Influenza
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
influenza management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Here is the full overview:
Influenza
1. Virology and Classification
Influenza viruses belong to the family Orthomyxoviridae and contain a segmented, single-stranded, negative-sense RNA genome. Three types infect humans:
- Type A - most clinically important; undergoes both antigenic drift and shift; classified by surface glycoproteins hemagglutinin (H1-H18) and neuraminidase (N1-N11)
- Type B - predominantly human; undergoes antigenic drift but NOT shift; two circulating lineages (Victoria and Yamagata)
- Type C - rare; causes mild intermittent illness
Genome Segments and Key Proteins
| Segment | Protein | Function |
|---|---|---|
| 4 | HA (Hemagglutinin) | Viral attachment to sialic acid receptors; fusion protein; target of neutralizing antibody |
| 6 | NA (Neuraminidase) | Cleaves sialic acid; promotes virus release from cells; target of oseltamivir/zanamivir |
| 7 | M2 | Proton channel; facilitates uncoating; target of amantadine/rimantadine |
| 1-3 | PB1, PB2, PA | RNA polymerase complex |
- Medical Microbiology 9e, p. 555 (Segment/Protein table)
2. Antigenic Variation - The Key to Epidemics
Antigenic Drift - Minor point mutations in HA and NA genes. Occurs every 2-3 years. Causes local/regional outbreaks of both influenza A and B. This is why the vaccine must be reformulated annually.
Antigenic Shift - Major reassortment of genome segments between different strains (including animal strains). Occurs only with influenza A. Can cause pandemics because few humans have pre-existing immunity.
Historical Pandemics from Antigenic Shift
| Year | Subtype | Name |
|---|---|---|
| 1918 | H1N1 | Spanish flu |
| 1957 | H2N2 | Asian flu |
| 1968 | H3N2 | Hong Kong flu |
| 1977 | H1N1 | Russian flu |
| 2009 | H1N1 | Swine flu (pdm09) |
The 2009 H1N1pdm strain was a reassortment with gene segments from avian, human, and swine hosts. Swine are proposed as a "mixing vessel" because their respiratory epithelial cells express both human-type (alpha-2,6-galactose) and avian-type (alpha-2,3-galactose) sialic acid receptors.
- Harrison's Principles of Internal Medicine 22E, p. 1589; Medical Microbiology 9e, p. 555
3. Pathogenesis
Infection is initiated in the upper respiratory tract via aerosolized virus. HA binds to sialic acid on ciliated respiratory epithelial cells. After endocytosis, the M2 proton channel acidifies the endosome, releasing the nucleocapsid into the cytoplasm. Viral RNA is transcribed and replicated in the nucleus; NA cleaves sialic acid on newly formed virions to facilitate release.
Denudation of superficial epithelium accounts for much of the symptomatology and predisposes to secondary bacterial pneumonia. Systemic symptoms (fever, myalgia, malaise) are largely cytokine-mediated - excessive cytokine production also explains the acute toxicity of H5N1.
