Polycystic kidney disease pathology slide
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have all the key images and pathology descriptions needed. Let me compile the comprehensive answer.
Polycystic Kidney Disease - Pathology
Gross Pathology
Fig. 46.8 - Greatly enlarged polycystic kidneys from ADPKD compared with a normal kidney (middle):

Fig. 12.23 (Robbins) - ADPKD (A,B) and ARPKD (C) and associated liver cysts (D):
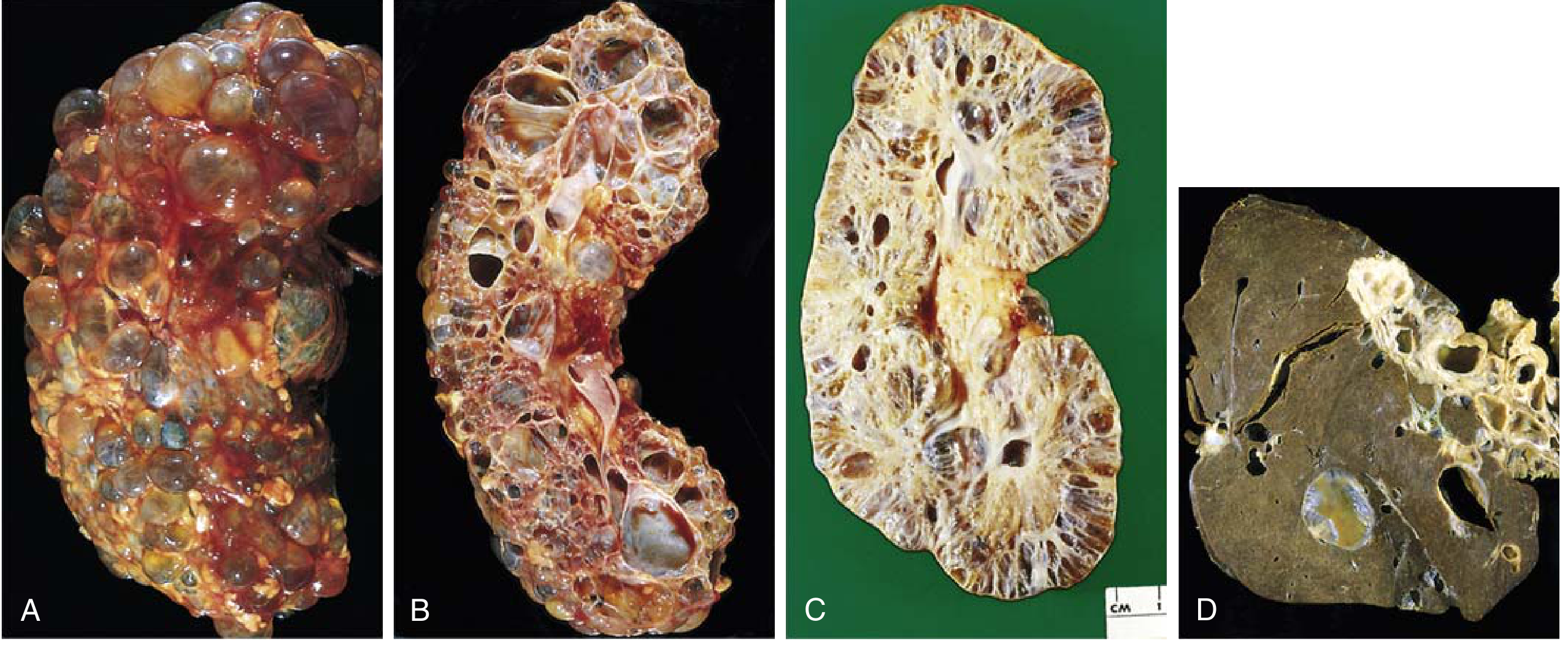
Gross features of ADPKD:
- Both kidneys reach enormous size - weights up to 4 kg each
- On cut section: innumerable spherical cysts up to 3-4 cm in diameter distributed evenly between cortex and medulla
- Cysts contain fluid that is clear, turbid, or hemorrhagic (dark brown/green = old blood)
- Normal intervening parenchyma is essentially absent in end-stage disease
- Fibrous bands encapsulate cysts on cut surface; fibrous tissue plasters the capsule
Gross features of ARPKD:
- Smaller cysts giving a sponge-like appearance
- Dilated, elongated channels oriented at right angles to the cortical surface, replacing cortex and medulla uniformly
- Invariably bilateral
Histology / Microscopic Pathology
Fig. 46.9 - H&E histology of ADPKD cysts (x200):
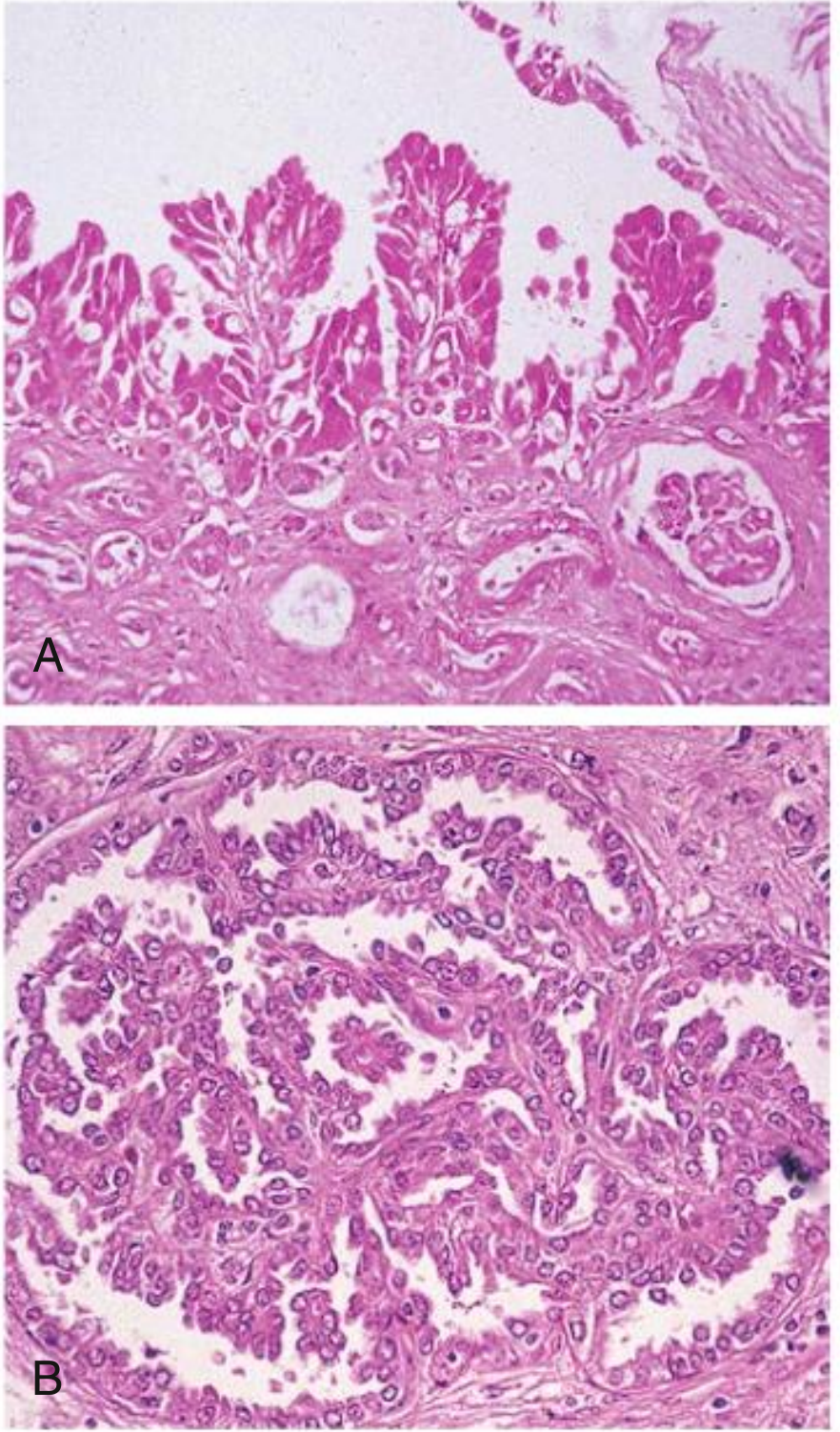
Key histologic features of ADPKD cysts:
- Cysts arise from any nephron segment (tubules and collecting ducts); most studies indicate predominantly distal nephron and collecting duct origin
- Cyst lining is variable and often atrophic (flattened cuboidal epithelium)
- Hyperplastic changes are characteristic:
- (A) Papillary hyperplasia of cyst epithelium - frond-like projections into the cyst lumen
- (B) Papillary microscopic adenomas form within the cyst wall
- Occasionally, Bowman's capsule gives rise to cysts - in these, glomerular tufts can be seen within the cystic space
- Even in early disease with normal GFR: interstitial fibrosis, pre-glomerular vascular sclerosis (afferent arterioles + interlobular arteries), and macrophage/lymphocyte interstitial infiltrate
- End-stage: tubulointerstitial fibrosis and arteriolar sclerosis are cardinal features; scant normal parenchyma in isolated patches
Fig. 45.6 (Brenner & Rector) - Scanning electron micrographs of ADPKD cyst epithelium:
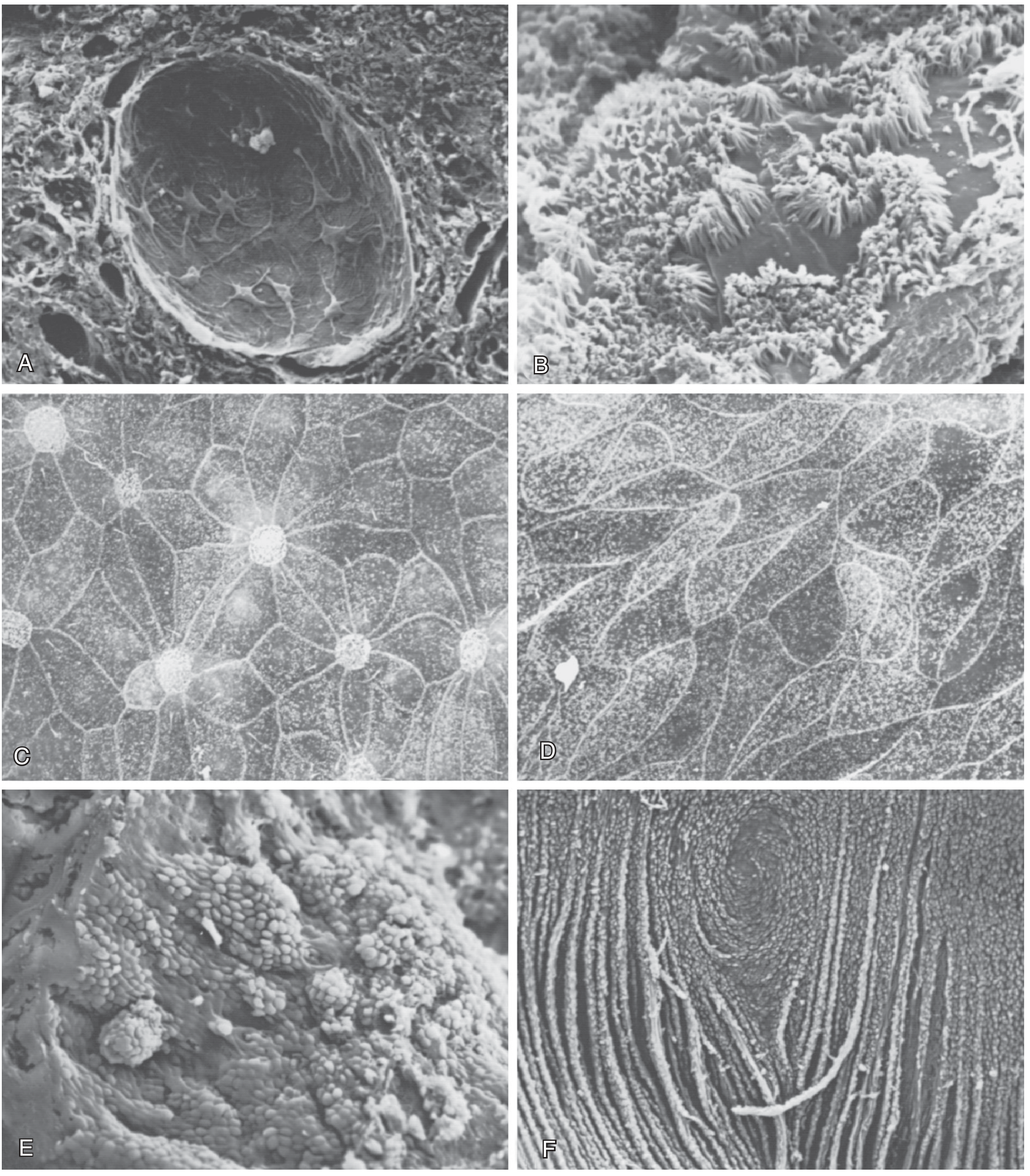
The 6 SEM panels show the diverse origin of cysts - epithelia morphologically resembling: (A) glomerular visceral layer, (B) proximal tubule brush border, (C) thick ascending limb, (D) distal tubule, (E) collecting duct principal cells, (F) medullary collecting duct. This variability confirms cysts arise from all nephron segments.
ARPKD histology:
- Uniform lining of cuboidal cells (reflects collecting tubule origin throughout)
- Uniformly small cysts; elongated channels perpendicular to cortical surface
- Associated liver findings: multiple epithelium-lined hepatic cysts + portal bile duct proliferation (congenital hepatic fibrosis)
Pathogenesis Summary
| Feature | ADPKD | ARPKD |
|---|---|---|
| Gene | PKD1 (chr 16p) ~85%; PKD2 (chr 4q) ~15% | PKHD1 |
| Protein | Polycystin-1 / Polycystin-2 | Fibrocystin |
| Location | Primary cilia (TRP channel complex) | Primary cilia |
| Mechanism | "Two-hit": somatic loss of second allele → loss of mechanosensing → ↑ proliferation, ↑ fluid secretion, ↓ calcium signaling, ↑ cAMP | Loss of fibrocystin → collecting duct dilatation |
| Prevalence | 1:400-1000 | 1:20,000 |
| Age at presentation | 4th-5th decade | Perinatal/neonatal |
The underlying defect is a ciliopathy - the polycystins (PC1 and PC2) reside in the primary cilia of tubular epithelial cells and sense fluid flow. Loss of PC1 function below a critical threshold disrupts calcium influx and planar polarity, triggering cyst expansion through increased mTOR/cAMP signaling.
Sources: Robbins & Kumar Basic Pathology, p. 525-526 | Comprehensive Clinical Nephrology, 7th Ed., p. 653-660 | Brenner and Rector's The Kidney, p. 1985-1988
This is a shared conversation. Sign in to Orris to start your own chat.