocytes) | Primary myelofibrosis, marrow infiltration |
| Polychromasia | Reticulocytosis (hemolysis, hemorrhage) |
| Nucleated RBCs | Severe marrow stress, asplenia |
| Elliptocytes / pencil cells | Iron deficiency, hereditary elliptocytosis |
(Goldman-Cecil Medicine, p. 1660; Harrison's 22E, p. 489)
3. Reticulocyte Count
This measures new red cells released by the bone marrow and is the key test for determining the mechanism of anemia:
- Low/normal reticulocytes → Hyporegenerative (production defect): aplastic anemia, iron/B12/folate deficiency, renal failure, marrow infiltration
- Elevated reticulocytes → Hyperregenerative: blood loss or hemolysis
The absolute reticulocyte count (reticulocytes/100 × RBC number) is preferred as it does not require correction for the degree of anemia. A corrected reticulocyte count (reticulocyte index) adjusts for the patient's hematocrit.
(Harrison's 22E, p. 491; Quick Compendium of Clinical Pathology 5th ed., p. 233)
4. Iron Studies
Ordered when microcytic or iron deficiency anemia is suspected:
| Test | Iron Deficiency | Anemia of Chronic Disease |
|---|---|---|
| Serum Iron | Low | Low |
| TIBC (Total Iron Binding Capacity) | High | Low/Normal |
| Transferrin Saturation | Low (<20%) | Low/Normal |
| Serum Ferritin | Low (<12 µg/L) | Normal/High |
- Ferritin is the most sensitive single test for iron deficiency (it is a storage protein; low ferritin essentially confirms depleted stores)
- Up to 40% of iron-deficient patients will have a normal MCV, so iron studies should be considered in all anemias unless MCV >95 fL
5. Vitamin B12 and Folate Levels
Ordered for macrocytic anemia or suspected megaloblastic anemia:
- Low serum B12 (<200 pg/mL) or low RBC folate confirms deficiency
- Methylmalonic acid (MMA) and homocysteine levels are more sensitive confirmatory tests - MMA is elevated in B12 deficiency only, while homocysteine is elevated in both
6. Hemolysis Workup
When hemolytic anemia is suspected (elevated reticulocyte count, jaundice, dark urine):
| Test | Significance |
|---|---|
| LDH (Lactate Dehydrogenase) | Elevated in hemolysis (released from destroyed RBCs) |
| Indirect bilirubin | Elevated (from heme breakdown) |
| Haptoglobin | Decreased (binds free hemoglobin released during hemolysis) |
| Direct Coombs test (DAT) | Positive in immune-mediated hemolytic anemia |
| Free plasma hemoglobin | Elevated in intravascular hemolysis |
7. Bone Marrow Examination
Indicated when peripheral blood findings suggest:
- Aplastic anemia (pancytopenia)
- Myelodysplasia
- Marrow infiltration (malignancy, fibrosis)
- Unexplained severe anemia
- Pure red cell aplasia
Includes both aspiration (cell morphology, differential count, myeloid:erythroid ratio) and biopsy (architecture, cellularity, infiltrates). Bone marrow iron stores can also be assessed with special staining.
(Harrison's Principles 22E, p. 491)
8. Additional/Specialized Tests
| Test | When to Order |
|---|---|
| Hemoglobin electrophoresis | Suspected thalassemia or hemoglobinopathy |
| Osmotic fragility test | Suspected hereditary spherocytosis |
| G6PD assay | Suspected G6PD deficiency (especially after hemolytic episode) |
| TSH | Macrocytic anemia (hypothyroidism causes macrocytosis) |
| Renal function (creatinine/BUN) | Normocytic anemia (EPO deficiency in CKD) |
| Serum protein electrophoresis | Suspected multiple myeloma |
| Lead level | Basophilic stippling, occupational exposure |
| Stool occult blood | Suspected GI blood loss in iron deficiency |
Diagnostic Summary Algorithm
CBC + Blood Smear + Reticulocyte Count
|
MCV Classification
/ | \
Microcytic Normocytic Macrocytic
| | |
Iron studies Reticulocyte B12/Folate
(ferritin, count high? levels
TIBC) / \
Yes No
Hemolysis Bone marrow
workup vs. renal/
endocrine
The ARUP Consult anemia algorithm and the AAFP guidelines both confirm this sequential approach as standard practice.
