Diabetes mellitus in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information from multiple authoritative textbooks. Let me compile the complete, detailed response.
Diabetes Mellitus - A Comprehensive Overview
1. Definition and Overview
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The chronic hyperglycemia of diabetes is associated with long-term damage, dysfunction, and failure of various organs - especially the eyes, kidneys, nerves, heart, and blood vessels.
- Tietz Textbook of Laboratory Medicine, 7th Edition
2. Classification (ADA)
The American Diabetes Association (ADA) recognizes four major clinical types:
| Type | Mechanism |
|---|---|
| Type 1 DM (T1DM) | Autoimmune beta-cell destruction → absolute insulin deficiency |
| Type 2 DM (T2DM) | Progressive beta-cell failure on a background of insulin resistance |
| Gestational DM (GDM) | Diabetes first diagnosed during pregnancy, not clearly pre-existing |
| Other specific types | Monogenic (MODY, neonatal DM), exocrine pancreatic disease (cystic fibrosis), drug-induced (glucocorticoids, HIV therapy, post-transplant) |
Historical nomenclature (IDDM/NIDDM; juvenile-onset/adult-onset) was formally abolished in the 1997 ADA reclassification.
- Creasy & Resnik's Maternal-Fetal Medicine, Tietz Textbook of Laboratory Medicine, 7th Edition
3. Epidemiology
-
T2DM accounts for approximately 90% of all diabetes cases worldwide
-
T1DM represents 5-10% of all cases
-
The global burden is rising steeply - IDF projects hundreds of millions affected through 2040, with the Western Pacific, Southeast Asia, and North America/Caribbean regions carrying the highest loads
-
Incidence of T1DM is increasing particularly among children under age 5
-
Creasy & Resnik's Maternal-Fetal Medicine; Mulholland & Greenfield's Surgery, 7e
4. Pathophysiology
Type 1 Diabetes Mellitus
T1DM is a chronic autoimmune disease in which T-lymphocyte-mediated destruction of pancreatic beta cells (insulitis) leads to absolute insulin deficiency. Key features:
-
Genetic susceptibility: Over 60 loci identified; HLA region genes (especially antigen-presenting molecules) confer the greatest genetic risk. Concordance in monozygotic twins is less than 100%, confirming that environment also matters.
-
Autoimmune markers: Islet cell autoantibodies, anti-insulin antibodies, anti-GAD65 antibodies, anti-IA-2 (tyrosine phosphatase) antibodies
-
Environmental triggers: Enteroviruses are strongly implicated epidemiologically. Cow's milk exposure has been debated but not confirmed in clinical trials.
-
Natural history: In genetically at-risk individuals, two or more diabetes-related autoantibodies confer ~75% risk of T1DM over 10 years and near-certain risk over 20 years
-
New therapy: Teplizumab, a monoclonal antibody that reduces CD8+ T-lymphocyte action on beta cells, has shown significant delay in T1DM onset in at-risk individuals
-
Mulholland & Greenfield's Surgery, 7e; Creasy & Resnik's Maternal-Fetal Medicine
Type 2 Diabetes Mellitus
T2DM involves two major pathological defects that interact:
-
Insulin resistance - decreased biological response to normal circulating insulin concentrations in peripheral tissues (muscle, liver, adipose). Insulin resistance is thought by many to be the primary underlying defect, preceding clinical diabetes by up to 20 years. It is driven by:
- Visceral adiposity
- Systemic inflammation (elevated IL-6, TNF-alpha)
- Lipotoxicity from elevated free fatty acids
- Genetic polymorphisms
-
Beta-cell dysfunction - initially, beta cells hypersecrete insulin to compensate for resistance. Over time, glucotoxicity and lipotoxicity cause progressive loss of glucose-induced insulin release ("selective glucose unresponsiveness"), reduced beta-cell mass, disrupted pulsatile insulin release, and an increased proinsulin:insulin ratio.