Time Course of Infection
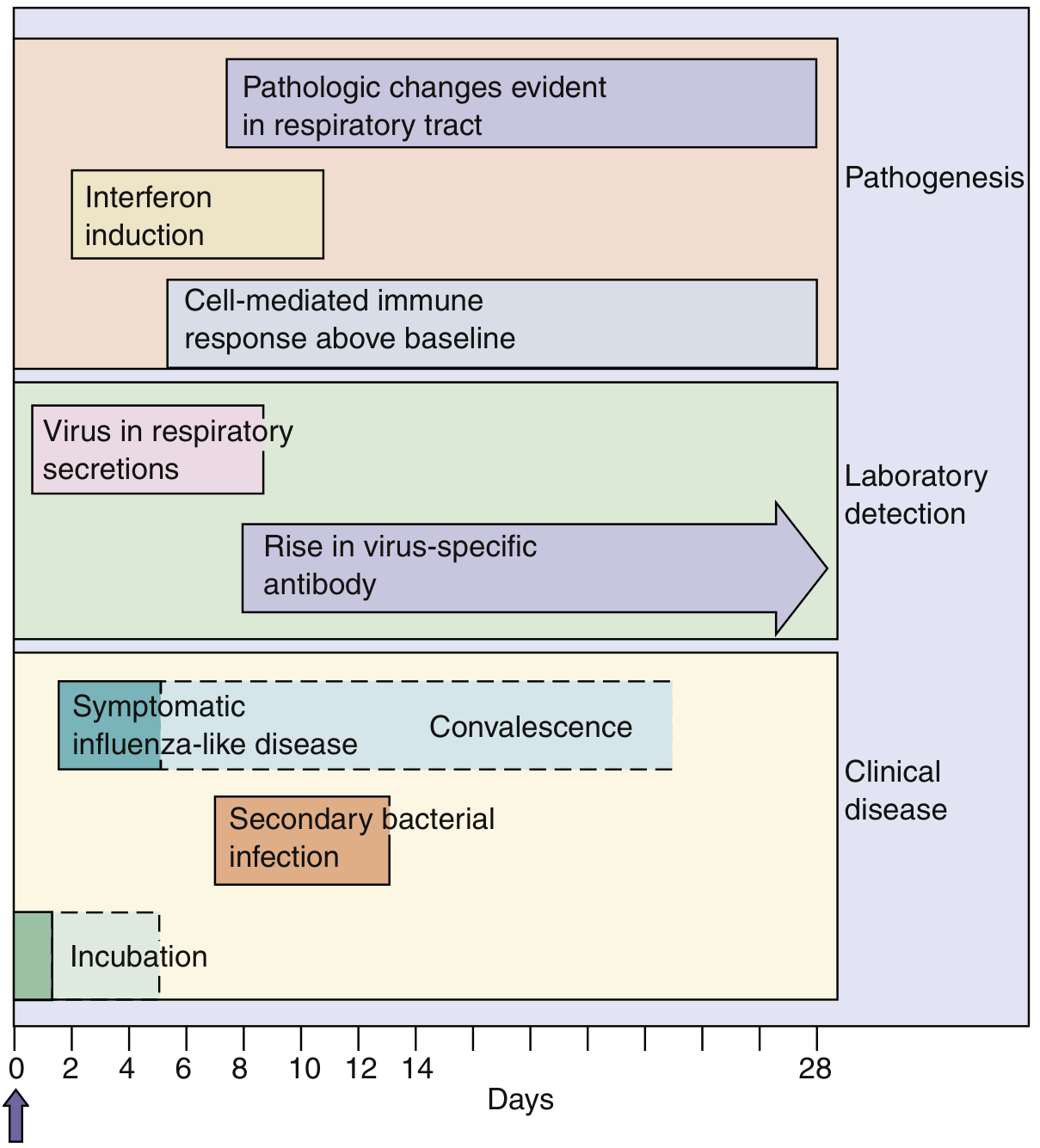
Medical Microbiology 9e - Time course of influenza A virus infection. Secondary bacterial pneumonia can occur in the subacute phase.
4. Epidemiology
Outbreaks of influenza A attack 10-20% of the general population; pandemics can affect >50%. Infection rates are highest in children; severe complications and deaths are most common in high-risk groups.
Annual US Burden (2010-2023)
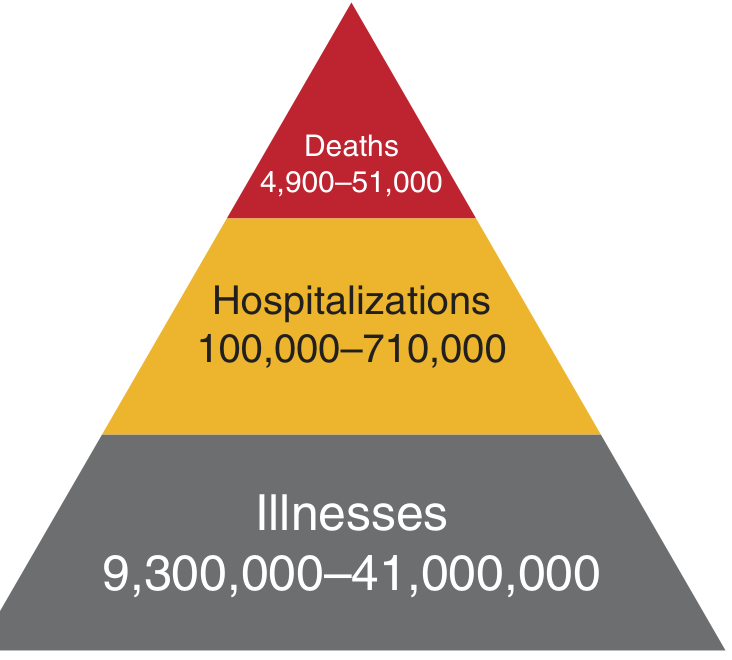
Harrison's Principles of Internal Medicine 22E - Annual influenza burden in the United States, 2010-2023 (CDC data).
