Explain me everything about anatomy of digestive system. Salivary glands, accessory organs, abdomen section. Digestive system organs everything don't miss a single detail.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Searching the Web
digestive system anatomy complete overview organs functions 2024
I now have extensive detail from Gray's Anatomy for Students and web sources. Let me compile the comprehensive answer.
Complete Anatomy of the Digestive System
The digestive system (also called the alimentary canal or gastrointestinal tract) is a continuous muscular tube extending from the mouth to the anus, approximately 8-9 meters long in adults. It is divided into the primary GI tract and accessory organs that support digestion from outside the main tube.
1. OVERVIEW: DIVISIONS OF THE DIGESTIVE SYSTEM
| Division | Organs |
|---|---|
| Primary GI tract | Oral cavity, pharynx, esophagus, stomach, small intestine, large intestine, rectum, anus |
| Accessory organs | Salivary glands, teeth, tongue, liver, gallbladder, pancreas |
Food is propelled along the GI tract by peristalsis - coordinated waves of circular and longitudinal muscle contraction - while accessory organs secrete enzymes, acids, and bile into the lumen to facilitate chemical digestion.
2. ORAL CAVITY (MOUTH)
The oral cavity is the first segment of the digestive system. It performs:
- Mechanical digestion via mastication (chewing by teeth)
- Chemical digestion begins here via salivary amylase
- Bolus formation - food mixed with saliva into a soft mass
Boundaries:
- Anterior: lips
- Posterior: oropharyngeal isthmus
- Lateral walls: cheeks (buccinator muscle)
- Roof: hard palate anteriorly, soft palate posteriorly
- Floor: tongue and mylohyoid muscle
Key structures:
- Teeth - 32 permanent teeth: 8 incisors (cutting), 4 canines (tearing), 8 premolars, 12 molars (grinding). Each tooth has a crown, neck, and root. The pulp cavity contains blood vessels and nerves.
- Tongue - a muscular organ composed of intrinsic muscles (alter tongue shape) and extrinsic muscles (genioglossus, hyoglossus, styloglossus, palatoglossus - move tongue). Covered by mucosa with papillae. The oral part (anterior 2/3) is separated from the pharyngeal part (posterior 1/3) by the sulcus terminalis. It is innervated by CN XII (motor), CN V3 (general sensation anterior 2/3), CN VII chorda tympani (taste anterior 2/3), CN IX (taste/sensation posterior 1/3).
- Hard palate - formed by palatine processes of maxillae and horizontal plates of palatine bones; provides a rigid surface for tongue to press food against
- Soft palate - muscular fold posterior to hard palate; closes off nasopharynx during swallowing via levator veli palatini and tensor veli palatini muscles
3. SALIVARY GLANDS
Salivary glands open or secrete into the oral cavity. Most are small mucous glands in the submucosa/mucosa of the tongue, palate, cheeks, and lips. The major glands are three paired structures.
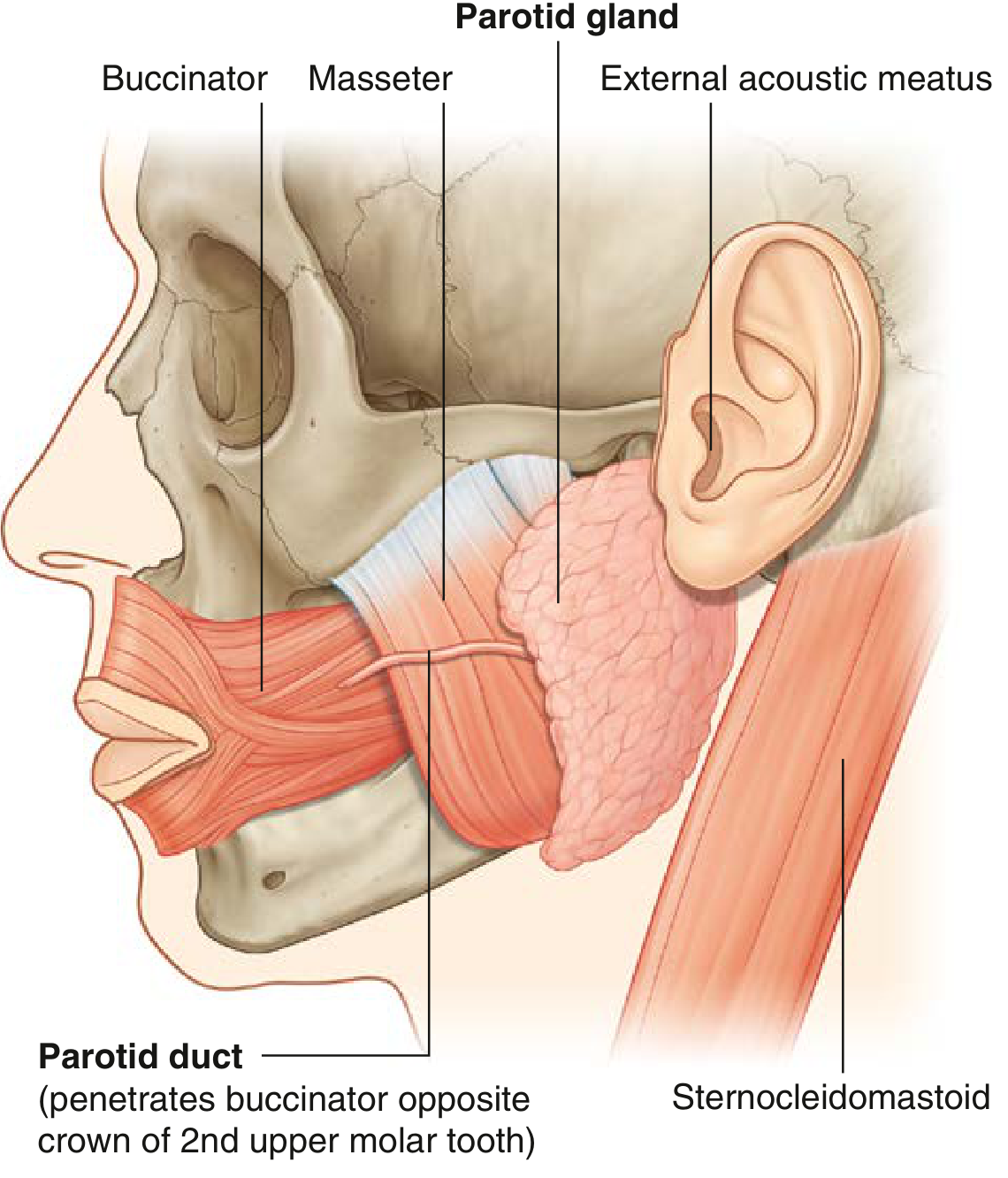
3a. Parotid Gland
The largest of the three major pairs.
