Dengue fever
Reading File
Finding Sources
Searching PubMed
dengue fever
Searching the Web
dengue fever 2025 2026 outbreak treatment guidelines WHO
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple textbooks to construct a thorough, well-organized answer on dengue fever.
Dengue Fever - A Comprehensive Overview
Causative Agent & Classification
Dengue is caused by the dengue virus (DENV), an RNA virus of the family Flaviviridae, genus Flavivirus. There are four antigenically distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4 - each capable of causing the full spectrum of dengue disease. A fifth serotype (DENV-5) has been reported but is not clinically classified yet.
Epidemiology
- Global burden: The WHO reports a 30-fold increase in dengue incidence over the past 30 years. An estimated 50 million+ cases occur annually, with 400,000 cases of dengue hemorrhagic fever (DHF). In 2024, the WHO recorded over 14 million cases - a historic high. A CDC report (2025) noted a 359% spike in US dengue incidence in 2024 (3,798 cases vs. an annual average of 828).
- Current outbreaks (2026): Sri Lanka is battling one of its worst outbreaks - over 44,000 cases and 28 deaths by mid-June 2026, with military drones now being deployed to detect mosquito breeding grounds.
- Endemic zones: Tropical and subtropical regions of Southeast Asia, the Pacific, Latin America, and the Caribbean. All four serotypes co-circulate in many areas.
- Vector: Primarily Aedes aegypti (day-biting mosquito); Aedes albopictus is a secondary vector. The mosquito breeds in clean, stagnant water in containers around human dwellings (endophagic and endophilic). It survives best at 16-30°C with 60-80% relative humidity.
- Transmission: Female mosquito acquires virus from a viremic human; extrinsic incubation period is 8-14 days, after which the mosquito remains infective for its lifetime (1-3 months). There is no person-to-person transmission except via blood transfusion and vertical (mother-to-child) transmission.
- Iceberg phenomenon: DF/DHF follows an "iceberg" or pyramid pattern - the majority of cases are asymptomatic at the base, followed by classical DF, DHF, and dengue shock syndrome (DSS) at the apex.
Dengue Virus Infection - Classification
The full spectrum is shown in this WHO classification diagram:
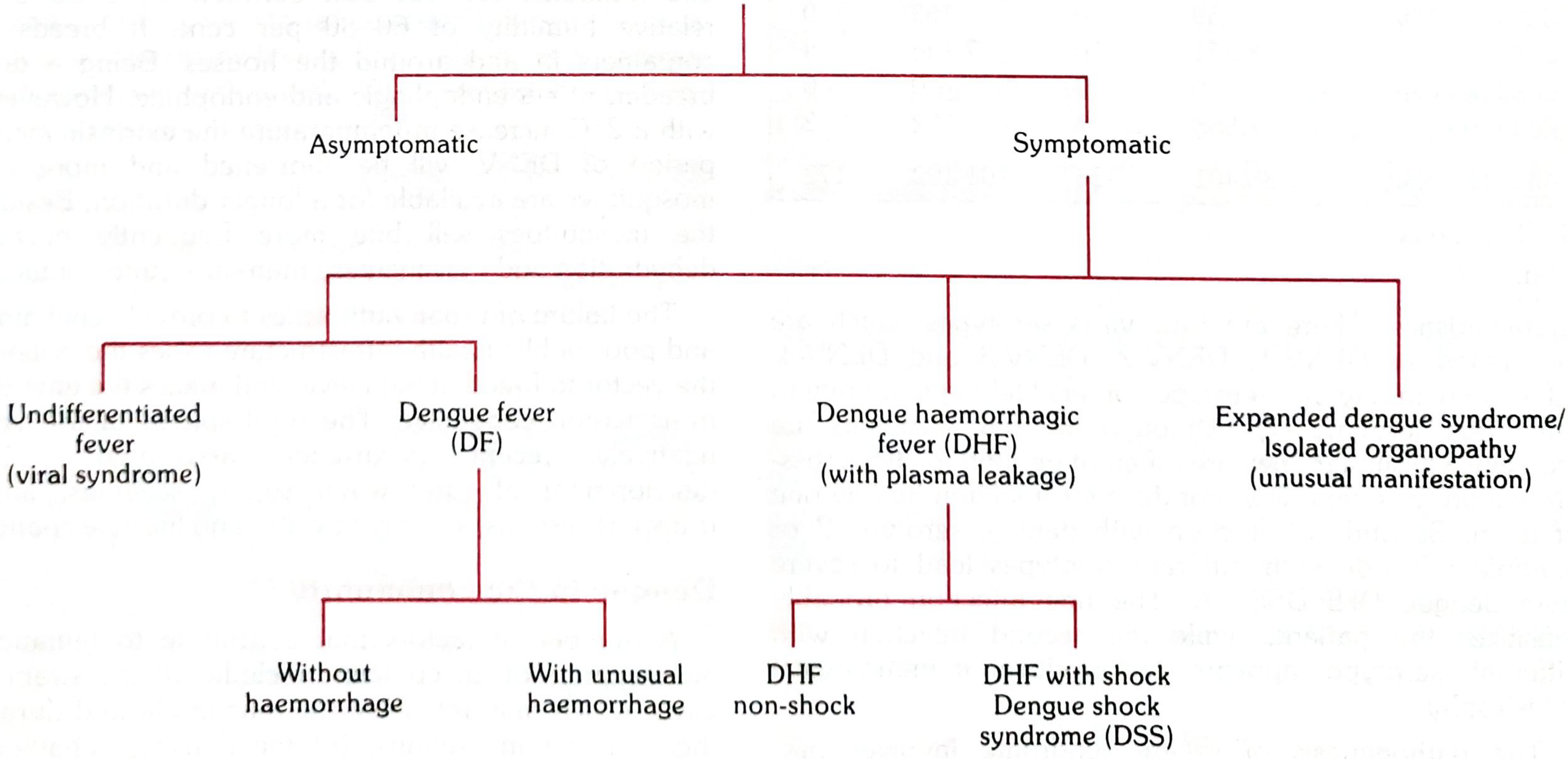
Manifestations of dengue virus infection - Park's Textbook of Preventive and Social Medicine
| Category | Key Feature |
|---|---|
| Asymptomatic | Majority of primary infections |
| Undifferentiated fever | Mild viral syndrome |
| Dengue Fever (DF) | Without/with unusual haemorrhage |
| Dengue Haemorrhagic Fever (DHF) | Plasma leakage; non-shock or with DSS |
| Expanded dengue syndrome | Unusual organ involvement |
Pathogenesis
The key concept is antibody-dependent enhancement (ADE):
- Infection with one serotype confers lifelong immunity to that serotype but only short-duration cross-protection against others.
- On secondary infection with a different serotype, pre-existing dengue antibodies form virus-antibody complexes. These non-neutralizing "enhancing" antibodies promote infection of a larger number of mononuclear cells.
- This triggers massive release of cytokines, vasoactive mediators, and procoagulants, leading to plasma leakage, thrombocytopenia, and disseminated intravascular coagulation (DIC) - the hallmarks of DHF.
- Cross-reactive T cell immune responses also contribute to the cytokine storm.
- Risk of DHF is ~0.2% in primary infection, but at least 10-fold higher with secondary infection by a different serotype. Co-circulation of all four serotypes (as seen in Panama in 2025) sharply increases severe case risk.
(Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.)
Clinical Features
Incubation Period
3-10 days (commonly 5-6 days; Tintinalli's states 4-7 days).