5. Clinical Features
Incubation period: 48-72 hours (short for a viral illness)
Classic "flu syndrome" - adults can often date symptoms to the hour:
- Abrupt onset high fever
- Throbbing headache, photophobia
- Severe myalgia and malaise
- Sore throat, substernal soreness
- Non-productive cough
- Disabling fatigue
Constitutional symptoms often dominate over respiratory symptoms. Presentation varies by age:
- Children: fever, rhinitis, pharyngitis, vomiting, diarrhea
- Elderly: high fever, nasal obstruction, lassitude, diarrhea
6. Complications
Pneumonia is the major life-threatening complication. Three patterns:
- Primary influenza pneumonia - direct viral pneumonitis; persistent high fever and dyspnea >3-4 days; more common in elderly, immunocompromised, and pregnant women (but can affect young adults)
- Secondary bacterial pneumonia - most commonly Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae; follows initial improvement then relapse
- Mixed viral-bacterial pneumonia
Other complications:
- Myocarditis (influenza A and B are established causes)
- Encephalitis/neurologic complications
- Rhabdomyolysis
- Exacerbation of COPD, asthma, heart failure
7. High-Risk Groups (Priority for Vaccination and Treatment)
-
Adults ≥65 years
-
Children 6 months - 5 years
-
Pregnant women (and up to 2 weeks postpartum)
-
Residents of nursing homes and long-term care facilities
-
Persons with chronic medical conditions (cardiac, pulmonary, renal, hepatic, neurologic, hematologic, metabolic disorders including diabetes)
-
Immunocompromised individuals (HIV, chemotherapy, steroids)
-
Morbidly obese (BMI ≥40)
-
American Indian/Alaska Native populations
-
Health care personnel
-
Harrison's Principles of Internal Medicine 22E, Table 206-2
8. Diagnosis
Rapid influenza diagnostic tests (RIDTs)
- Results in ~15 minutes
- Sensitivity: ~50-70%; specificity: ~90-95%
- A negative test does NOT exclude influenza when the patient has compatible symptoms during active community circulation
RT-PCR (molecular testing) - gold standard; higher sensitivity than RIDTs; can distinguish type and subtype
Viral culture - confirmatory but slow (days to weeks); used for surveillance
Key point: During influenza season, treat based on clinical presentation even with a negative rapid test if symptoms are compatible.
9. Treatment - Antiviral Drugs
| Drug | Class | Route | Comments |
|---|---|---|---|
| Oseltamivir (Tamiflu) | Neuraminidase inhibitor | Oral | First-line; start within 48h of symptom onset; 5-day course; drug of choice in pregnancy |
| Zanamivir (Relenza) | Neuraminidase inhibitor | Inhaled | Alternative; avoid in bronchospasm |
| Peramivir | Neuraminidase inhibitor | IV | For hospitalized patients unable to take oral/inhaled |
| Baloxavir marboxil | Cap-dependent endonuclease inhibitor | Oral | Single dose; approved for uncomplicated influenza |
| Amantadine/Rimantadine | M2 ion channel inhibitors | Oral | Active only vs. influenza A; widespread resistance limits current use |
When to treat:
-
All hospitalized patients: start antivirals (oseltamivir) as soon as possible regardless of time from onset
-
High-risk outpatients: treat when influenza is suspected/confirmed
-
Otherwise healthy outpatients: consider if within 48 hours of symptom onset
-
Treatment should begin as early as possible; do not withhold in severely ill patients even if >48 hours have elapsed
-
Harrison's Principles of Internal Medicine 22E, p. 1590; Tintinalli's Emergency Medicine; Creasy & Resnik's Maternal-Fetal Medicine
10. Vaccination
Annual influenza vaccination is the cornerstone of prevention. The vaccine is reformulated each year to match projected circulating strains, based on WHO surveillance.