Result: relative insulin deficiency early in disease → absolute deficiency late in disease.
Additional causes of insulin resistance include: PCOS (~80% of affected women), Cushing syndrome, acromegaly, lipodystrophy, hemochromatosis, mutations in the insulin receptor or PPARγ, and pregnancy.
- Tietz Textbook of Laboratory Medicine, 7th Edition; Guyton & Hall Medical Physiology; Mulholland & Greenfield's Surgery, 7e
5. Diagnosis
Current ADA Criteria (Box 47.3) - any one of the following is diagnostic:
| Criterion | Threshold |
|---|---|
| HbA1c | ≥ 6.5% (≥ 48 mmol/mol) |
| Fasting Plasma Glucose (FPG) | ≥ 126 mg/dL (≥ 7.0 mmol/L)* |
| 2-hour plasma glucose during 75g OGTT | ≥ 200 mg/dL (≥ 11.1 mmol/L) |
| Random plasma glucose | ≥ 200 mg/dL with classic symptoms |
*After ≥8 hours fasting. In the absence of hyperglycemic crisis, diagnosis requires confirmation with a second test.
Key historical evolution:
- Pre-1997: FPG threshold was ≥140 mg/dL (7.8 mmol/L)
- 1997: Lowered to ≥126 mg/dL (7.0 mmol/L) for earlier detection of retinopathy/nephropathy risk
- 2009: HbA1c ≥6.5% added as a diagnostic criterion (endorsed by ADA, WHO, IDF)
Prediabetes: HbA1c 5.7-6.4% (39-46 mmol/mol) OR FPG 100-125 mg/dL (impaired fasting glucose) OR 2-h OGTT 140-199 mg/dL (impaired glucose tolerance)
- Tietz Textbook of Laboratory Medicine, 7th Edition
6. Clinical Features
Type 1 DM - Usually abrupt onset:
- Polyuria, polydipsia, polyphagia
- Rapid, unexplained weight loss
- Fatigue and weakness
- Diabetic ketoacidosis (DKA) may be the presenting event
- Typically younger age of onset
Type 2 DM - Often insidious onset:
-
Many patients are asymptomatic at diagnosis; discovered incidentally
-
May have classic symptoms (polyuria, polydipsia)
-
Recurrent infections (skin, urinary tract, candidiasis)
-
Blurred vision
-
Many patients already have irreversible complications at the time of first diagnosis
-
Tietz Textbook of Laboratory Medicine, 7th Edition
7. Chronic Complications
Microvascular Complications (directly caused by hyperglycemia)
A. Diabetic Retinopathy (DR)
- Leading preventable cause of blindness; 5th leading cause of severe vision loss worldwide
- Classification:
- Preproliferative: microaneurysms, retinal infarcts (cotton-wool spots), lipid exudates, microhemorrhages ± macular edema
- Proliferative: new vessel formation (neovascularization), especially near the optic disk
- Other ocular complications: cataracts, glaucoma, optic neuropathy, extraocular muscle paresis
- Treatment: glycemic control, BP control (ACE inhibitor/ARB), fenofibrate for hyperlipidemia; laser photocoagulation for proliferative disease; anti-VEGF agents (intravitreal injections) for macular edema - superior to laser for preserving vision; vitrectomy for vitreous hemorrhage or retinal detachment
- Intensive glycemic control (HbA1c <7%) reduced retinopathy progression by 76% in the DCCT (Diabetes Control and Complications Trial)
B. Diabetic Nephropathy
- 20-40% of patients with either T1DM or T2DM develop clinically evident nephropathy
- Leading cause of end-stage renal disease (ESRD) in the United States
- Associated with ~15-year reduction in life expectancy
- Screening: Annual urine albumin-to-creatinine ratio (ACR); normal <30 mg/g; albuminuria ≥30 mg/g is the earliest marker. Begins in T1DM after 5 years of diagnosis; at diagnosis for T2DM.