Location: Occupies a shallow, triangular-shaped trench (parotid bed) bounded by:
- Posteriorly: sternocleidomastoid muscle
- Anteriorly: ramus of the mandible
- Superiorly: external acoustic meatus and posterior aspect of zygomatic arch
The gland extends anteriorly over the masseter muscle and inferiorly over the posterior belly of the digastric muscle.
Parotid duct (Stensen's duct): Passes anteriorly across the external surface of the masseter muscle, then turns medially to penetrate the buccinator muscle and opens into the oral cavity adjacent to the crown of the second upper molar tooth.
Contents enclosed within the gland:
- External carotid artery
- Retromandibular vein
- Origin of the extracranial facial nerve (CN VII)
Vasculature: Arteries from the external carotid artery and its adjacent branches. Veins drain into the external jugular vein.
Lymphatics: Into nodes on/in the gland (parotid nodes), then to superficial and deep cervical nodes.
Innervation: Parasympathetic fibers originate from CN IX (glossopharyngeal nerve) → tympanic nerve → lesser petrosal nerve → otic ganglion → auriculotemporal nerve (branch of CN V3) → parotid gland. Sympathetic supply travels along the external carotid artery.
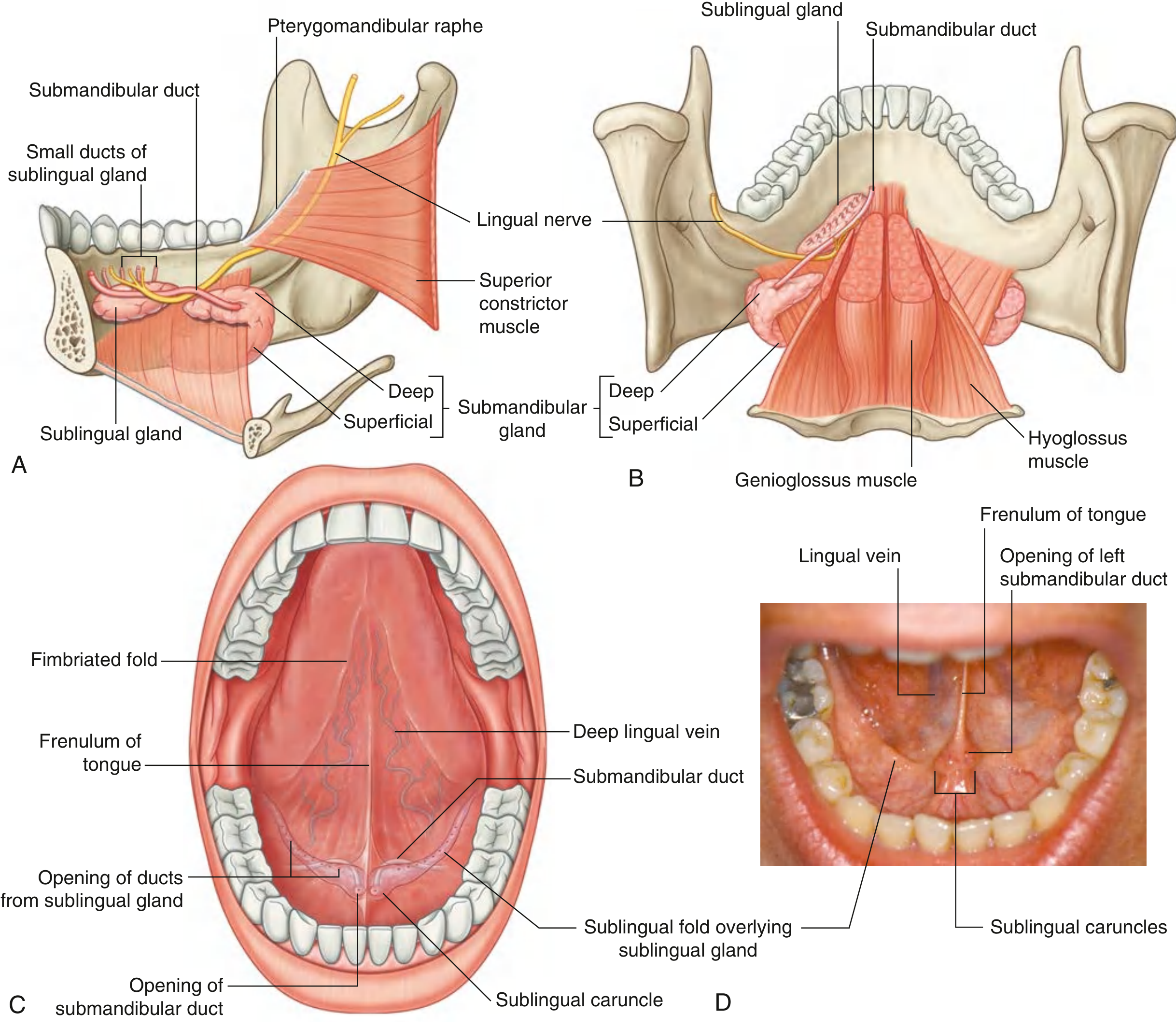
3b. Submandibular Glands
Size: Smaller than parotid but larger than sublingual. Hook-shaped with a larger superficial part and a smaller deep part.