Types of Vaccines
- Inactivated influenza vaccine (IIV) - licensed >60 years; injected; safe in pregnancy
- Recombinant influenza vaccine (RIV) - FDA-approved 2017; avoids egg-adaptation issues
- Live attenuated influenza vaccine (LAIV) - intranasal; preferred in children (ages 2-49 years); not for pregnant women or immunocompromised
- High-dose and adjuvanted vaccines - preferred for adults ≥65 years; superior immunogenicity and effectiveness vs. standard dose
Effectiveness
Meta-analysis of RCTs showed pooled efficacy of ~59% (95% CI 51-67%) for inactivated vaccines in adults aged 18-65 years in matched seasons. Effectiveness is lower in mismatched years. Despite imperfect efficacy, vaccination reduces ICU admissions in children by ~74% and deaths by ~65% (observational data).
Vaccine Safety Notes
- Common: local injection site reactions
- Rare: Guillain-Barré syndrome (identified in 1976 vaccine; risk very small)
- Adjuvanted vaccines: more local pain/erythema
- LAIV: avoid in asthma/immunocompromised patients
Starting 2024-2025, the US vaccine is trivalent (B/Yamagata lineage removed as it has not circulated since March 2020).
- Harrison's Principles of Internal Medicine 22E, pp. 1589-1591
11. Prevention Beyond Vaccination
- Hand hygiene and respiratory etiquette (cough/sneeze into elbow)
- Droplet/contact precautions in healthcare settings (airborne precautions for aerosol-generating procedures)
- Post-exposure chemoprophylaxis with oseltamivir or zanamivir (75 mg oseltamivir once daily for 10 days) for high-risk contacts during outbreaks
- Avoid contact with sick individuals during the infectious period (1 day before to ~5-7 days after symptom onset)
Sources: Harrison's Principles of Internal Medicine 22E, p. 1587-1591 | Medical Microbiology 9e, p. 554-557 | Textbook of Family Medicine 9e, p. 274 | Tintinalli's Emergency Medicine | Creasy & Resnik's Maternal-Fetal Medicine | Murray & Nadel's Textbook of Respiratory Medicine
Pneumonia
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Pneumonia
1. Definition and Overview
Pneumonia is an infection of the lung parenchyma leading to consolidation of the normally air-filled alveoli. It can be caused by bacteria, viruses, fungi, mycobacteria, and atypical organisms. It is the leading cause of death from infection in adults >65 years in the United States, causes >1 million hospitalizations per year, and together with influenza ranks as the eighth leading cause of death overall in the US.