Three Clinical Phases of DHF
| Phase | Duration | Key Features |
|---|---|---|
| Febrile phase | Days 1-3 | Sudden high fever (39-40°C), severe headache, myalgia/arthralgia ("breakbone fever"), retro-orbital pain, facial flushing, anorexia |
| Critical phase | Days 4-6 | Defervescence, plasma leakage, rising haematocrit, pleural effusion/ascites, thrombocytopenia, risk of shock - this is the danger window |
| Recovery phase | Days 7-10 | Reabsorption of fluids, improvement; risk of fluid overload if over-replaced |
Classical Dengue Fever (DF)
- Sudden onset with chills, high fever, intense headache, retro-orbital pain (worsened by eye movement), severe myalgia/arthralgia
- Biphasic fever curve (saddle-back): fever for ~3-4 days, brief remission, then a second febrile phase
- Rash: appears in ~80% of cases during remission or second febrile phase - maculopapular or scarlatiniform, starting on trunk/chest, spreading to extremities and face; may be accompanied by itching and hyperaesthesia
- Fine pale morbilliform rash on trunk spreading outward after defervescence
- Convalescence may be protracted; fatality is exceedingly low in classical DF
- Small children may present with only mild URTI symptoms
Dengue Haemorrhagic Fever (DHF) - WHO Criteria (all four required)
- Acute fever lasting 2-7 days
- Haemorrhagic manifestations: positive tourniquet test, petechiae, ecchymoses, purpura, or bleeding from mucosa/GI tract/injection sites
- Platelet count ≤ 100,000 cells/mm³
- Objective evidence of plasma leakage: haematocrit rise ≥20% from baseline, OR pleural effusion, ascites, hypoproteinaemia
Dengue Shock Syndrome (DSS) - DHF plus shock
- Tachycardia, cool extremities, delayed capillary refill, weak/thready pulse, lethargy or restlessness
- Pulse pressure ≤ 20 mmHg (e.g., 100/80 mmHg)
- Hypotension for age
- Mortality >10% if untreated; can be reduced to <1% with prompt treatment
(Park's Textbook of Preventive and Social Medicine; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
Grading of Dengue Infection (WHO)
| Grade | Features |
|---|---|
| DF | Fever + 2 symptoms; no plasma leakage; thrombocytopenia without haemoconcentration |
| DHF Grade I | Fever + haemorrhagic manifestations (positive tourniquet test) + thrombocytopenia + haemoconcentration |
| DHF Grade II | Grade I + spontaneous bleeding |
| DHF Grade III | Grade I/II + circulatory failure (weak pulse, narrow pulse pressure, hypotension) |
| DHF Grade IV (DSS) | Profound shock; undetectable BP and pulse |
Diagnosis
Probable Diagnosis (clinical):
Acute febrile illness + 2 or more of: headache, retro-orbital pain, myalgia, arthralgia/bone pain, rash, haemorrhagic manifestations, leukopenia (WBC ≤5,000/mm³), thrombocytopenia (<150,000/mm³), rising haematocrit (5-10%) - AND at least one supportive serological finding.
Confirmed Diagnosis (laboratory):
- Virus isolation from serum/CSF/autopsy tissue (within first 6 days of illness)
- Fourfold rise in IgG (HIA) or IgM seroconversion
- Detection of viral antigen/genome by ELISA, immunofluorescence, or RT-PCR
- NS1 antigen detection: ELISA or rapid test - detects antigen from Day 1 to Day 6 (earliest marker, does not differentiate serotype)
- IgM (MAC-ELISA): detectable after Day 5; remains positive for months
Diagnostic Test Timing Summary
| Test | Sample | Window |
|---|---|---|
| NS1 antigen (rapid/ELISA) | Acute serum | Days 1-6 |
| RT-PCR | Acute serum | Days 1-5 |
| IgM ELISA | Serum after Day 5 | Days 5+ |
| IgG ELISA / HIA | Paired sera | Seroconversion Days 15-21 |
| Platelet + haematocrit | Blood | Serial monitoring |
(Park's Textbook; Rosen's Emergency Medicine)
Other Lab Findings
- Leukopenia (characteristic)
- Thrombocytopenia (progressive)
- Rising haematocrit (haemoconcentration from plasma leakage)
- Elevated liver enzymes (ALT/AST)
- Coagulopathy in DHF
Differential Diagnosis
Dengue must be distinguished from:
- Influenza, measles, rubella (similar fever + rash)
- Chikungunya (prominent arthralgia; rash similar)
- Zika virus (conjunctivitis more prominent; teratogenic risk)
- West Nile fever (causes lymphadenopathy - usually absent in dengue)
- Malaria (especially falciparum - must be excluded)
- Leptospirosis, rickettsial infections, meningococcemia (petechial rash overlap)
- Other viral haemorrhagic fevers (Ebola, Marburg, yellow fever)
(Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
Management
There are no specific antiviral agents for dengue. Treatment is entirely supportive.
Dengue Fever (DF - outpatient)
- Rest and adequate oral fluids (ORS, fruit juices, electrolyte-containing drinks)
- Paracetamol for fever and pain
- Avoid NSAIDs and aspirin - risk of bleeding due to thrombocytopenia and platelet dysfunction
- Monitor for warning signs (abdominal pain, persistent vomiting, bleeding, rapid breathing, postural hypotension, drop in platelet count)
- Return to hospital immediately if warning signs develop
DHF Grade I/II (hospital admission)
- IV fluid therapy if oral intake inadequate
- Monitor haematocrit, platelet count, and urine output closely
- Isotonic crystalloids (normal saline or Ringer's lactate)
- Critical phase fluid management: adjust rate based on haematocrit trends
- Watch for signs of over-hydration during recovery phase
DHF Grade III/IV - DSS (ICU)
- Aggressive IV fluid resuscitation (colloid if haematocrit does not improve)
- Oxygen and vital sign monitoring
- Blood product transfusions for significant haemorrhage (packed RBCs, fresh frozen plasma, platelets as needed)
- Organ support as required
- Steroids: several studies evaluated but evidence remains inconclusive - not currently recommended
Disposition
- DF: can be outpatient if tolerating oral fluids and no warning signs
- DHF: hospital admission for IV fluids and monitoring
- DSS: ICU admission
(Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Park's Textbook)
Prevention & Control
Personal Protection
- Insect repellents (DEET, picaridin)
- Protective clothing (long sleeves, long trousers)
- Mosquito nets (especially for sleeping children/infants)
- Window and door screens
Vector Control
- Source reduction: eliminate stagnant water containers (flower pots, tyres, water tanks, coolers) - the cornerstone
- Larviciding: temephos in water containers
- Adult mosquito control: indoor residual spraying, space spraying (fogging)
- Biological control: Bacillus thuringiensis israelensis (Bti), larvivorous fish
- Novel approaches: Wolbachia-infected mosquitoes to suppress virus replication; sterile insect technique; genetically modified mosquitoes
Vaccination
- Dengvaxia (CYD-TDV) by Sanofi Pasteur: first licensed dengue vaccine; tetravalent; recommended only for seropositive individuals (prior dengue infection confirmed) aged 9-16 in endemic areas - risk of severe dengue in seronegative recipients
- TAK-003 (Qdenga) by Takeda: newer tetravalent live-attenuated vaccine; approved in EU, Indonesia, and several other countries; can be given regardless of prior serostatus in endemic regions
Surveillance (India - National Programme)
- 521 sentinel surveillance hospitals with lab support for endemic states
- 14 Apex Referral Laboratories linked to sentinel hospitals
- IgM capture ELISA kits provided free via National Institute of Virology, Pune
- NS1 ELISA kits introduced for early (Day 1) diagnosis
- Mid-term plan components: surveillance, case management, vector management, outbreak response, capacity building, IEC (Information, Education, Communication)
(Park's Textbook of Preventive and Social Medicine)
Recent Evidence (2025)
A 2025 systematic review (PMID 41037858) in Journal of Infection and Public Health provides an updated synthesis of dengue pathogenesis, diagnosis, and management, confirming the supportive-care-only approach and highlighting advances in NS1 detection and the ADE mechanism. Cardiovascular complications are gaining attention - a 2025 meta-analysis (PMID 41160032) confirmed dengue's association with elevated cardiovascular disease risk.