- Risk factors: poor glycemic control, hypertension, smoking, obesity
- Treatment:
- ACE inhibitors or ARBs as first-line antihypertensive (also renoprotective)
- BP target: <130/80 mmHg
- SGLT2 inhibitors (empagliflozin, canagliflozin) reduce CKD progression independently of glucose control
- Finerenone (nonsteroidal MRA) reduces CKD progression and CV events in T2DM + CKD
- Dietary protein: 0.8 g/kg/d (based on ideal body weight)
C. Diabetic Neuropathy
-
Classification:
- Subclinical (detected only by electrodiagnostic/quantitative sensory testing)
- Diffuse symmetrical polyneuropathy (distal sensorimotor ± autonomic)
- Focal syndromes (mononeuropathy, cranial nerve palsies, radiculopathy)
-
Distal symmetric polyneuropathy (DPN) is the most common neuropathy in developed countries, accounts for more hospitalizations than all other diabetic complications combined, and is responsible for 50-75% of non-traumatic amputations
-
Screening: Annual foot examination; 10g monofilament, 128Hz tuning fork, pinprick, temperature sensation
-
Treatment of painful neuropathy:
- Tricyclic antidepressants (amitriptyline 10-150 mg at bedtime)
- Anticonvulsants: gabapentin (900-3600 mg/d), pregabalin (150-300 mg/d), carbamazepine
- Topical capsaicin (0.075%)
- Alpha-lipoic acid (600 mg tid); vitamin B12 supplementation if deficient
-
Autonomic neuropathy: orthostatic hypotension, gastroparesis (metoclopramide, erythromycin), erectile dysfunction, bladder dysfunction
Macrovascular Complications
-
Atherosclerotic cardiovascular disease (ASCVD): coronary artery disease, stroke, peripheral arterial disease
-
T2DM carries a cardiovascular risk equivalent to having had a prior MI in non-diabetic patients (Haffner et al., NEJM 1998)
-
Metabolic syndrome (hypertension, dyslipidemia, obesity, insulin resistance) amplifies cardiovascular risk dramatically
-
Washington Manual of Medical Therapeutics; Goodman & Gilman's Pharmacological Basis of Therapeutics; Tietz Textbook of Laboratory Medicine, 7th Edition
8. Acute Complications
| Complication | Mainly in | Key Features |
|---|---|---|
| Diabetic Ketoacidosis (DKA) | T1DM (also T2DM under stress) | Absolute insulin deficiency → ketone production → anion gap metabolic acidosis; Kussmaul breathing, fruity breath, vomiting |
| Hyperosmolar Hyperglycemic State (HHS) | T2DM | Extreme hyperglycemia (>600 mg/dL), severe dehydration, hyperosmolarity, no/minimal ketosis |
| Hypoglycemia | Both (iatrogenic, mainly with insulin/sulfonylureas) | Glucose <70 mg/dL; sweating, tremor, confusion, loss of consciousness |
9. Management
Lifestyle Modification (for all types)
- Medical nutrition therapy (individualized diet)
- Regular physical activity (150 min/week moderate aerobic)
- Weight management (especially T2DM)
- Smoking cessation
Type 1 DM Management
- Insulin is mandatory - either multiple daily injections (MDI) or continuous subcutaneous insulin infusion (CSII/pump)
- Rapid-acting insulin for meals + long-acting basal insulin (basal-bolus regimen)
- Continuous glucose monitoring (CGM)
- Carbohydrate counting
Type 2 DM Pharmacological Algorithm
Step 1 - First line: Metformin + lifestyle modification (unless contraindicated)
- Mechanism: reduces hepatic glucose output, improves insulin sensitivity
- Contraindicated: eGFR <30 mL/min/1.73 m² (risk of lactic acidosis)
Step 2 - Add second agent (if A1c not at target within 2-3 months):
| Drug Class | Key Agents | Clinical Advantage |
|---|---|---|
| GLP-1 receptor agonists | Semaglutide, liraglutide, dulaglutide | CV benefit, weight loss; preferred in ASCVD |
| SGLT-2 inhibitors | Empagliflozin, dapagliflozin, canagliflozin | CV + renal benefit; preferred in heart failure & CKD |
| DPP-4 inhibitors | Sitagliptin, saxagliptin | Weight neutral, well tolerated |
| Sulfonylureas | Glimepiride, glipizide | Low cost; risk of hypoglycemia |
| Thiazolidinediones (TZDs) | Pioglitazone | Insulin sensitizer; weight gain, fluid retention |
| Basal insulin | Glargine, detemir, degludec | Effective for FPG control |
For ASCVD, heart failure, or diabetic nephropathy: early addition of GLP-1 receptor agonist or SGLT-2 inhibitor is specifically recommended.