Location:
- Superficial (larger) part: Below the mylohyoid muscle in the horizontal plane, outside the oral cavity proper - lies against the submandibular fossa on the medial surface of the mandible inferior to the mylohyoid line
- Deep (smaller) part: Loops around the posterior margin of the mylohyoid muscle into the floor of the oral cavity, lateral to the root of the tongue on the lateral surface of the hyoglossus muscle
Submandibular duct (Wharton's duct): Emerges from the medial side of the deep part in the oral cavity, passes forward, and opens on the summit of the sublingual caruncle (papilla) beside the base of the frenulum of the tongue. The lingual nerve loops under this duct, crossing first its lateral and then its medial side.
Vasculature: Supplied by branches of the facial and lingual arteries. Veins drain into lingual and facial veins.
Lymphatics: Mainly to submandibular nodes, then to deep cervical nodes (especially jugulo-omohyoid node).
Innervation: Parasympathetic from CN VII (facial nerve) via chorda tympani → lingual nerve → submandibular ganglion → submandibular gland. Sympathetic from superior cervical ganglion along facial/lingual arteries.
3c. Sublingual Glands
The smallest of the three major pairs.
Shape: Almond-shaped, immediately lateral to the submandibular duct and lingual nerve in the floor of the oral cavity.
Location: Lies directly against the medial surface of the mandible in the sublingual fossa, superior to the anterior one-third of the mylohyoid line.
The superior margin raises an elongate mucosal fold - the sublingual fold - which extends from the posterolateral floor of the oral cavity to the sublingual papilla at the midline anteriorly.
Drainage: Via numerous minor sublingual ducts (Rivinus ducts) opening onto the crest of the sublingual fold. Occasionally, a major sublingual duct (Bartholin's duct) drains the anterior portion alongside the submandibular duct at the sublingual caruncle.
Vasculature: Branches of facial and lingual arteries; veins into lingual and facial veins.
Lymphatics: To submandibular nodes then deep cervical nodes.
Innervation: Same as submandibular gland (chorda tympani of CN VII via submandibular ganglion).
Salivary Gland Innervation Summary
All major salivary glands receive parasympathetic innervation from branches of CN VII (facial nerve), which join branches of CN V2/V3 to reach their destinations:
- Parotid: CN IX → otic ganglion → CN V3 (auriculotemporal nerve)
- Submandibular & Sublingual: CN VII chorda tympani → submandibular ganglion → glands directly
Sympathetic innervation from the superior cervical ganglion traveling along the arteries supplying each gland causes vasoconstriction and reduced secretion.
4. PHARYNX
The pharynx is a musculofibrous tube approximately 12-14 cm long that connects the nasal/oral cavities to the esophagus and larynx. It is divided into three parts:
4a. Nasopharynx
- Superior part, behind the nasal cavity
- Contains the pharyngeal tonsil (adenoids) on the posterior wall
- Eustachian tube openings on each lateral wall
- Purely respiratory - food does not normally pass through
4b. Oropharynx
- Extends from the soft palate to the upper border of the epiglottis
- Palatine tonsils are located in the tonsillar fossa between the palatoglossal and palatopharyngeal arches
- Both food and air pass through
4c. Laryngopharynx (Hypopharynx)
- Extends from the upper border of the epiglottis to the lower border of the cricoid cartilage (C6), where it becomes the esophagus
- Piriform recesses (fossae) on either side of the laryngeal inlet - common site for foreign body impaction
Swallowing (Deglutition): Three phases:
- Oral phase (voluntary) - bolus pushed posteriorly by tongue
- Pharyngeal phase (involuntary) - soft palate closes off nasopharynx; epiglottis tilts down; larynx elevates; pharyngeal constrictors propel bolus
- Esophageal phase (involuntary) - peristaltic waves carry bolus to stomach
5. ESOPHAGUS
A muscular tube ~25 cm long, extending from the pharynx (C6) to the stomach (T11).
Anatomical course and constrictions:
The esophagus has four natural narrowings (clinically important for foreign body impaction and stricture formation):
- Cricopharyngeal constriction - at origin, where cricopharyngeus muscle forms the upper esophageal sphincter (UES), C6, ~15 cm from incisors
- Aortic arch constriction - where the arch of the aorta crosses, ~22-23 cm from incisors
- Left main bronchus constriction - where the left main bronchus crosses, ~27 cm from incisors
- Diaphragmatic constriction (hiatus) - as it passes through the esophageal hiatus of the diaphragm (T10), ~38-40 cm from incisors
Regions:
- Cervical esophagus: C6 to T1; related to trachea anteriorly, prevertebral fascia posteriorly, recurrent laryngeal nerves in the grooves laterally
- Thoracic esophagus: T1 to T10; passes through the posterior mediastinum; initially right of midline, then crosses behind the aorta to the left
- Abdominal esophagus: Short segment (~1-2 cm) below the hiatus before joining the stomach at the gastroesophageal junction
Wall layers (from inside out):
- Mucosa: non-keratinized stratified squamous epithelium
- Submucosa: contains mucous glands
- Muscularis externa: upper 1/3 = skeletal muscle; middle 1/3 = mixed; lower 1/3 = smooth muscle
- Adventitia (no serosa - important: lack of serosa means tumor spreads easily)
Lower esophageal sphincter (LES): A functional high-pressure zone (~3-4 cm above the hiatus); prevents gastroesophageal reflux. When incompetent, causes GERD.