Key "must-know" points at a glance:
- 4 serotypes; secondary infection with a different serotype = risk of DHF via ADE
- Vector: Aedes aegypti - day-biting, breeds in clean stagnant water
- "Breakbone fever" = severe myalgia/arthralgia; biphasic fever; rash on trunk spreading outward
- DHF diagnosis requires all 4 WHO criteria: fever + haemorrhage + thrombocytopenia + plasma leakage
- No antivirals; avoid NSAIDs/aspirin; fluid management is the cornerstone
- NS1 antigen = earliest lab marker (Days 1-6); IgM after Day 5
- Dengvaxia only for seropositive individuals; Qdenga (TAK-003) is the newer option
Heart attack medication, diagnosis, procedure.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
heart attack myocardial infarction 2025 guidelines ACC AHA treatment PCI
Reading File
Reading File
Reading Web Page
https://www.jacc.org/doi/10.1016/j.jacc.2025.01.018
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Heart Attack (Myocardial Infarction) - Medication, Diagnosis & Procedures
What Is a Heart Attack?
A myocardial infarction (MI) occurs when sustained ischemia from coronary artery occlusion - almost always due to rupture of a vulnerable atherosclerotic plaque followed by thrombosis - causes irreversible death (necrosis) of heart muscle. Based on the ECG at presentation, MI is classified into two major types that determine the immediate management strategy:
| Type | ECG Finding | Key Feature |
|---|---|---|
| STEMI (ST-Elevation MI) | ST-segment elevation or new LBBB | Complete occlusion; immediate reperfusion mandatory |
| NSTEMI (Non-ST-Elevation MI) | No ST elevation; troponin elevated | Partial occlusion; urgent-invasive strategy |
| Unstable Angina (UA) | No ST elevation; troponin normal | No myonecrosis; managed like NSTEMI |
NSTEMI is rising in incidence (obesity, diabetes, aging populations, wider use of high-sensitivity troponin). STEMI incidence is declining due to broader aspirin, statin, and smoking cessation uptake. (Harrison's Principles of Internal Medicine, 22nd Ed.)
Pathophysiology
ACS is caused by an imbalance between myocardial oxygen supply and demand, most commonly from coronary arterial thrombosis via:
- Plaque fissure with inflammation - T-cell driven adaptive immune dysregulation
- Plaque fissure without inflammation
- Plaque erosion - present in at least one-third of ACS cases
"Vulnerable plaques" have a lipid-rich core with a thin fibrous cap and an eccentric stenosis at angiography. Patients often have multiple such plaques at risk of disruption simultaneously. (Harrison's 22nd Ed.)
Diagnosis
Symptoms ("MONA" mnemonic for initial management is taught, but here is the clinical picture)
- Chest pain/pressure: severe, at rest, >10 minutes, crushing or squeezing, radiating to left arm, jaw, back, or epigastrium
- Associated features: diaphoresis, dyspnea, nausea/vomiting, lightheadedness, sense of impending doom
- Atypical presentations: women, elderly, and diabetics may present with fatigue, dyspnea, or epigastric pain without classic chest pain
12-Lead ECG (First and Fastest Test - get within 10 minutes of arrival)
| Finding | Interpretation |
|---|---|
| ST elevation ≥1 mm in ≥2 contiguous leads | STEMI - activate cath lab immediately |
| New LBBB | Treat as STEMI if clinical picture fits |
| ST depression + T-wave changes | NSTEMI/UA |
| Pathological Q waves (new) | Prior MI or evolving MI |
| True posterior MI | ST depression V1-V3 + dominant R waves |
Biomarkers
Cardiac Troponin (cTn) - gold standard:
- Most sensitive and specific biomarker available for myocardial necrosis
- High-sensitivity troponin (hsTn) assays allow earlier and more accurate detection
- Standard protocol: measure at presentation, 1 hour, and 3 hours if needed
- Troponin begins to rise 3-6 hours after symptom onset, peaks at 12-24 hours, remains elevated for 7-14 days (helpful for late presenters)
- Caveats: hsTn can be falsely elevated in AKI, myocarditis, PE, sepsis, and many other conditions
| Test | Sensitivity (serial) | Specificity |
|---|---|---|
| Troponin I (serial) | 90-100% | 83-96% |
| CK-MB (serial) | 79% | 96-97% |
| Myoglobin (serial) | 89% | 87% |
(Rosen's Emergency Medicine)
Other Investigations
- Chest X-ray: cardiomegaly, pulmonary edema (Killip class assessment)
- Echocardiogram: wall motion abnormalities, LV function, pericardial effusion, mechanical complications
- Coronary angiography: definitive anatomy - culprit artery identification; gold standard for STEMI
- CT coronary angiography (CTCA): for intermediate-risk patients in the ED, or to rule out obstructive CAD
Differential Diagnosis of Troponin Elevation (causes of myocardial injury that are NOT MI)
- Myocarditis, takotsubo cardiomyopathy, heart failure
- Pulmonary embolism, stroke/subarachnoid haemorrhage
- Sepsis, critical illness, renal failure
- Cardiac contusion, defibrillator shocks, ablation
- Chemotherapy agents (Fourth Universal Definition of MI, 2018)
Treatment - Medications
1. Immediate ("Upstream") Therapy - ALL ACS
A. Antiplatelet Agents
| Drug | Class | Dose | Notes |
|---|---|---|---|
