Write a post graduate question on Strain replacement theory related to dental caries. you can take information from pubmed indexed articles and give me references
strain replacement theory dental caries Streptococcus mutans
Streptococcus mutans replacement therapy dental caries prevention
bacterial strain replacement caries Streptococcus mutans
PMID: 3326613
PMID: 12369203
PMID: 17448156
PMID: 27616834
PMID: 12727383
Postgraduate Question: Strain Replacement Therapy and Dental Caries
Long Essay Question (20 Marks)
Model Answer / Examiner's Key Points
(a) Definition and Theoretical Basis (4 marks)
- Infectious etiology of dental caries: Dental caries is a transmissible, bacterially mediated disease in which Streptococcus mutans is the primary etiological agent. Its acquisition follows a definable window of infectivity in early childhood.
- Ecological competition within biofilms: Members of the indigenous oral microflora actively compete for colonization sites and nutrients. Bacteria produce bacteriocins (e.g., mutacins) that inhibit competing strains - a phenomenon known as antibiosis. This natural antagonism can be exploited therapeutically.
- Colonization resistance: Once a strain occupies an ecological niche, it is difficult for a competing strain to displace it. A pre-established, benign effector strain can therefore block the subsequent establishment of pathogenic strains.
(b) Construction of BCS3-L1 and A2JM (6 marks)
| Modification | Gene Targeted | Rationale |
|---|---|---|
| Deletion of lactate dehydrogenase (LDH) gene | ldh | Completely abrogates lactic acid production, eliminating the primary mechanism of enamel demineralization. The strain retains the ability to colonize but cannot acidify the plaque environment. |
| Upregulation of mutacin 1140 production | Mutacin structural genes | Mutacin 1140 is a novel lantibiotic peptide antibiotic. Elevated production gives BCS3-L1 a strong competitive advantage over wild-type S. mutans strains in the same niche. |
- Genetically stable over prolonged colonization
- Non-cariogenic in gnotobiotic rats (significantly less cariogenic than wild-type)
- Capable of displacing indigenous S. mutans after a single topical application
| Additional Modification | Gene | Purpose |
|---|---|---|
| Deletion of d-alanine biosynthesis gene | dal | Creates auxotrophy for d-alanine; the strain requires exogenous d-alanine to survive, allowing rapid eradication with chlorhexidine by depleting the oral bacterial reservoir if adverse effects occur. |
| Deletion of genetic transformation gene | comE | Reduces horizontal gene transfer competence, limiting the possibility of the engineered genetic material spreading to other oral bacteria and increasing genetic containment. |
(c) Properties of an Ideal Effector Strain (4 marks)
- Competitive colonization ability: The strain must be capable of establishing itself in the complex oral biofilm environment and persisting long-term after a single or limited application.
- Production of a potent, narrow-spectrum bacteriocin: It must produce an antibiotic (such as mutacin 1140) that specifically disadvantages the target pathogen (S. mutans) without broadly disrupting the commensal oral microbiome.
- Elimination of virulence factor(s): The cariogenic determinant (lactic acid production via LDH) must be deleted while retaining all colonization-related properties (adhesins, glucosyltransferases for biofilm formation).
- Genetic stability: The modifications must not revert to wild-type under in vivo selection pressures.
- Safety and containment: An ideal strain incorporates a "kill-switch" mechanism (auxotrophy, antibiotic sensitivity) that allows its eradication in the event of unexpected side effects, as exemplified by the dal deletion in A2JM.
- Lack of horizontal gene transfer: Reduced genetic transformability to prevent spread of engineered sequences to other oral microorganisms.
(d) Limitations, Biosafety, and Ethical Considerations (4 marks)
- Although comE deletion reduces competence, horizontal gene transfer cannot be entirely excluded. Spread of mutacin 1140 overproduction genes to other oral streptococci could alter the oral microbiome unpredictably.
- Auxotrophic strains can scavenge d-alanine from surrounding plaque bacteria, reducing the effectiveness of the kill-switch (demonstrated in the A2JM animal model).
- Long-term colonization effects on the broader oral and systemic microbiome remain incompletely characterized.
- The window of infectivity concept implies that treatment must be timed during early childhood, before indigenous S. mutans becomes established.
- The current strain targets only S. mutans, but other mutans streptococci (e.g., S. sobrinus) also contribute to caries.
- No large-scale human RCTs have been published to date confirming long-term safety or efficacy.
- Deliberate introduction of a live genetically modified organism (GMO) into the human oral cavity raises regulatory and bioethical questions regarding informed consent, especially in pediatric populations.
- Long-term ecological consequences of permanently displacing wild-type strains in a community setting are unknown.
- Public acceptance of "GMO bacteria" as a dental preventive measure may be limited.