Gastroesophageal junction: Transition from squamous epithelium (esophagus) to columnar epithelium (stomach). When the histological junction shifts proximally into the lower esophagus, this is Barrett's esophagus - a metaplastic change associated with chronic GERD and increased adenocarcinoma risk.
Blood supply:
- Cervical: inferior thyroid arteries
- Thoracic: bronchial arteries + direct aortic branches
- Abdominal: left gastric artery and inferior phrenic arteries
Venous drainage: Important clinically - lower esophageal veins drain into the portal system (left gastric vein), creating a porto-systemic anastomosis. Portal hypertension causes esophageal varices here.
Innervation: Vagus nerves (CN X) form the esophageal plexus; left vagus becomes anterior vagal trunk, right vagus becomes posterior vagal trunk at the esophageal hiatus.
6. STOMACH
The stomach is a J-shaped, muscular, distensible organ in the left upper quadrant (epigastric and left hypochondriac regions).
Capacity: ~1-1.5 liters empty, up to 3-4 liters when full.
Parts of the stomach:
- Cardia - surrounds the gastroesophageal junction (cardiac orifice)
- Fundus - dome-shaped part superior to the cardiac orifice; usually contains swallowed air (visible on upright X-ray)
- Body (corpus) - main central part; contains most gastric glands
- Pyloric antrum - distal funnel-shaped part leading to the pylorus
- Pylorus - the distal constriction with the thick pyloric sphincter (pyloric canal ~3 cm); connects to duodenum at the pyloric orifice
Curvatures:
- Lesser curvature (right/medial side): shorter; gives attachment to the lesser omentum; contains the incisura angularis (angular notch), a fixed landmark
- Greater curvature (left/lateral side): longer; gives attachment to the greater omentum, gastrosplenic ligament, and gastrocolic ligament
Wall layers (unique to stomach):
- Mucosa: simple columnar epithelium with gastric pits leading to gastric glands; rugae (longitudinal folds) allow distension
- Submucosa
- Muscularis externa: three layers (unique!) - outer longitudinal, middle circular (forms pyloric sphincter), inner oblique
- Serosa (peritoneum)
Gastric glands (by region):
- Cardia: mucous-secreting cells
- Fundus/body: chief cells (pepsinogen), parietal cells (HCl and intrinsic factor), mucous neck cells, enteroendocrine cells (G cells in antrum → gastrin; D cells → somatostatin; ECL cells → histamine)
- Pyloric antrum: mucous and G cells (gastrin)
Blood supply - rich anastomotic network:
- Lesser curvature: right gastric artery (from hepatic artery proper) + left gastric artery (from celiac trunk)
- Greater curvature: right gastro-omental (from gastroduodenal artery) + left gastro-omental (from splenic artery)
- Fundus: short gastric arteries (from splenic artery)
Venous drainage: Mirrors arteries; left and right gastric veins → portal vein; short gastric and left gastro-omental veins → splenic vein → portal vein
Lymphatics: Follow the arterial supply; ultimately drain into celiac lymph nodes
Innervation:
- Parasympathetic: vagus (CN X) via anterior/posterior vagal trunks - stimulates motility and secretion
- Sympathetic: T6-T9 via celiac plexus - inhibits motility, vasoconstricts
7. SMALL INTESTINE
The longest segment of the GI tract, ~6-7 meters long (cadaver measurement; contracts to ~3 m in living individuals). This is the primary site of digestion and absorption. Divided into three parts:
7a. Duodenum (~25 cm, C-shaped)
The shortest but most fixed part, wraps around the head of the pancreas. Retroperitoneal (except the first 2 cm).
Four parts:
- Superior (D1) - from pylorus, crosses L1; lies anteriorly to the common bile duct and gastroduodenal artery; the duodenal cap (first 2 cm) is intraperitoneal - site of most duodenal ulcers
- Descending (D2) - descends along right side of L1-L3; the ampulla of Vater (major duodenal papilla) receives the common bile duct and main pancreatic duct (duct of Wirsung); the minor duodenal papilla (accessory pancreatic duct of Santorini) is ~2 cm superior
- Horizontal/Inferior (D3) - crosses L3 horizontally; crossed anteriorly by the superior mesenteric vessels (SMA/SMV), creating a potential site for compression (superior mesenteric artery syndrome)
- Ascending (D4) - ascends to the left of L2, turning abruptly at the duodenojejunal flexure (ligament of Treitz) - the landmark separating upper from lower GI tract
Duodenal wall specialization: Contains Brunner's glands (submucosal mucous glands unique to duodenum) that secrete alkaline mucus to neutralize gastric acid.
Blood supply: Superior pancreaticoduodenal arteries (from gastroduodenal) + inferior pancreaticoduodenal arteries (from SMA) form anastomotic arcades around the pancreatic head.
7b. Jejunum (~2.5 m, proximal 2/5)
Begins at the duodenojejunal flexure (ligament of Treitz, at L2 level), suspended by the mesentery. Mostly in the left upper and central abdomen.