| Aspirin (ASA) | COX-1 inhibitor | 162-325 mg loading dose, then 75-100 mg daily | Give to ALL ACS patients immediately; irreversible platelet inhibition |
| Ticagrelor | P2Y12 inhibitor (reversible) | 180 mg load, then 90 mg twice daily | Preferred for NSTE-ACS and STEMI; superior to clopidogrel; avoid if prior stroke/TIA |
| Prasugrel | P2Y12 inhibitor (irreversible) | 60 mg load, then 10 mg daily | Preferred for STEMI-PCI; stronger than clopidogrel; avoid if prior stroke/TIA, age >75, weight <60 kg |
| Clopidogrel | P2Y12 inhibitor (irreversible) | 300-600 mg load, then 75 mg daily | Use if fibrinolysis given, or if ticagrelor/prasugrel contraindicated; CYP2C19 polymorphism affects response in ~30% |
Per the 2025 ACC/AHA ACS Guideline: Ticagrelor or prasugrel are preferred over clopidogrel for both STEMI and NSTE-ACS patients undergoing PCI. Transition to ticagrelor monotherapy ≥1 month post-PCI is recommended to reduce bleeding while maintaining protection. Dual antiplatelet therapy (DAPT) should continue for 12 months unless high bleeding risk. (2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline - JACC 2025)
B. Anticoagulation
| Drug | Use | Notes |
|---|---|---|
| Unfractionated heparin (UFH) | PCI or fibrinolysis | Most widely used; monitor APTT |
| Enoxaparin (LMWH) | Fibrinolysis, NSTE-ACS | 30 mg IV bolus then 1 mg/kg SC bid; avoid if creatinine >2.5 (men) or >2.0 (women) mg/dL |
| Bivalirudin | PCI (especially with HIT) | Direct thrombin inhibitor; 0.75 mg/kg bolus + 1.75 mg/kg/h infusion; lower bleeding but higher stent thrombosis than heparin+GPIIb/IIIa |
| Fondaparinux | NSTE-ACS, fibrinolysis | Factor Xa inhibitor; preferred if high bleeding risk |
C. Anti-Ischemic Agents
| Drug | Details | Contraindications |
|---|---|---|
| Nitroglycerin (GTN) | SL 0.3-0.6 mg q5min x3, then IV 5-200 mcg/min | Hypotension (SBP <90), RV infarct, HR <50 or >100, PDE-5 inhibitor use within 24-48h, severe AS |
| Beta-blockers (metoprolol, atenolol, carvedilol) | Start oral within 24h; reduce infarct size, arrhythmia, mortality | Killip class II+, cardiogenic shock, HR <60, SBP <120, PR >0.24s, 2nd/3rd AV block, severe bronchospasm |
| Morphine | 2-4 mg IV for refractory pain | Caution - may mask symptoms; reduces catecholamines |
| Oxygen | If O2 saturation <90% or heart failure | Avoid in normoxic patients (may increase infarct size) |
| Calcium channel blockers | Vasospastic angina; if beta-blocker contraindicated | Avoid if LV dysfunction, pulmonary edema, SBP <90 |
D. Lipid-Lowering (Start during admission)
- High-intensity statins (atorvastatin 40-80 mg or rosuvastatin 20-40 mg): recommended for ALL ACS patients; reduce MACE (2025 ACC/AHA Guideline)
- Ezetimibe + statin: if LDL-C goal not achieved on statin alone (goal <70 mg/dL, or <55 mg/dL for very high risk)
- PCSK9 inhibitors (evolocumab, alirocumab): for recurrent ACS or LDL not at goal despite max statin + ezetimibe; LDL goal as low as <40 mg/dL in recurrent events within 2 years
E. Other Long-Term Post-MI Medications
| Drug | Indication | Benefit |
|---|---|---|
| ACE inhibitor / ARB | All MI patients (especially reduced EF, diabetes, HTN) | Reduce LV remodeling, mortality |
| Beta-blocker (long-term) | All MI with reduced EF (LVEF <40%) | Reduce sudden death, mortality |
| Aldosterone antagonist (eplerenone/spironolactone) | Post-MI with LVEF ≤40% and HF or diabetes | Reduce mortality (EPHESUS trial) |
| Aspirin | Lifelong | Secondary prevention |
Procedures
1. Primary Percutaneous Coronary Intervention (Primary PCI) - Gold Standard for STEMI
The preferred reperfusion strategy when available within the required time frame.
How PCI works:
- Patient is taken to the cardiac catheterisation laboratory
- Arterial access obtained - radial artery approach is now preferred over femoral (lower bleeding, possible mortality benefit)
- A guiding catheter is inserted and advanced to the coronary ostium under fluoroscopy
- A thin guidewire crosses the occlusion
- A balloon catheter is inflated to open the artery (balloon angioplasty)
- A coronary stent is deployed - drug-eluting stents (DES) are preferred over bare-metal stents (BMS); DES reduce restenosis
- Post-procedure imaging confirms restored blood flow (TIMI 3 flow = normal)
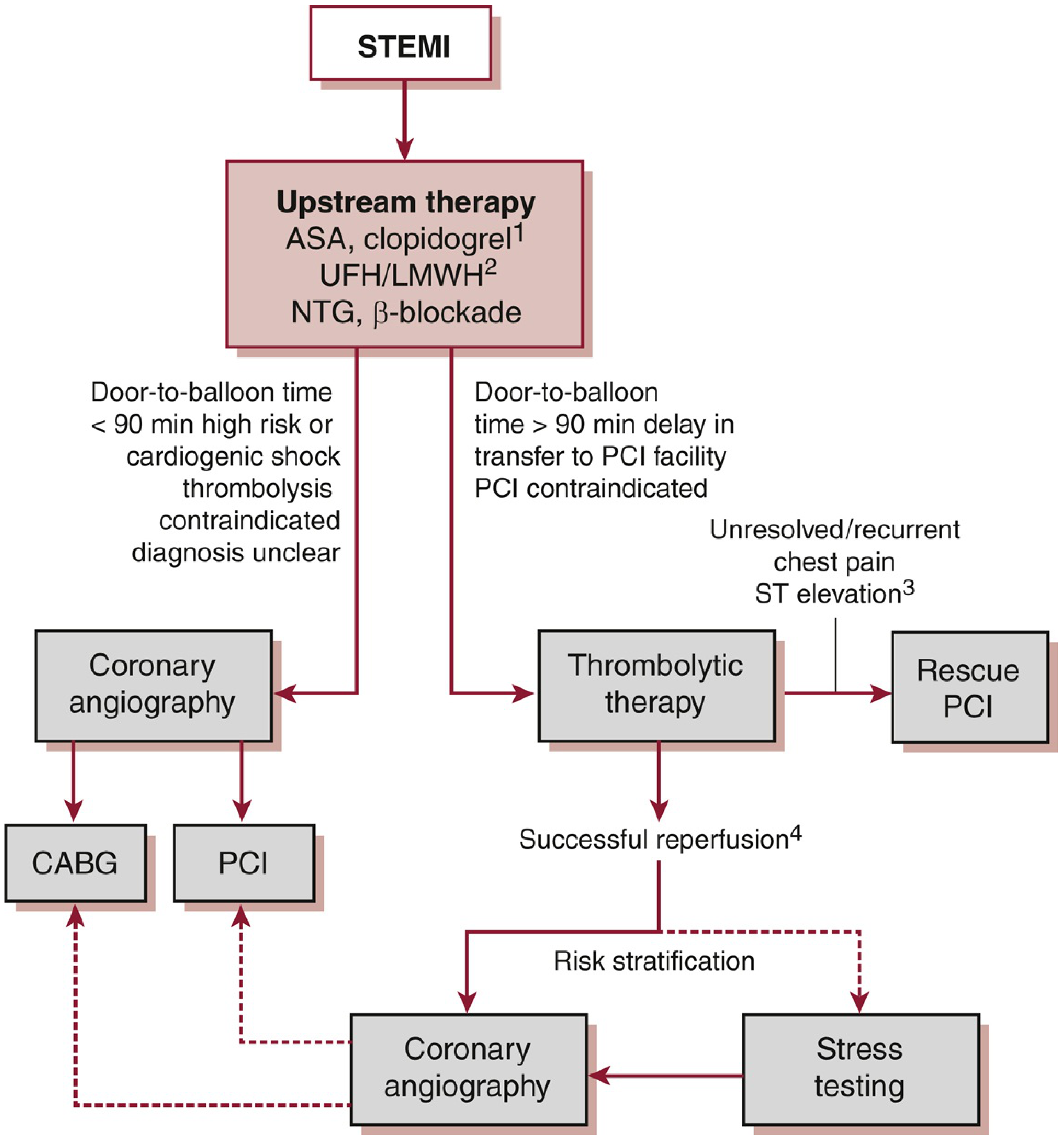
Time targets (critical):
- Door-to-balloon (D2B) time: ≤90 minutes from first medical contact
- If transfer required: first medical contact to balloon ≤120 minutes
- If neither target achievable, give fibrinolytics first
PCI is ALWAYS preferred over fibrinolysis when:
- Cardiogenic shock (Killip III/IV) or severe heart failure
- Contraindication to fibrinolytics exists
- Symptom onset >12 hours prior
- Prior CABG or recent PCI
- Diagnosis uncertain
Multivessel disease: In hemodynamically stable STEMI with multivessel disease, complete revascularization (PCI of non-culprit lesions) is now recommended - either during index PCI or within 45 days - per the 2025 ACC/AHA Guideline. In cardiogenic shock (CULPRIT-SHOCK trial), culprit-lesion-only PCI reduces mortality. (Washington Manual; 2025 ACC/AHA Guideline)
2. Fibrinolytic (Thrombolytic) Therapy
Used when primary PCI is not available within 120 minutes.