Step 3 - Triple therapy or insulin: Metformin + 2 other agents, or Metformin + insulin (basal ± prandial)
Glycemic target: HbA1c <7% for most adults (individualized based on age, comorbidities, hypoglycemia risk)
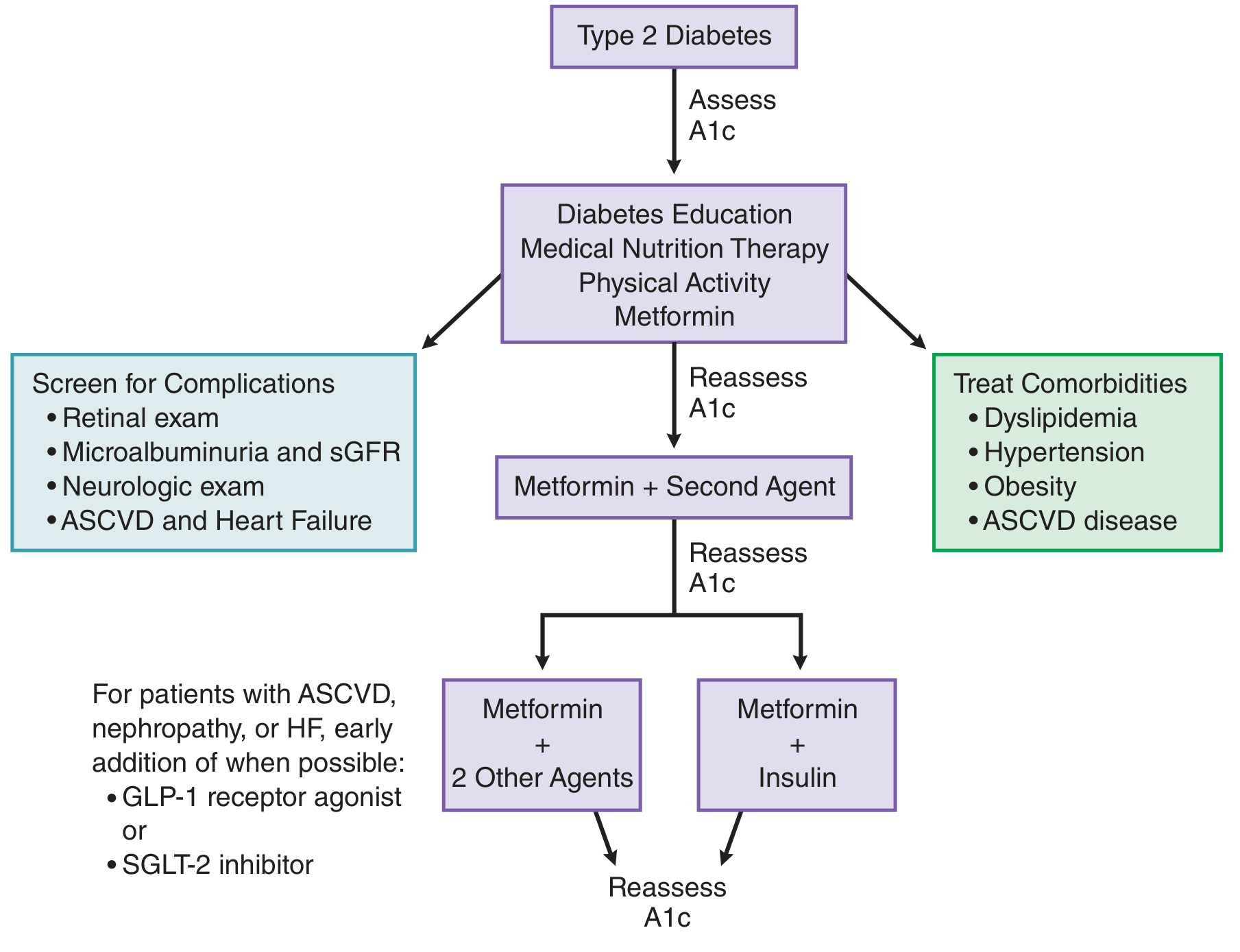
Treatment algorithm: Type 2 Diabetes - Goodman & Gilman's Pharmacological Basis of Therapeutics
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Washington Manual of Medical Therapeutics
10. Monitoring
| Test | Frequency | Target |
|---|---|---|
| HbA1c | Every 3 months (unstable) or every 6 months (stable) | <7% for most patients |
| Fasting/random plasma glucose | Daily self-monitoring (T1DM); variable in T2DM | 80-130 mg/dL fasting |
| Urine ACR | Annually | <30 mg/g |
| Serum creatinine/eGFR | Annually | - |
| Ophthalmologic exam | Annually (T2DM from diagnosis; T1DM from 3-5 years after onset) | - |
| Foot examination | Annually (more often if high-risk) | - |
| Lipid profile | Annually | LDL <100 mg/dL (<70 in high CV risk) |
| Blood pressure | Every visit | <130/80 mmHg |
11. Special Populations
Gestational DM (GDM):
- Diagnosed by OGTT during pregnancy (Carpenter-Coustan or IADPSG criteria)
- First-line: medical nutrition therapy + exercise
- Pharmacotherapy: insulin (preferred); metformin and glyburide used but not universally endorsed
- Increased risk of T2DM in mother (50% lifetime risk) and metabolic syndrome in offspring
Pediatric T1DM:
- Increasing incidence especially under age 5