Characteristics distinguishing it from ileum:
- Thicker wall with taller, more numerous plicae circulares (valves of Kerckring) - permanent circular folds that increase surface area 3-fold
- Larger diameter lumen
- More vascular (redder color)
- Fewer lymphoid patches
- Fewer and shorter arterial arcades with longer vasa recta
- Less mesenteric fat
Primary site of carbohydrate and protein absorption; also absorbs fat, fat-soluble vitamins, and most water-soluble vitamins.
7c. Ileum (~3.5 m, distal 3/5)
Occupies the right lower quadrant; terminates at the ileocecal valve (Bauhin's valve) opening into the cecum.
Characteristics:
- Thinner wall with fewer, shorter plicae circulares
- Smaller diameter
- More mesenteric fat
- Peyer's patches (aggregated lymphoid follicles) - abundant in the anti-mesenteric wall; important for mucosal immunity
- Multiple arterial arcades (4-5 levels) with shorter vasa recta
Specialized absorption in ileum:
- Terminal ileum: vitamin B12-intrinsic factor complex (via cubilin receptors) and bile salts (enterohepatic circulation)
Small intestine surface area amplification:
- Plicae circulares: x3
- Villi: x10
- Microvilli (brush border): x20
- Total ~200-400 m² of absorptive surface
Blood supply (entire small intestine): Superior mesenteric artery (SMA) via jejunal and ileal branches forming arterial arcades → vasa recta → intestinal wall. Venous drainage via superior mesenteric vein (SMV) → portal vein.
8. LARGE INTESTINE (~1.5 m long)
Frames the small intestine from the ileocecal valve to the anus. Functions: absorb water and electrolytes, form and store feces, host gut microbiome.
Distinguishing features from small intestine:
- Taeniae coli - three longitudinal bands of condensed outer muscle running the length; they are shorter than the bowel, causing it to pucker into
- Haustra (sacculations) - pouches between the taeniae
- Omental (epiploic) appendages - fatty tags projecting from the serosal surface
- Larger diameter, fixed position (most parts)
8a. Cecum (~6 cm long)
The blind-ended pouch in the right iliac fossa; first part of the large intestine. The ileocecal valve guards the ileocecal junction, preventing backflow. The appendix (vermiform appendix) attaches to the posteromedial cecum at the convergence of the three taeniae coli.
Appendix: ~6-10 cm long; hangs into the pelvis most commonly. Has a mesentery (mesoappendix) containing the appendicular artery (from ileocolic artery). Rich in lymphoid tissue (tonsil of the abdomen). When blocked, leads to appendicitis.
McBurney's point: Located 2/3 of the way from the umbilicus to the right anterior superior iliac spine - the surface marking of the appendix base; site of maximal tenderness in appendicitis.
8b. Ascending Colon (~15 cm)
Ascends from the cecum to the right colic (hepatic) flexure in the right upper quadrant below the liver. Retroperitoneal (no mesentery). At the hepatic flexure, the colon turns left at approximately 90°.
8c. Transverse Colon (~45 cm)
Most mobile segment; suspended by the transverse mesocolon attached to the anterior border of the pancreas. Hangs across the abdomen from the right hepatic flexure to the left colic (splenic) flexure. The splenic flexure is higher and more acute than the hepatic flexure; it is tethered by the phrenocolic ligament.
The greater omentum (apron of fat) hangs from the greater curvature of the stomach and drapes over the transverse colon and small intestine, acting as a peritoneal "policeman" that walls off infection.
8d. Descending Colon (~25 cm)
Retroperitoneal; descends from the splenic flexure to the left iliac fossa, where it becomes the sigmoid colon.
8e. Sigmoid Colon (~40 cm, highly variable)
S-shaped loop with a mesentery (sigmoid mesocolon), located in the left iliac fossa and pelvis. Most mobile part of the large bowel; common site of diverticular disease due to high intraluminal pressure.
8f. Rectum (~12 cm)
Begins at S3 vertebral level where the sigmoid mesocolon ends. Retroperitoneal superiorly, then subperitoneal. Has three lateral curves creating internal mucosal folds (Houston's valves/transverse rectal folds). The rectum has no taeniae (longitudinal muscle is complete). The rectal ampulla is the dilated terminal segment that stores feces before defecation.
Peritoneal reflections around the rectum:
- Anteriorly in males: rectovesical pouch (between rectum and bladder)
- Anteriorly in females: rectouterine pouch of Douglas (between rectum and uterus) - the most dependent part of the peritoneal cavity
8g. Anal Canal (~3-4 cm)
The terminal part of the large intestine, below the pelvic floor (levator ani muscle).
Key landmarks:
- Pectinate (dentate) line - marks the transition from columnar mucosa (upper 2/3 of anal canal) to stratified squamous epithelium (lower 1/3); functionally divides the sensory innervation and lymphatic drainage
- Anal columns (of Morgagni) - longitudinal ridges of mucosa in the upper anal canal; their bases are connected by anal valves forming anal sinuses where anal glands open
- Internal anal sphincter (IAS) - thickened involuntary smooth muscle (continuation of circular muscle); always contracted at rest; responsible for ~85% of resting anal tone
- External anal sphincter (EAS) - voluntary skeletal muscle; has three parts (subcutaneous, superficial, deep); innervated by inferior rectal nerve (S2/S3) and perineal branch of S4
Blood supply:
- Superior rectal artery (from inferior mesenteric artery) - supplies upper rectum and upper anal canal
- Middle rectal arteries (from internal iliac arteries)
- Inferior rectal arteries (from internal pudendal arteries) - supply lower anal canal
Hemorrhoids: Dilated submucosal venous plexuses. Internal hemorrhoids (above pectinate line) are insensate; external hemorrhoids (below pectinate line) are painful due to somatic innervation.