| Drug | Type | Dose |
|---|---|---|
| Alteplase (tPA) | Fibrin-specific | 15 mg IV bolus, then 0.75 mg/kg over 30 min, then 0.5 mg/kg over 60 min |
| Tenecteplase (TNK-tPA) | Fibrin-specific, single bolus | Weight-based bolus; easier to administer pre-hospital |
| Reteplase (rPA) | Fibrin-specific, double bolus | Two 10-unit boluses 30 min apart |
| Streptokinase | Non-fibrin-specific | 1.5 million units over 60 min; older, cheaper |
When to give: within 12 hours of symptom onset with qualifying ECG (ST elevation, new LBBB, or true posterior MI); most effective in first 3 hours.
Must administer within 30 minutes of patient contact (door-to-needle time ≤30 min)
Absolute contraindications to fibrinolytics:
- Any prior intracranial hemorrhage
- Ischemic stroke within 3 months
- Active internal bleeding
- Aortic dissection
- Severe head trauma/CNS surgery within 2 months
- Significant closed-head injury within 3 months
Signs of successful reperfusion: chest pain relief, ≥50% reduction in ST elevation, reperfusion arrhythmia (accelerated idioventricular rhythm)
If fibrinolysis fails: Rescue PCI (ongoing chest pain, recurrent ST elevation, hemodynamic instability 60-90 minutes after fibrinolysis)
3. Coronary Artery Bypass Graft (CABG)
Surgical revascularisation, generally reserved for:
- Left main coronary artery disease
- Three-vessel disease, especially with diabetes or reduced LV function
- Anatomy unsuitable for PCI (heavily calcified, tortuous vessels)
- Failed PCI or mechanical complications of MI (VSD, papillary muscle rupture)
Left internal mammary artery (LIMA) to LAD is the gold-standard conduit; saphenous vein grafts used for other vessels.
4. Invasive Strategy for NSTE-ACS
NSTEMI patients do not need immediate PCI like STEMI, but risk stratification guides timing:
| Risk Level | Strategy | Timing |
|---|---|---|
| Very high risk (ongoing ischemia, shock, arrhythmia, refractory symptoms) | Immediate invasive | <2 hours |
| High risk (troponin rise, dynamic ST changes, GRACE score >140) | Early invasive | <24 hours |
| Intermediate risk (diabetes, CKD, EF <40%, GRACE 109-140) | Invasive | 24-72 hours |
| Low risk | Ischemia evaluation (stress test or CTCA) | Elective |
Killip Classification (for risk stratification in STEMI)
| Class | Clinical Features | Mortality |
|---|---|---|
| I | No heart failure | ~6% |
| II | S3 gallop, rales <50% lung fields, elevated JVP | ~17% |
| III | Pulmonary edema (rales >50% lung fields) | ~38% |
| IV | Cardiogenic shock (hypotension + end-organ hypoperfusion) | ~81% |
Complications of MI
| Complication | Timing | Notes |
|---|---|---|
| Arrhythmias (VF, VT, complete heart block) | Hours to days | VF is leading cause of out-of-hospital death |
| Left ventricular failure / cardiogenic shock | Early | Most common cause of in-hospital death |
| Mechanical: Free wall rupture, VSD, papillary muscle rupture (acute MR) | Days 3-7 | Surgical emergency |
| Pericarditis (Dressler's syndrome) | Weeks to months | Autoimmune; treat with NSAIDs/colchicine |
| LV thrombus | Weeks | Anticoagulate; risk of stroke |
| Reinfarction | Days to weeks | Stent thrombosis, new plaque rupture |
Summary: The "MONA + DAPT + Reperfuse" Approach
Acute MI → Aspirin + P2Y12 inhibitor (DAPT) + Anticoagulant
→ Nitroglycerin (if no contraindication)
→ Oxygen (if SpO2 <90%)
→ Beta-blocker (oral, within 24h if stable)
→ High-intensity statin (start immediately)
→ REPERFUSION:
STEMI → Primary PCI (door-to-balloon ≤90 min)
→ Fibrinolysis if PCI unavailable within 120 min
NSTEMI → Risk-stratify → Invasive strategy within 24-72h
→ Long-term: ASA + ACEi/ARB + beta-blocker + statin ± eplerenone
Key 2025 Guideline Updates (ACC/AHA):
- Ticagrelor/prasugrel preferred over clopidogrel for PCI patients
- Transition to ticagrelor monotherapy ≥1 month post-PCI reduces bleeding
- Complete revascularization recommended in stable STEMI with multivessel disease (within 45 days)
- Radial artery access recommended over femoral for coronary angiography
- High-intensity statin + ezetimibe ± PCSK9 inhibitor for aggressive LDL lowering post-MI
- In cardiogenic shock: culprit-lesion only PCI (not multivessel at same sitting)
(Sources: Harrison's Principles of Internal Medicine 22nd Ed; Washington Manual of Medical Therapeutics; Fuster and Hurst's The Heart 15th Ed; Rosen's Emergency Medicine; 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline)
Heart attack define, medication and diagnosis and Clinical frecure
Finding Sources
Finding Sources
Searching the Web
myocardial infarction clinical features diagnosis medications 2025 guidelines
Finding Sources
Finding Sources
Searching PubMed
"acute myocardial infarction"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, authoritative data from multiple textbooks plus current guidelines. Let me compile the complete answer.
Heart Attack (Myocardial Infarction) - Definition, Clinical Features, Diagnosis & Medications
1. DEFINITION
A myocardial infarction (MI), commonly called a "heart attack," is the necrosis (irreversible death) of heart muscle resulting from sustained ischemia - a critically reduced blood supply to the myocardium.
The 2018 Fourth Universal Definition (joint U.S./European Cardiology Task Force) defines MI as:
"The presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
(Robbins & Kumar Basic Pathology)
What Happens Physiologically?
When a coronary artery is suddenly blocked, blood flow ceases in the vessels beyond the occlusion. The muscle in that zone:
- Has zero or near-zero blood flow - unable to sustain function
- Within hours of no blood supply, cardiac muscle cells die
- The infarcted area becomes engorged with deoxygenated stagnant blood, taking on a bluish-brown hue
- Vessel walls become permeable, leaking fluid → local oedema
- Cellular metabolism shuts down → cell swelling and death
The subendocardium is most vulnerable - it has the highest oxygen consumption and vessels are compressed during systolic contraction. Even 15-30% of normal coronary blood flow can keep muscle alive; it is only the central zone with near-complete occlusion that dies.