- Annual incidence: 16-23 per 1,000 adults
- ~30% of CAP patients require hospitalization; mortality among outpatients <5%, rising to 12-40% in hospitalized patients
- Overall annual cost: ~$17 billion (US)
2. Classification
Pneumonia is classified primarily by setting of acquisition, as this strongly predicts likely pathogens and guides empiric therapy:
| Type | Definition |
|---|---|
| CAP - Community-Acquired Pneumonia | Acquired outside hospital or within 48h of admission in a patient not recently hospitalized |
| HAP - Hospital-Acquired Pneumonia | Onset ≥48h after hospital admission |
| VAP - Ventilator-Associated Pneumonia | Onset ≥48-72h after endotracheal intubation |
| Aspiration Pneumonia | Inhalation of oropharyngeal/gastric contents |
3. Etiology and Common Pathogens
Community-Acquired Pneumonia (CAP)
"Typical" bacteria:
- Streptococcus pneumoniae (pneumococcus) - most common proven cause; accounts for ~2/3 of CAP with positive blood cultures
- Haemophilus influenzae - especially in COPD/smokers
- Staphylococcus aureus - especially post-influenza, cavitary/necrotizing pneumonia
- Klebsiella pneumoniae - especially in alcoholics
- Moraxella catarrhalis - COPD
"Atypical" bacteria (intracellular; no cell wall; not covered by beta-lactams alone):
- Mycoplasma pneumoniae - younger patients, community outbreaks
- Chlamydophila pneumoniae - insidious onset, mild disease
- Legionella spp. - hotel/cruise ship exposure, water systems; can be severe
Viruses: Influenza A/B, SARS-CoV-2, RSV, parainfluenza, adenovirus
Epidemiologic Clues to Pathogen (Harrison's Table 131-2)
| Exposure/Risk Factor | Likely Pathogen(s) |
|---|---|
| Alcoholism | S. pneumoniae, oral anaerobes, Klebsiella, M. tuberculosis |
| COPD/smoking | H. influenzae, P. aeruginosa, S. pneumoniae, M. catarrhalis |
| Structural lung disease | P. aeruginosa, S. aureus |
| Dementia/aspiration | Oral anaerobes, gram-negative enteric bacteria |
| Lung abscess | CA-MRSA, anaerobes, endemic fungi, TB |
| Hotel/cruise ship (past 2 wks) | Legionella spp. |
| Exposure to birds | Histoplasma, Chlamydia psittaci |
| Exposure to sheep/goats/parturient cats | Coxiella burnetii (Q fever) |
| Southwest US travel | Coccidioides spp., Hantavirus |
| Immunosuppression/HIV | P. jirovecii, Cryptococcus, Histoplasma, atypical mycobacteria |
Hospital-Acquired (HAP) and Ventilator-Associated (VAP) Pneumonia
Pathogens are more resistant than CAP organisms:
- S. aureus (including MRSA)
- Pseudomonas aeruginosa
- Gram-negative enteric bacilli (Klebsiella, Enterobacter, E. coli, Acinetobacter)
Risk factors for MDR pathogens in VAP:
- IV antibiotic use within prior 90 days
- Septic shock at time of VAP
- ARDS preceding VAP
- ≥5 days in hospital before VAP onset
- Acute renal replacement therapy before VAP
4. Pathogenesis and Pathophysiology
Infection follows failure of host defenses to clear microorganisms that reach the lower respiratory tract. Routes of entry include:
- Microaspiration of oropharyngeal secretions (most common)
- Inhalation of aerosolized droplets
- Hematogenous spread
Once infection is established, alveolar inflammation leads to fluid and cellular exudate filling the alveoli - the hallmark of consolidation. The resulting hypoxemia is primarily due to increased perfusion of shunt units (consolidated, non-ventilated alveoli) and low V/Q units. In severe pneumonia, shunt fraction can exceed 20%, causing refractory hypoxemia.
Classic lobar consolidation (typical bacterial): 4 stages:
- Congestion - vascular engorgement, edema
- Red hepatization - alveoli fill with red blood cells, fibrin, PMNs
- Grey hepatization - RBCs lyse; fibrin, PMNs persist
- Resolution - enzymatic digestion, macrophage clearance
5. Clinical Features
Typical (Bacterial) Pneumonia
- Abrupt onset with high fever, rigors/chills
- Productive cough (purulent or rust-colored sputum in pneumococcal pneumonia)
- Pleuritic chest pain
- Dyspnea
- Physical exam: decreased breath sounds, dullness to percussion, bronchial breathing, egophony, tactile fremitus over consolidation
- WBC typically >15,000/mm³ with neutrophilia
Atypical Pneumonia
- Gradual onset over days
- Low-grade fever, less impressive constitutional symptoms (the "walking pneumonia" pattern)
- Dry, non-productive cough