Blood supply to the large intestine:
- Cecum, ascending colon, right 2/3 transverse colon: superior mesenteric artery (SMA) via ileocolic, right colic, and middle colic arteries
- Left 1/3 transverse colon, descending colon, sigmoid, rectum: inferior mesenteric artery (IMA) via left colic, sigmoid, and superior rectal arteries
- Marginal artery (of Drummond): Runs along the mesenteric border of the entire colon, anastomosing SMA and IMA territories
- Arc of Riolan (meandering mesenteric artery): Additional anastomosis between SMA and IMA in the mesentery; important collateral pathway
- Watershed areas (most vulnerable to ischemia): Splenic flexure (Griffith's point) and rectosigmoid junction (Sudeck's point)
9. ACCESSORY ORGANS OF DIGESTION
9a. Liver
The largest gland in the body (~1.5 kg); lies in the right hypochondriac and epigastric regions, protected by the lower ribs.
Lobes and surfaces:
- Anatomical lobes (by falciform ligament): right lobe (larger) and left lobe; the quadrate lobe and caudate lobe are on the visceral surface
- Functional/surgical lobes (Couinaud segments, by vascular supply): right and left functional lobes separated by the principal plane (Cantlie's line) running from the gallbladder fossa to the IVC groove. The liver is divided into 8 Couinaud segments, each with an independent vascular pedicle (portal vein, hepatic artery, bile duct) and hepatic vein drainage - allows individual segment resection
Surfaces:
- Diaphragmatic surface (anterior/superior): smooth, related to diaphragm and anterior abdominal wall; the falciform ligament attaches here, containing the ligamentum teres (obliterated umbilical vein)
- Visceral surface (posterior/inferior): has the porta hepatis ("gate of the liver") - the transverse fissure where the portal vein, hepatic artery proper, and hepatic ducts enter/leave; also has impressions for stomach, gallbladder, right kidney, right adrenal, duodenum, and colon
Ligaments of the liver:
- Falciform ligament: connects liver to anterior abdominal wall and diaphragm
- Coronary ligaments (anterior and posterior): attach liver to diaphragm; bare area between them
- Right and left triangular ligaments: lateral extensions of coronary ligaments
- Hepatoduodenal ligament (right free edge of lesser omentum): contains the portal triad - portal vein (posterior), hepatic artery proper (left), common bile duct (right) - Calot's triangle and Pringle maneuver (compression here stops hepatic blood flow)
- Hepatogastric ligament: connects liver to lesser curvature of stomach (part of lesser omentum)
Blood supply (dual):
- Portal vein (~75%): carries nutrient-rich blood from the gut and spleen; formed by SMV + splenic vein behind the neck of the pancreas
- Hepatic artery proper (~25%): carries oxygenated blood; branch of the common hepatic artery from the celiac trunk
Venous drainage: Three hepatic veins (right, middle, left) drain directly into the IVC
Bile production: Hepatocytes produce ~500-1000 mL bile/day. Bile contains bile salts, cholesterol, bilirubin, phospholipids, and water. Bile flows from hepatocytes into canaliculi → cholangioles → bile ducts within portal triads → left and right hepatic ducts → common hepatic duct → (joins cystic duct) → common bile duct → ampulla of Vater → duodenum
Hepatic microstructure:
- Hepatic acinus (functional unit): Zones 1, 2, 3 arranged around the portal triad. Zone 1 (periportal) receives highest O2; Zone 3 (centrilobular/perivenous) is most vulnerable to ischemia and alcohol damage.
- Hepatic lobule (classic unit): Hexagonal; central vein in center, portal triads at corners; hepatocyte plates radiate outward
9b. Gallbladder
A pear-shaped reservoir on the inferior surface of the right lobe of the liver, in the gallbladder fossa.
Parts:
- Fundus - rounded blind end, projects beyond the liver margin; can be palpated at the right costal margin in the midclavicular line (Murphy's sign in cholecystitis)
- Body - main part, related to the transverse colon and duodenum
- Neck - tapers into the cystic duct; may have a small pouch (Hartmann's pouch), a common site for gallstone impaction
- Cystic duct - joins the common hepatic duct to form the common bile duct (CBD); has a spiral valve of Heister internally
Capacity: ~30-50 mL
Function: Stores and concentrates bile (up to 10-fold concentration) between meals. Contracts in response to cholecystokinin (CCK) released from duodenal I cells in response to fat and protein.
Blood supply: Cystic artery (usually a branch of the right hepatic artery) within Calot's triangle (bounded by the cystic duct, common hepatic duct, and liver edge) - critical anatomy during cholecystectomy.
Common bile duct (CBD):
- Formed by union of common hepatic duct + cystic duct
- ~7-8 cm long
- Descends in the free edge of the lesser omentum (hepatoduodenal ligament) → behind duodenum → in a groove on posterior pancreatic head → unites with main pancreatic duct to form the hepatopancreatic ampulla (ampulla of Vater)
- Opens at the major duodenal papilla in D2 of duodenum
- The sphincter of Oddi surrounds the ampulla and controls flow of bile and pancreatic juice
9c. Pancreas
A retroperitoneal gland (~15-20 cm long, ~80-90 g) lying in the C-curve of the duodenum, at the level of L1-L2.