(e) Comparison with Probiotic-Based Approaches (2 marks)
| Feature | Strain Replacement Therapy | Probiotic Therapy |
|---|---|---|
| Organism type | Genetically engineered effector strain | Wild-type or naturally selected bacteria (e.g., Lactobacillus, S. salivarius) |
| Permanence | Designed for permanent, single-application colonization | Requires repeated administration; transient colonization |
| Specificity | Highly specific (targets S. mutans niche via mutacin) | Indirect competition; broad spectrum |
| Regulatory path | Requires GMO approval; stringent clinical trials | Generally regarded as safe (GRAS); simpler approval |
| Mechanism | Competitive displacement + bacteriocin production | Competitive exclusion, immune modulation, lowered pH tolerance |
| Scope of disease | Dental caries specifically | Caries, periodontitis, and some systemic effects |
References (PubMed Indexed)
-
Hillman JD, Socransky SS. Replacement therapy of the prevention of dental disease. Adv Dent Res. 1987 Oct;1(1):119-25. PMID: 3326613
-
Hillman JD. Genetically modified Streptococcus mutans for the prevention of dental caries. Antonie Van Leeuwenhoek. 2002 Aug;82(1-4):361-6. PMID: 12369203
-
Tagg JR, Dierksen KP. Bacterial replacement therapy: adapting 'germ warfare' to infection prevention. Trends Biotechnol. 2003 May;21(5):217-23. PMID: 12727383
-
Hillman JD, Mo J, McDonell E, Cvitkovitch D, Hillman CH. Modification of an effector strain for replacement therapy of dental caries to enable clinical safety trials. J Appl Microbiol. 2007 May;102(5):1209-19. PMID: 17448156
-
Gupta S, Marwah N. 'Use a Thorn to Draw Thorn' Replacement Therapy for Prevention of Dental Caries. Int J Clin Pediatr Dent. 2010 Sep-Dec;3(3):157-62. PMC4993818. PMID: 27616834
write an answer for the exam
EXAM ANSWER
"Strain Replacement Therapy as a Paradigm Shift in Dental Caries Prevention"
(a) Definition and Theoretical Basis
(b) Construction of BCS3-L1 and Its Clinical Modification A2JM
(c) Properties of an Ideal Effector Strain
(d) Limitations, Biosafety, and Ethical Considerations
(e) Comparison with Probiotic-Based Approaches
References
-
Hillman JD, Socransky SS. Replacement therapy of the prevention of dental disease. Adv Dent Res. 1987;1(1):119-25. PMID: 3326613
-
Hillman JD. Genetically modified Streptococcus mutans for the prevention of dental caries. Antonie Van Leeuwenhoek. 2002;82(1-4):361-6. PMID: 12369203
-
Tagg JR, Dierksen KP. Bacterial replacement therapy: adapting 'germ warfare' to infection prevention. Trends Biotechnol. 2003;21(5):217-23. PMID: 12727383
-
Hillman JD, Mo J, McDonell E, Cvitkovitch D, Hillman CH. Modification of an effector strain for replacement therapy of dental caries to enable clinical safety trials. J Appl Microbiol. 2007;102(5):1209-19. PMID: 17448156
-
Gupta S, Marwah N. 'Use a Thorn to Draw Thorn' Replacement Therapy for Prevention of Dental Caries. Int J Clin Pediatr Dent. 2010;3(3):157-62. PMID: 27616834
add a flowchart explaining the mechanism
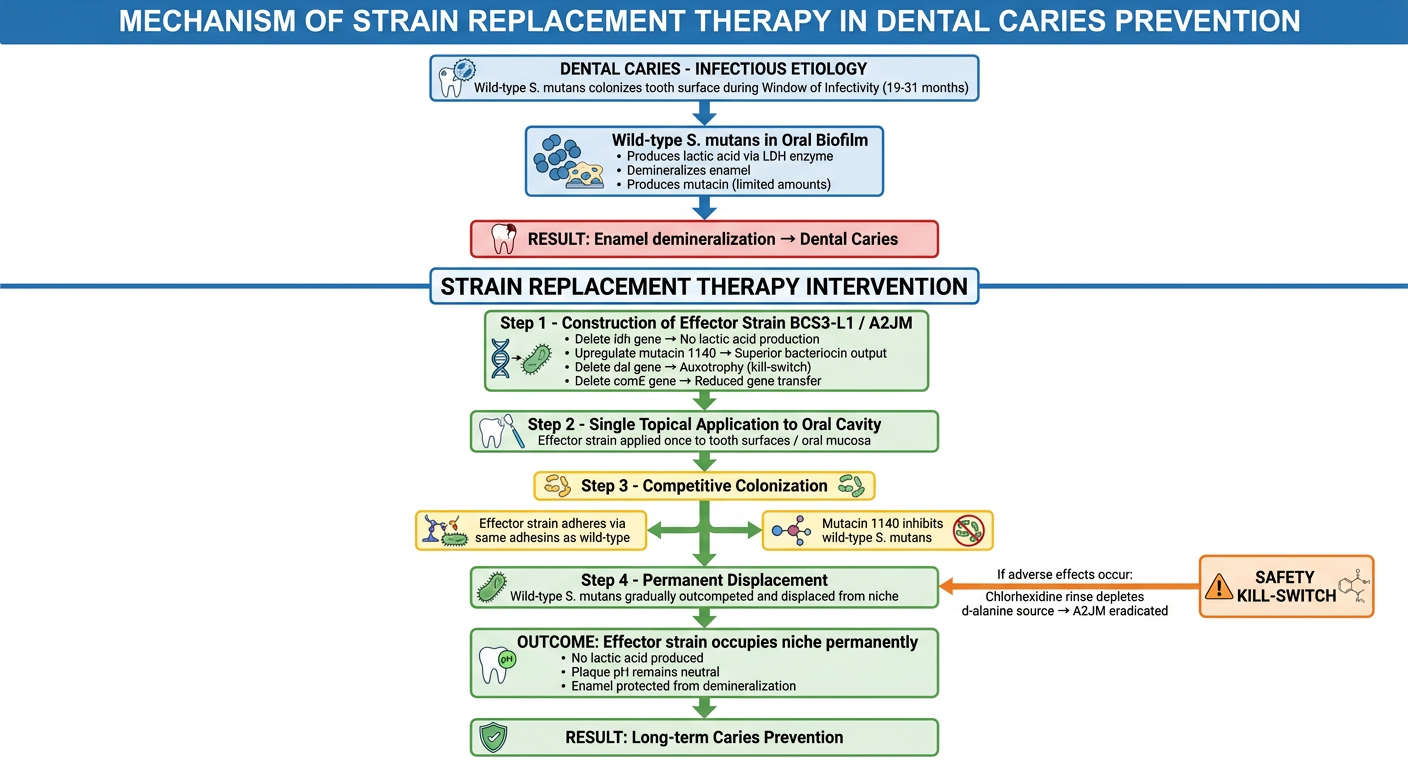