- Insulin pump and CGM are standard of care in many centers
- Teplizumab may delay onset in high-risk individuals
12. Recent Evidence Update
- A 2024 systematic review and meta-analysis on digital interventions for T2DM self-management (PMID 39037772) confirms the benefit of digital tools for glycemic control
- A 2025 systematic review on GLP-1 receptor agonists and GI adverse events (PMID 40499738) provides updated safety data relevant to clinical counseling
- The GRADE study confirmed that adding liraglutide or basal insulin to metformin provides slightly better glycemic control than glimepiride or sitagliptin
Summary: Key Numbers to Remember
| Parameter | Value |
|---|---|
| T1DM proportion | 5-10% of all DM |
| T2DM proportion | ~90% of all DM |
| HbA1c diagnostic cutoff | ≥6.5% |
| FPG diagnostic cutoff | ≥126 mg/dL |
| HbA1c target (most adults) | <7% |
| Retinopathy reduction with tight control (DCCT) | 76% |
| Nephropathy lifetime risk | 20-40% |
| DPN responsible for amputations | 50-75% of non-traumatic |
| BP target with nephropathy | <130/80 mmHg |
Sources: Tietz Textbook of Laboratory Medicine (7th Ed.), Goodman & Gilman's Pharmacological Basis of Therapeutics, Washington Manual of Medical Therapeutics, Guyton & Hall Medical Physiology, Mulholland & Greenfield's Surgery (7e), Creasy & Resnik's Maternal-Fetal Medicine, Lippincott Illustrated Reviews Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.