Parts:
- Head - the broad right portion nestled in the C-loop of the duodenum; the uncinate process is a tongue of tissue projecting left behind the superior mesenteric vessels; the CBD runs through or behind the head
- Neck - the narrow part anterior to the junction of the SMV and portal vein; a key landmark in pancreatic surgery
- Body - crosses the midline; the splenic vein runs along its posterior surface
- Tail - the left tapered end; lies in the splenorenal ligament and is in contact with the splenic hilum; the only truly intraperitoneal part
Duct system:
- Main pancreatic duct (Wirsung's duct): Runs the length of the pancreas, receiving tributaries; joins the CBD at the hepatopancreatic ampulla
- Accessory pancreatic duct (Santorini's duct): Drains the upper head and uncinate process; opens at the minor duodenal papilla ~2 cm proximal to the major papilla
Exocrine function (~98% of pancreatic tissue):
- Acinar cells secrete digestive enzymes: amylase (starch), lipase (fats), trypsinogen, chymotrypsinogen, proelastase (proteins - secreted as inactive zymogens), ribonuclease, DNase
- Ductal cells secrete bicarbonate-rich juice (pH 7.1-8.2) that neutralizes gastric acid in the duodenum; secretin (from duodenal S cells) stimulates this
- Trypsinogen is activated to trypsin by enterokinase (enteropeptidase) on the duodenal brush border; trypsin then activates all other proteolytic zymogens (cascade activation)
Endocrine function (Islets of Langerhans, ~2% of tissue):
- Alpha (α) cells: Glucagon (raises blood glucose)
- Beta (β) cells: Insulin (lowers blood glucose); ~70% of islet cells
- Delta (δ) cells: Somatostatin (inhibits both insulin and glucagon)
- PP cells: Pancreatic polypeptide
- Epsilon cells: Ghrelin
Blood supply: Superior pancreaticoduodenal arteries (from gastroduodenal artery/SMA) supply the head; body and tail are supplied by splenic artery branches (dorsal pancreatic artery, great pancreatic artery, caudal pancreatic artery).
Venous drainage: Into the portal/splenic veins.
10. THE ABDOMINAL CAVITY AND PERITONEUM
10a. Peritoneum
A thin serous membrane (mesothelium) lining the abdominal cavity.
- Parietal peritoneum: Lines the abdominal and pelvic walls; supplied by somatic nerves (senses sharp, well-localized pain)
- Visceral peritoneum: Covers the organs; supplied by autonomic nerves (senses dull, poorly-localized pain)
- Peritoneal cavity: The potential space between parietal and visceral layers; contains only a thin film of fluid (~100 mL) for lubrication
10b. Intraperitoneal vs. Retroperitoneal Organs
| Intraperitoneal (covered by peritoneum, mobile) | Retroperitoneal (behind peritoneum, fixed) |
|---|---|
| Stomach, spleen | Duodenum (D2, D3, D4) |
| Liver (mostly), gallbladder | Pancreas (mostly) |
| Jejunum, ileum | Ascending colon |
| Transverse colon (has mesentery) | Descending colon |
| Sigmoid colon (has mesentery) | Rectum (partly) |
| Cecum (mostly) | Kidneys, adrenal glands, aorta, IVC |
| Appendix |
Mnemonic for retroperitoneal organs: "SAD PUCKER" - Suprarenal glands, Aorta/IVC, Duodenum (2nd-4th parts), Pancreas (except tail), Ureters, Colon (ascending/descending), Kidneys, Esophagus (abdominal), Rectum (lower 2/3)
10c. Peritoneal Ligaments, Omenta, and Mesenteries
Lesser omentum: Double layer of peritoneum connecting lesser curvature of stomach and proximal duodenum to the liver:
- Hepatogastric ligament (left, larger portion)
- Hepatoduodenal ligament (right, contains portal triad: portal vein, hepatic artery, bile duct)
- Right free edge is the anterior boundary of the epiploic foramen (foramen of Winslow) - the opening into the lesser sac (omental bursa)
Greater omentum: Apron of fat hanging from the greater curvature of the stomach; fuses with the transverse mesocolon; rich in macrophages and lymphatics ("abdominal policeman" - walls off infections like perforated appendix)
Epiploic foramen (foramen of Winslow): Communicates the greater sac with the lesser sac (omental bursa); bounded anteriorly by hepatoduodenal ligament, posteriorly by IVC, superiorly by caudate lobe of liver, inferiorly by D1 duodenum
Mesentery (of the small bowel): Fan-shaped double fold of peritoneum from the root of the mesentery (runs from the duodenojejunal flexure at L2 to the ileocecal junction at the right sacroiliac joint, ~15 cm long) containing the jejunal/ileal branches of SMA, SMV, lymphatics, and autonomic nerves
Transverse mesocolon: Suspends transverse colon from anterior border of pancreas
Sigmoid mesocolon: Inverted V-shaped attachment to posterior pelvic wall
10d. Abdominal Regions
The abdomen is divided into 9 regions by two horizontal planes (subcostal and transtubercular/intertubercular) and two vertical planes (midclavicular):
| Right hypochondriac | Epigastric | Left hypochondriac |
|---|---|---|
| Right liver, gallbladder, right kidney, hepatic flexure | Liver (left lobe), stomach, pancreas (head), spleen | Stomach fundus, spleen, left kidney, splenic flexure |
| Right lumbar | Umbilical | Left lumbar |
| Ascending colon, right kidney | Small bowel, transverse colon, aorta | Descending colon, left kidney |
| Right iliac fossa | Hypogastric (pubic) | Left iliac fossa |
| Cecum, appendix, right ovary/tube | Bladder, uterus, sigmoid colon | Sigmoid colon, left ovary/tube |
Alternatively, 4 clinical quadrants: RUQ, LUQ, RLQ, LLQ.