A detailed, clean medical/scientific flowchart titled "Mechanism of Strain Replacement Therapy in Dental Caries Prevention". The flowchart should have a vertical flow with clearly labeled boxes and arrows, on a white background with professional dental/microbiology styling. Include the following sequential steps with connecting arrows: 1. TOP BOX (blue header): "DENTAL CARIES - INFECTIOUS ETIOLOGY" with subtext "Wild-type S. mutans colonizes tooth surface during Window of Infectivity (19-31 months)" 2. Arrow down to: "Wild-type S. mutans in Oral Biofilm" with bullet points: "Produces lactic acid via LDH enzyme", "Demineralizes enamel", "Produces mutacin (limited amounts)" 3. Arrow down to a RED decision/problem box: "RESULT: Enamel demineralization → Dental Caries" 4. Then a large horizontal dividing line labeled "STRAIN REPLACEMENT THERAPY INTERVENTION" 5. Arrow down to a GREEN box: "Step 1 - Construction of Effector Strain BCS3-L1 / A2JM" with bullet points listing: "Delete ldh gene → No lactic acid production", "Upregulate mutacin 1140 → Superior bacteriocin output", "Delete dal gene → Auxotrophy (kill-switch)", "Delete comE gene → Reduced gene transfer" 6. Arrow down to: "Step 2 - Single Topical Application to Oral Cavity" with subtext "Effector strain applied once to tooth surfaces / oral mucosa" 7. Arrow down to a YELLOW box: "Step 3 - Competitive Colonization" with two branches: - Left branch: "Effector strain adheres via same adhesins as wild-type" - Right branch: "Mutacin 1140 inhibits wild-type S. mutans" Both arrows merge back down 8. Arrow down to: "Step 4 - Permanent Displacement" with subtext "Wild-type S. mutans gradually outcompeted and displaced from niche" 9. Arrow down to a GREEN result box: "OUTCOME: Effector strain occupies niche permanently" with bullet points: "No lactic acid produced", "Plaque pH remains neutral", "Enamel protected from demineralization" 10. BOTTOM GREEN box: "RESULT: Long-term Caries Prevention" 11. A separate side box in orange labeled "SAFETY KILL-SWITCH" with arrow pointing to the permanent displacement box: "If adverse effects occur: Chlorhexidine rinse depletes d-alanine source → A2JM eradicated" Use color coding: blue for normal biology, red for disease, green for therapeutic benefit, yellow for process steps, orange for safety. Include small icons of bacteria, teeth, and DNA where appropriate. Make text clearly readable.
-
Disease context - Wild-type S. mutans establishes during the window of infectivity and produces lactic acid via LDH, driving enamel demineralization.
-
Genetic engineering - BCS3-L1/A2JM is constructed with four key mutations: ldh deletion (no acid), mutacin 1140 upregulation (competitive weapon), dal deletion (kill-switch), and comE deletion (gene transfer block).
-
Single application - The effector strain is applied topically once to the oral cavity.
-
Competitive displacement - The effector strain colonizes the same niche using identical adhesion machinery, while mutacin 1140 suppresses wild-type S. mutans.
-
Permanent protection - The niche is permanently occupied by a non-acidogenic strain, maintaining neutral plaque pH and preventing enamel demineralization. The orange safety kill-switch pathway shows how chlorhexidine can eradicate A2JM if needed by depleting its d-alanine source.