Confirmatory test for maleria
Reading File
Searching the Web
confirmatory diagnostic tests malaria WHO guidelines 2024
Finding Sources
Searching PubMed
"malaria" AND "diagnosis" AND "rapid diagnostic test"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook content and real microscopy images. Here is the full answer:
Confirmatory Tests for Malaria
Key principle from Harrison's 22E: "Malaria is not a clinical diagnosis." All suspected cases must be confirmed with parasite-based testing before treatment is initiated. (Harrison's Principles of Internal Medicine 22E, p. 1810)
1. Blood Smear Microscopy (GOLD STANDARD)
This is the definitive confirmatory test for malaria. It involves examining Giemsa-stained thick and thin blood films under oil immersion microscopy (×1000 magnification).
Thick Blood Smear
- Red cells are lysed during staining, concentrating parasites by 40-100 fold compared to a thin film
- Used primarily to detect the presence of parasites (higher sensitivity)
- Both parasites and WBCs are counted; parasitemia is expressed as parasites per µL
- At least 100-200 fields must be examined before calling a smear negative
- A minimum of 200 WBCs should be counted under oil immersion
Thin Blood Smear
- RBCs remain intact; examined at the tail of the film where cells are not overlapping
- Used for species identification and quantifying parasitemia (% infected RBCs)
- Parasitemia expressed as number of parasitized erythrocytes per 1000 RBCs
Staining
- Giemsa stain at pH 7.2 is preferred (Romanowsky stain)
- Field's, Wright's, or Leishman's stains can also be used
- Acridine orange (fluorescent dye) allows more rapid diagnosis in low-level parasitemia, but cannot be used for speciation
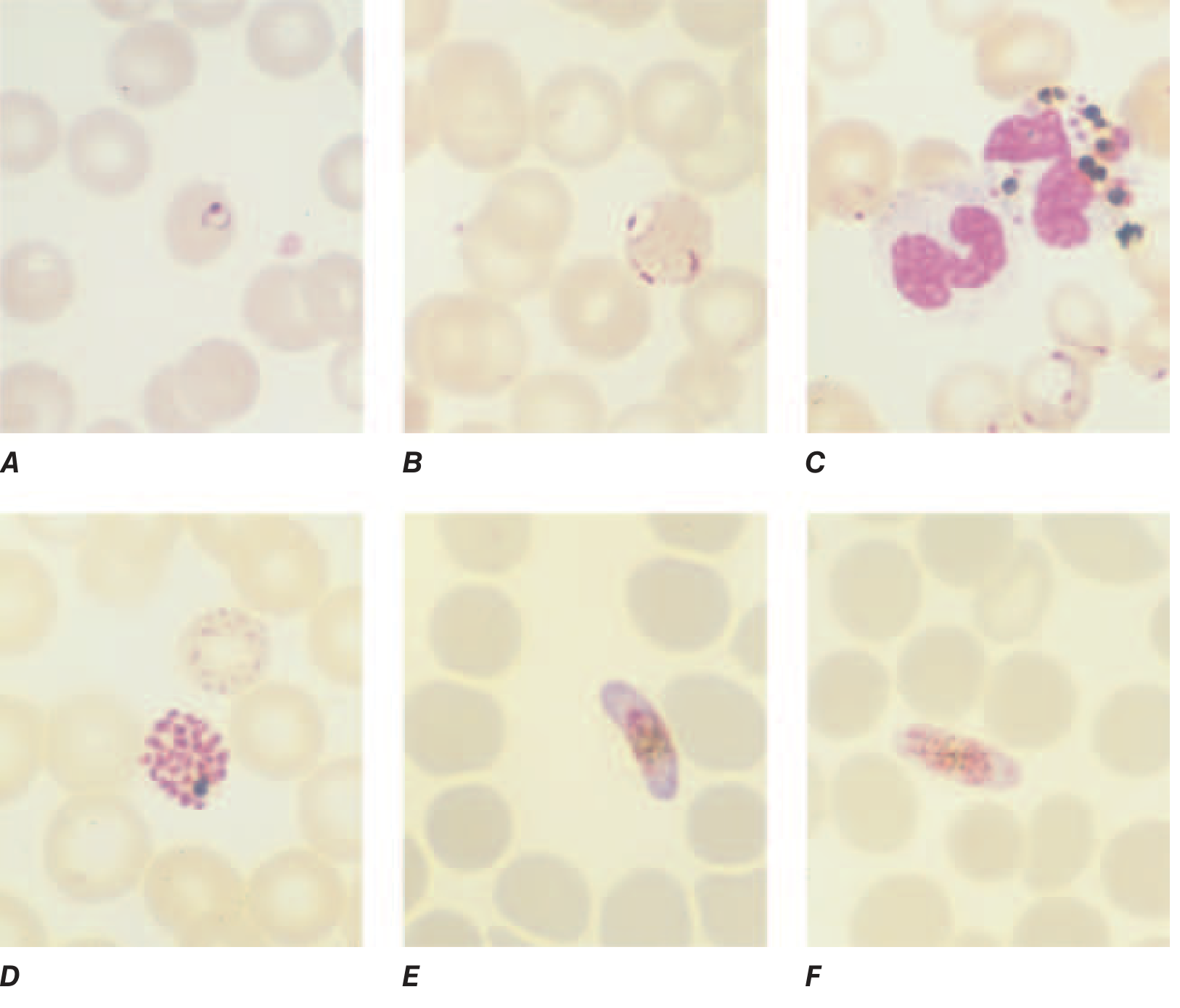
Microscopy images of Plasmodium falciparum (thin smear):
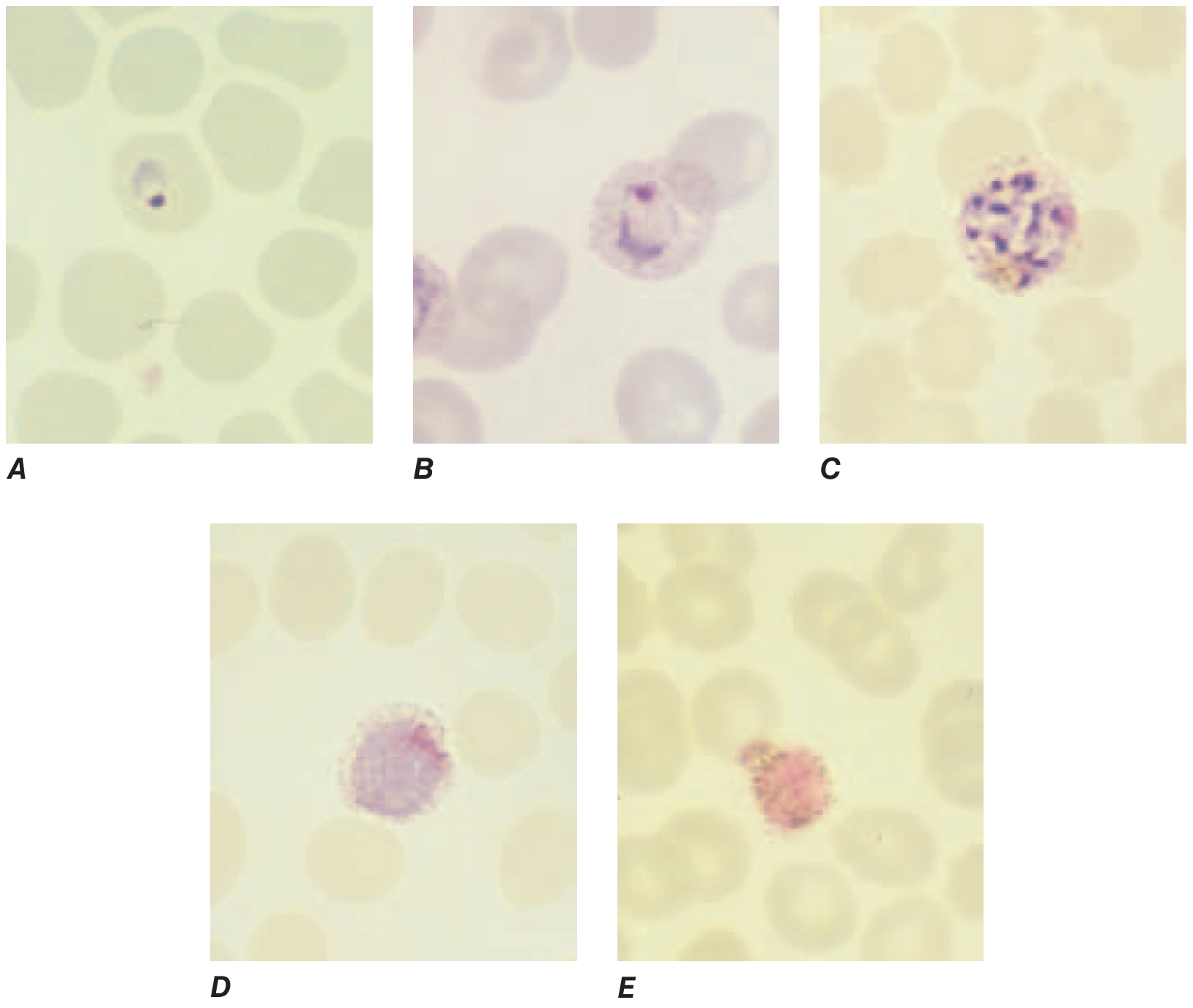
Microscopy images of Plasmodium vivax (thin smear):
2. Rapid Diagnostic Tests (RDTs)
RDTs detect malaria parasite antigens from a finger-prick blood sample. They produce results within 15-20 minutes and can be performed under field conditions without a microscope. WHO recommends confirming all suspected malaria with either microscopy or RDT before treatment.