11. WALL LAYERS OF THE GI TRACT (General Plan)
All parts of the GI tract share a common wall plan (from lumen outward):
- Mucosa (innermost):
- Epithelium - varies by region (squamous in esophagus/anal canal; simple columnar with villi in small bowel)
- Lamina propria - loose connective tissue with capillaries, lymphatics (lacteals in small bowel), plasma cells, lymphocytes
- Muscularis mucosae - thin smooth muscle layer; creates local folds
- Submucosa:
- Dense connective tissue; contains blood vessels, lymphatics, Meissner's (submucosal) nerve plexus (controls secretion)
- Brunner's glands in duodenum only
- Lymphoid follicles/Peyer's patches in ileum
- Muscularis externa:
- Inner circular muscle layer
- Auerbach's (myenteric) nerve plexus between the two muscle layers (controls motility)
- Outer longitudinal muscle layer
- Exception: stomach has an additional inner oblique layer
- Serosa or Adventitia (outermost):
- Serosa = visceral peritoneum (intraperitoneal organs)
- Adventitia = connective tissue without peritoneum (retroperitoneal organs, esophagus)
Enteric Nervous System
The "gut brain" - contains ~100 million neurons in two plexuses:
- Meissner's submucosal plexus: Controls secretion and mucosal blood flow
- Auerbach's myenteric plexus: Controls motility (peristalsis, segmentation)
12. KEY BLOOD SUPPLY SUMMARY
| Artery | Origin | Territory |
|---|---|---|
| Left gastric artery | Celiac trunk (direct) | Lesser curvature of stomach (left), distal esophagus |
| Common hepatic artery | Celiac trunk | Liver (hepatic artery proper), duodenum (gastroduodenal artery), stomach (right gastric, right gastro-omental) |
| Splenic artery | Celiac trunk | Spleen, pancreas (body/tail), stomach (short gastric, left gastro-omental) |
| Superior mesenteric artery (SMA) | Aorta at L1 | Duodenum (distal), jejunum, ileum, cecum, appendix, ascending colon, right 2/3 transverse colon |
| Inferior mesenteric artery (IMA) | Aorta at L3 | Left 1/3 transverse colon, descending colon, sigmoid, upper rectum |
Celiac Trunk (T12-L1): "Foregut artery"
Supplies derivatives of the embryological foregut (esophagus [lower], stomach, duodenum [proximal], liver, gallbladder, pancreas, spleen).
SMA (L1): "Midgut artery"
Supplies midgut derivatives (distal duodenum to mid-transverse colon).
IMA (L3): "Hindgut artery"
Supplies hindgut derivatives (mid-transverse colon to upper anal canal).
13. PORTAL VENOUS SYSTEM
The portal vein carries nutrient-rich blood from the GI tract and spleen to the liver before returning to systemic circulation. Formed by:
- SMV + Splenic vein → portal vein (behind the neck of the pancreas, at L2)
- Portal vein enters the liver via the porta hepatis, dividing into right and left branches
Porto-systemic anastomoses (clinically important in portal hypertension - varices form here):
- Lower esophagus: Left gastric vein (portal) ↔ azygos/hemiazygos veins (systemic) → esophageal varices
- Umbilicus: Paraumbilical veins (portal) ↔ epigastric veins (systemic) → caput medusae
- Rectum/anal canal: Superior rectal (portal via IMA) ↔ middle/inferior rectal (systemic via iliac) → rectal varices
- Retroperitoneum: Veins of Retzius (portal) ↔ posterior abdominal wall veins (systemic)
Summary Table: All Digestive System Organs
| Organ | Location | Primary Function | Key Feature |
|---|---|---|---|
| Oral cavity | Head | Mechanical + initial chemical digestion | Salivary amylase, bolus formation |
| Parotid gland | Preauricular | Serous saliva (amylase-rich) | Stensen's duct opens at upper 2nd molar |
| Submandibular gland | Below mandible | Mixed serous + mucous saliva | Wharton's duct, largest saliva output |
| Sublingual gland | Floor of mouth | Mostly mucous saliva | Multiple Rivinus ducts |
| Pharynx | Neck | Swallowing conduit | 3 parts; complex deglutition reflex |
| Esophagus | Neck to abdomen | Peristaltic transport | 4 constrictions; LES prevents reflux |
| Stomach | LUQ | Protein digestion, HCl, bolus churning | 3 muscle layers; rugae; intrinsic factor |
| Duodenum | Retroperitoneal | Bile + pancreatic enzyme mixing | Ampulla of Vater; Brunner's glands |
| Jejunum | Central abdomen | Carbohydrate/protein/fat absorption | Tall plicae; richly vascular |
| Ileum | RLQ | Continued absorption; B12 + bile salts | Peyer's patches; ileocecal valve |
| Cecum + Appendix | RIF | Transition zone; lymphoid organ | McBurney's point |
| Colon | Peripheral | Water absorption; feces formation | Taeniae coli, haustra |
| Rectum | Pelvis | Feces storage | Rectal ampulla; Houston's valves |
| Anal canal | Perineum | Controlled defecation | Pectinate line; dual sphincters |
| Liver | RUQ | Bile production, metabolism, detoxification | 8 Couinaud segments; dual blood supply |
| Gallbladder | Liver undersurface | Bile storage and concentration | Hartmann's pouch; Calot's triangle |
| Pancreas | Retroperitoneal L1-L2 | Exocrine enzymes + endocrine hormones | Ampulla of Vater; islets of Langerhans |
Sources: Gray's Anatomy for Students (9780323934237), Guyton and Hall Textbook of Medical Physiology, Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Yamada's Textbook of Gastroenterology
This is a shared conversation. Sign in to Orris to start your own chat.