(Guyton and Hall Textbook of Medical Physiology)
How Does the Occlusion Form? - The 4-Step Sequence
- An atherosclerotic plaque is eroded or suddenly disrupted by endothelial injury, intraplaque haemorrhage, or mechanical forces - exposing subendothelial collagen and necrotic plaque contents to blood
- Platelets adhere, aggregate, and activate - releasing thromboxane A2, ADP, and serotonin, causing further platelet aggregation and vasospasm
- Coagulation is activated by exposed tissue factor - adding to the growing thrombus
- Within minutes, the enlarging thrombus completely occludes the coronary artery lumen
Angiography within 4 hours of MI shows thrombotic occlusion in ~90% of cases. In 10% of MIs, transmural infarction occurs without atherosclerosis - due to coronary vasospasm, embolism from mural thrombi (e.g., in atrial fibrillation), or valve vegetations.
(Robbins & Kumar Basic Pathology)
2. CLINICAL FEATURES (Symptoms and Signs)
ACS Spectrum - How Patients Present
A. Symptoms
| Symptom | Details |
|---|---|
| Chest pain/pressure | The hallmark - severe, crushing, squeezing, or pressure-like; substernal location |
| Radiation | To left arm, left shoulder, neck, jaw, back, or epigastrium |
| Duration | Typically >10 minutes; often persistent and unrelieved by rest |
| Diaphoresis | Profuse sweating - a very important warning sign |
| Dyspnea | Shortness of breath - due to reduced LV function or pulmonary oedema |
| Nausea and vomiting | Common, especially with inferior MI (vagal activation) |
| Lightheadedness/syncope | Due to reduced cardiac output or arrhythmia |
| Sense of impending doom | Classic - patient may feel they are dying |
| Epigastric pain | Mistaken for indigestion, especially in inferior MI |
| Fatigue/weakness | May be the only complaint in women, elderly, and diabetics |
B. "Atypical" or Silent Presentations
Women, elderly patients, and patients with diabetes mellitus frequently do NOT have classic chest pain. They may present with:
- Fatigue alone
- Dyspnea without chest pain
- Nausea/vomiting
- Jaw or arm discomfort without chest pain
These patients are at risk of delayed diagnosis.
C. Physical Examination Findings
| Finding | Significance |
|---|---|
| Diaphoresis, pale, cool skin | Sympathetic activation, reduced cardiac output |
| Sinus tachycardia | Compensatory response to reduced stroke volume |
| S3 gallop | Reduced LV compliance, early heart failure |
| S4 gallop | Stiff, ischaemic ventricle |
| Basilar rales (crackles) | Pulmonary oedema from LV failure |
| Hypotension | Cardiogenic shock - very serious |
| Elevated JVP | Right ventricular failure (RV infarction or severe LV failure) |
| New mitral regurgitation murmur | Papillary muscle dysfunction or rupture |
| Pericardial friction rub | Pericarditis (later complication) |
(Harrison's Principles of Internal Medicine, 22nd Ed.)
D. Killip Classification (Severity Grading at Presentation)
| Class | Features | Approximate Mortality |
|---|---|---|
| I | No signs of heart failure | ~6% |
| II | S3 gallop, rales in <50% of lung fields, raised JVP | ~17% |
| III | Pulmonary oedema (rales >50% of lung fields) | ~38% |
| IV | Cardiogenic shock (hypotension + end-organ failure) | ~81% |
E. Arrhythmias After MI
MI is commonly complicated by serious ventricular arrhythmias. They occur in three periods:
- First 30 minutes: re-entry arrhythmias (most dangerous - VF risk highest)
- 12 hours later: arrhythmias from increased automaticity
- 3 days to weeks: re-entry again (due to scarring)
Ventricular fibrillation is the most common cause of sudden death in the first hour after MI.
(Ganong's Review of Medical Physiology, 26th Ed.)
3. DIAGNOSIS
Step 1 - ECG (Electrocardiogram) - Get within 10 minutes of arrival
The ECG is the single most important immediate test. It classifies the MI and determines the treatment pathway.
ECG Changes in MI - Three Stages
| Stage | Timing | ECG Finding |
|---|---|---|
| Hyperacute | Minutes to hours | Tall, peaked (hyperacute) T waves; ST-segment elevation begins |
| Acute | Hours to days | ST elevation (STEMI); pathological Q waves begin to appear |
| Evolving/Old | Days to weeks | ST settles; T-wave inversion; permanent Q waves remain |
Why Does ST Elevation Occur? (Mechanism)
Three simultaneous membrane changes occur in infarcted cells:
- Rapid repolarization → current flows OUT of infarct → ST elevation
- Decreased resting membrane potential → current flows INTO infarct during diastole → TQ depression (recorded as ST elevation)
- Delayed depolarization → current flows OUT of infarct → ST elevation
All three changes cause the same result: ST segment elevation in leads overlying the infarct, and reciprocal ST depression in leads on the opposite side of the heart.
(Ganong's Review of Medical Physiology, 26th Ed.)