Antigens Detected
| RDT Type | Antigen Detected | Species |
|---|---|---|
| Monovalent (HRP2-based) | Histidine-Rich Protein 2 (HRP-2) | P. falciparum only |
| Bivalent (pLDH-based) | Parasite Lactate Dehydrogenase (pLDH) | P. falciparum AND P. vivax |
| Pan-malaria | Aldolase or pan-pLDH | All Plasmodium species |
- ParaSight F (HRP2-based): sensitivity >95% for P. falciparum
- OptiMAL (pLDH-based): distinguishes between P. falciparum and P. vivax
Limitations of RDTs:
- Cannot quantify parasitemia
- Cannot reliably speciate alone - microscopy should still be performed alongside RDT
- HRP2-based RDTs may remain positive for weeks after treatment due to antigen persistence
- Emerging hrp2/hrp3 gene deletions in P. falciparum (especially in parts of Africa and South America) can cause false-negative HRP2 RDT results - a growing concern per recent WHO guidance
(Sherris & Ryan's Medical Microbiology, 8th ed., p. 1705)
3. PCR (Polymerase Chain Reaction)
PCR is the most sensitive confirmatory method, detecting parasite DNA from blood samples.
- Sensitivity: superior to both microscopy and RDT, especially for low-density parasitemia
- Can precisely identify species and even distinguish mixed infections
- Detects drug resistance markers: dhfr mutations (antifolates), Pfcrt mutations (chloroquine), Pfkelch13 mutations (artemisinin), Pfmdr1 amplification (mefloquine)
- Limitation: not suitable for acutely ill patients because results take days; primarily used for research, epidemiological surveillance, and reference lab confirmation
(Harrison's 22E, p. 1810)
4. Quantitative Buffy Coat (QBC) Technique
- Involves acridine orange staining of parasites concentrated by centrifugation in capillary tubes
- Requires a fluorescence microscope
- More rapid and sensitive than standard smear for detecting parasites
- Cannot reliably speciate infections
- Mainly used in reference or hospital laboratories that only occasionally diagnose malaria
5. Serology (Antibody Detection)
- Detects anti-malarial antibodies (IgG/IgM), not the parasite itself
- Available only at large reference laboratories
- Used primarily for epidemiological surveys, not for acute diagnosis
- Occasionally helpful for speciation and detecting occult/past infections
- Not used routinely for confirming acute malaria
Comparison Summary
| Test | Sensitivity | Speciation | Parasitemia Quantification | Practical Setting |
|---|---|---|---|---|
| Thick smear (Giemsa) | High | No | Yes | Routine |
| Thin smear (Giemsa) | Moderate | Yes | Yes | Routine |
| RDT (HRP2) | >95% for P. falciparum | Partial | No | Field/POC |
| RDT (pLDH) | High | Pf vs Pv | No | Field/POC |
| QBC/Acridine orange | High | No | No | Reference lab |
| PCR | Highest | Best | No | Reference lab only |
| Serology | Low (acute) | Limited | No | Epidemiology only |
WHO/CDC Diagnostic Algorithm
Suspected malaria (fever + travel to endemic area)
↓
Prepare thick + thin blood smear IMMEDIATELY
↓
Reliable microscopy available?
YES → Examine smear (detect + speciate + quantify)
NO → Perform RDT
↓
If smear negative but clinical suspicion high →
Repeat smear every 12-24h × 3 (negative ×3 = not malaria)
↓
If low-density parasitemia or species unclear →
Send for PCR (reference lab)
(Park's Textbook of Preventive and Social Medicine; CDC Malaria Diagnostic Guidelines June 2024)
Recent evidence note: A 2025 systematic review and meta-analysis (PMID: 41366413) on RDT performance in Nigeria found variable sensitivity across product brands, reinforcing that microscopy remains the reference standard and RDTs should not be used as the sole diagnostic tool where microscopy expertise is available.
This is a shared conversation. Sign in to Orris to start your own chat.