Serial ECG Pattern in Anterior MI:
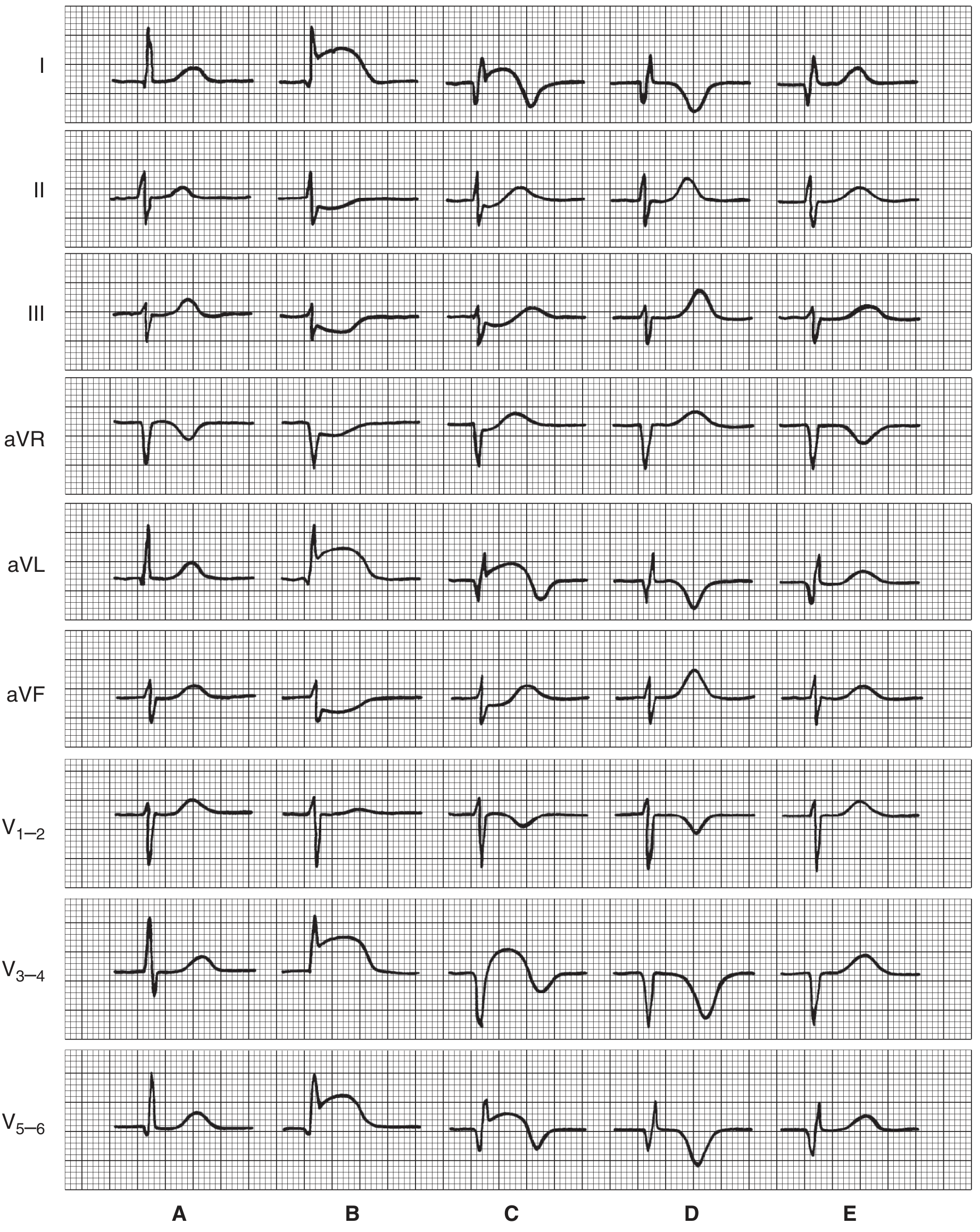
ECG Classification by Location
| Infarct Location | Leads with ST Elevation | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD (left anterior descending) |
| Inferior | II, III, aVF | RCA (right coronary artery) |
| Lateral | I, aVL, V5-V6 | LCx (left circumflex) |
| Posterior | ST depression V1-V3 + tall R waves | RCA or LCx |
| Right Ventricular | V1 + right-sided leads (V3R, V4R) | RCA (proximal) |
Pathological Q Wave Criteria
- Leads V2-V3: Q wave ≥0.02 seconds OR QS complex
- Other leads: Q wave ≥0.03 seconds AND ≥0.1 mV deep in ≥2 contiguous leads
- New LBBB (left bundle branch block) with symptoms = treat as STEMI
(Washington Manual of Medical Therapeutics)
Step 2 - Cardiac Biomarkers
Cardiac Troponin (cTn) - the gold-standard biomarker
| Feature | Details |
|---|---|
| Type | Troponin I (cTnI) or Troponin T (cTnT); high-sensitivity (hs-cTn) assays now preferred |
| Rises | 3-6 hours after onset of infarction |
| Peaks | 12-24 hours |
| Normalises | 7-14 days (useful for late presenters) |
| Protocol | Measure at presentation, at 1 hour, and at 3 hours if needed |
| Significance | Risk of cardiac death is directly proportional to degree of troponin elevation; peak level can estimate infarct size |
Important: Initial biomarkers may be NORMAL if the patient arrives within the first few hours. A normal troponin on arrival never rules out STEMI - treat on ECG findings, not biomarkers, for STEMI.
Other biomarkers (less commonly used now):
- CK-MB: rises in 4-6 hours; useful for re-infarction detection (faster normalisation)
- Myoglobin: earliest to rise (1-3 hours) but very non-specific
Step 3 - Other Investigations
| Investigation | What It Shows |
|---|---|
| Chest X-ray | Pulmonary oedema, cardiomegaly, pneumothorax, aortic dissection |
| Echocardiogram (TTE) | Wall motion abnormalities, LV function (EF), pericardial effusion, mechanical complications (VSD, MR); done when diagnosis is uncertain |
| Coronary Angiography | Gold standard - identifies culprit artery and stenosis anatomy; performed during PCI |
| Blood tests | CBC, coagulation (APTT, PT, INR), creatinine, electrolytes (including Mg2+), lipid profile, glucose |
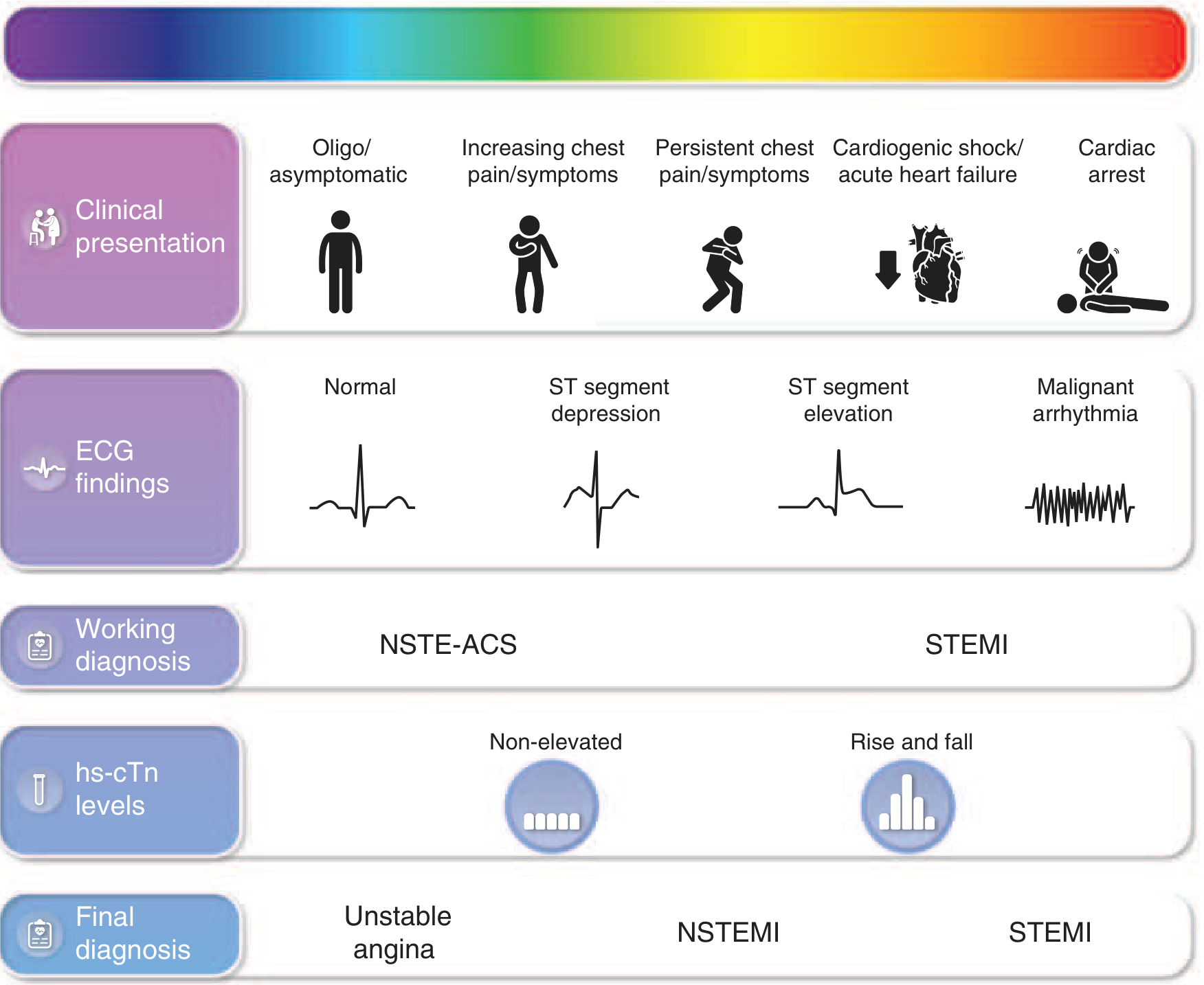
STEMI vs NSTEMI vs Unstable Angina - Final Diagnosis Framework
| Diagnosis | ECG | Troponin |
|---|---|---|
| STEMI | ST elevation / new LBBB | Elevated (rises and falls) |
| NSTEMI | ST depression / T-wave changes / normal | Elevated |
| Unstable Angina | ST depression / normal | Normal |
4. MEDICATIONS
A. Immediate Upstream Therapy (given to ALL ACS patients as soon as possible)
Antiplatelet Agents (Dual Antiplatelet Therapy - DAPT)
| Drug | Dose | Key Points |
|---|---|---|
| Aspirin (ASA) | 162-325 mg chewed/crushed immediately; then 75-100 mg daily lifelong | Non-enteric-coated; chewed for rapid absorption and platelet inhibition; first drug given |
| Ticagrelor | 180 mg loading dose; then 90 mg twice daily | Preferred for NSTE-ACS and STEMI (mortality benefit over clopidogrel); ASA dose must not exceed 100 mg when used with ticagrelor |
| Prasugrel | 60 mg loading dose; then 10 mg daily | Preferred for STEMI-PCI; quicker and more potent than clopidogrel; avoid in patients >75 years, <60 kg body weight, or history of stroke/TIA |
| Clopidogrel | 600 mg loading dose; then 75 mg daily | Used when fibrinolysis is given, or if ticagrelor/prasugrel are contraindicated; response varies due to CYP2C19 genetic polymorphism in ~30% of patients |
Duration of DAPT: minimum 12 months post-ACS if not high bleeding risk. Per the 2025 ACC/AHA Guideline, transition to ticagrelor monotherapy ≥1 month after PCI is recommended to reduce bleeding while maintaining protection.
Anticoagulants
| Drug | Dose | Key Points |
|---|---|---|
| Unfractionated Heparin (UFH) | 60 units/kg IV bolus (max 4,000 units); then 12 units/kg/h | Given to ALL PCI patients and most thrombolysis patients |
| Enoxaparin (LMWH) | 30 mg IV bolus; then 1 mg/kg SC every 12h | Patients >75 years: no loading dose; 0.75 mg/kg SC bid; preferred in fibrinolysis |
| Bivalirudin | 0.75 mg/kg IV bolus; then 1.75 mg/kg/h | Direct thrombin inhibitor; drug of choice in heparin-induced thrombocytopenia (HIT); less bleeding but higher stent thrombosis |
| Fondaparinux | 2.5 mg IV; then 2.5 mg SC daily | Superior to UFH with fibrinolysis; do not use alone during PCI (risk of catheter thrombosis) |
Anti-Ischaemic Agents
| Drug | Dose | When to Use / Avoid |
|---|---|---|
| Nitroglycerin (GTN) | 0.4 mg SL every 5 min x3; then 10-200 mcg/min IV | Chest pain, hypertension, pulmonary oedema; avoid if SBP <90 mmHg, RV infarct, HR <50 or >100, recent PDE-5 inhibitor (sildenafil/vardenafil within 24h; tadalafil within 48h) |
| Beta-blockers (Metoprolol) | 25 mg orally 4x/day; titrate as needed | Start within 24 hours for ALL stable patients; reduces infarct size, arrhythmia, mortality; avoid if Killip ≥II, SBP <120, HR <60, PR >0.24s, 2nd/3rd AV block, severe bronchospasm |
| Morphine | 2-4 mg IV | Severe refractory chest pain not relieved by 3 doses of GTN; reduces catecholamines; caution - may mask ongoing ischaemia |
| Oxygen | Supplemental | Only if SpO2 <90%; avoid in normoxic patients (may increase infarct size and cause vasoconstriction) |
| Calcium channel blockers | Amlodipine, diltiazem | Used for vasospastic angina, or if beta-blockers are contraindicated; avoid in LV dysfunction, pulmonary oedema |
Statins - Start During Admission
- High-intensity statin: Atorvastatin 40-80 mg OR Rosuvastatin 20-40 mg
- Start immediately for ALL ACS patients regardless of baseline LDL
- 2025 ACC/AHA Guideline (Class I recommendation): high-intensity statins reduce major adverse cardiovascular events (MACE)
- If LDL not at goal: add ezetimibe; if still not at goal, add PCSK9 inhibitor (evolocumab or alirocumab)
B. Long-Term Post-MI Medications
| Drug Class | Example | Indication | Benefit |
|---|---|---|---|
| Aspirin (lifelong) | 75-100 mg daily | All MI patients | Secondary prevention |
| P2Y12 inhibitor | Ticagrelor or clopidogrel | Post-PCI, up to 12 months | Prevent stent thrombosis and re-infarction |
| Beta-blocker | Metoprolol, carvedilol | All MI, especially if EF <40% | Reduce sudden death, mortality, LV remodelling |
| ACE inhibitor / ARB | Ramipril, enalapril / valsartan | All MI (especially EF <40%, diabetes, HTN) | Reduce LV remodelling, mortality |
| Aldosterone antagonist | Eplerenone, spironolactone | EF ≤40% + heart failure or diabetes | Reduces mortality (EPHESUS trial) |
| High-intensity statin | Atorvastatin 80 mg | All MI patients | Plaque stabilisation, reduced MACE |
Quick Summary Reference
HEART ATTACK (MI)
│
├── DEFINITION: Ischaemic necrosis of myocardium from coronary
│ artery occlusion (>90% due to atherosclerotic plaque rupture
│ + thrombosis)
│
├── CLINICAL FEATURES:
│ ├── Chest pain (crushing, central, radiating to arm/jaw)
│ ├── Diaphoresis, nausea, vomiting, dyspnoea
│ ├── Atypical: fatigue, epigastric pain (women, elderly, DM)
│ └── Signs: tachycardia, S3/S4, rales, hypotension (if shock)
│
├── DIAGNOSIS:
│ ├── ECG (within 10 min): ST elevation → STEMI
│ │ ST depression/normal → NSTEMI/UA
│ ├── Troponin: rises 3-6h, peaks 12-24h, measure at 0/1/3h
│ ├── CXR: pulmonary oedema, cardiomegaly
│ └── Echo: wall motion abnormalities, LV function
│
└── MEDICATIONS:
├── IMMEDIATE: Aspirin + Ticagrelor/Prasugrel + UFH/Enoxaparin
├── ANTI-ISCHAEMIC: GTN, Beta-blocker, Oxygen (if SpO2 <90%)
├── STATIN: High-intensity (atorvastatin 80 mg) - start now
└── LONG-TERM: ASA + ACEi + Beta-blocker + Statin ± Eplerenone
(Sources: Guyton & Hall Medical Physiology; Robbins & Kumar Basic Pathology; Ganong's Review of Medical Physiology; Harrison's Principles of Internal Medicine 22nd Ed; Washington Manual of Medical Therapeutics; 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline - JACC)
This is a shared conversation. Sign in to Orris to start your own chat.