- Extrapulmonary features common (headache, rash, arthralgias - especially Mycoplasma)
- Often younger patients
- Chest X-ray may appear worse than symptoms suggest
Age-specific features:
- Children: Tachypnea is the earliest and most sensitive sign; intercostal retractions; viral pneumonias appear less toxic (low-grade fever, wheeze); bacterial pneumonias appear more acutely ill with high fever
- Elderly: May present atypically - confusion, falls, functional decline without classic respiratory symptoms; fever may be absent
6. Diagnosis
Clinical Diagnosis
Presumptive diagnosis based on:
- New respiratory symptoms (cough, dyspnea, chest pain)
- Fever
- New infiltrate on chest imaging
- Supporting exam findings
Imaging
- Chest X-ray - standard initial investigation
- Bacterial (typical): lobar/segmental consolidation, air bronchograms, alveolar infiltrates
- Atypical: bilateral interstitial or patchy infiltrates, often perihilar
- Viral: bilateral interstitial pattern, hyperinflation
- Note: CXR findings typically lag the clinical course by 1-2 days and can be normal on day 1
- Parapneumonic pleural effusions may be present
- CT chest - more sensitive; useful when CXR inconclusive or complications suspected (abscess, empyema)
Laboratory
- CBC with differential (leukocytosis with left shift in bacterial; leukopenia can indicate severe disease)
- Metabolic panel (urea/BUN - part of CURB-65 scoring)
- Sputum Gram stain and culture - low yield but useful if obtained correctly before antibiotics
- Blood cultures - recommended before antibiotics in hospitalized patients (quality indicator); bacteremia in ~15-20% of pneumococcal pneumonia
- Urinary antigen tests: Legionella (serogroup 1) and S. pneumoniae - rapid, highly specific
- Cold agglutinins: positive in Mycoplasma pneumoniae (sensitivity ~50%)
- Procalcitonin - elevated in bacterial infection; useful to guide antibiotic duration
- RT-PCR/molecular panels - highly sensitive for respiratory viruses, Mycoplasma, Legionella; increasingly used
When to perform invasive procedures
Bronchoscopy with BAL or protected brush specimen reserved for:
- Immunocompromised patients
- Failure to respond to empiric therapy
- VAP diagnosis
- Suspected unusual pathogens
7. Severity Assessment and Site of Care
Two validated tools for deciding outpatient vs. inpatient vs. ICU:
CURB-65 Score (preferred for simplicity)
| Variable | Score |
|---|---|
| Confusion (new disorientation to time/place/person) | 1 |
| Urea/BUN >7 mmol/L (>20 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure: systolic ≤90 or diastolic ≤60 mmHg | 1 |
| Age ≥65 years | 1 |
Interpretation:
- Score 0-1: Low risk - outpatient treatment
- Score 2: Moderate risk - consider short inpatient admission
- Score ≥3: High risk - hospital admission; consider ICU if score ≥4-5
- PSI class V and CURB-65 ≥3 may need ICU
Important: Scoring tools guide but do not replace clinical judgment. Also consider: ability to maintain oral intake, comorbidities, living situation, compliance, oxygenation (pulse oximetry), and social support.
Indications for hospitalization
- Failure to respond to or tolerate oral antibiotics
- Significant hypoxemia (SaO₂ <90% on room air)
- Multilobar consolidation
- Parapneumonic empyema
- Immunosuppression
- Lung abscess or pneumatocele
- Underlying cardiopulmonary disease
- Age extremes (infants <2 months, elderly)
ICU admission criteria (ATS/IDSA major criteria)
- Septic shock requiring vasopressors
- Acute respiratory failure requiring mechanical ventilation
8. Treatment
Outpatient CAP (low severity, no comorbidities)
| Patient Group | Recommended Antibiotics |
|---|---|
| Previously healthy, no recent antibiotics | Amoxicillin 1g TID, OR doxycycline, OR macrolide (azithromycin/clarithromycin) |
| Comorbidities (COPD, diabetes, renal/cardiac disease, immunosuppression) OR recent antibiotic use | Respiratory fluoroquinolone (levofloxacin, moxifloxacin) monotherapy OR beta-lactam + macrolide combination |
Inpatient CAP (non-ICU)
- Beta-lactam (ampicillin-sulbactam, ceftriaxone, or cefotaxime) + macrolide, OR
- Respiratory fluoroquinolone monotherapy
Severe CAP (ICU)
- Beta-lactam + macrolide, OR beta-lactam + respiratory fluoroquinolone
- Add MRSA coverage (vancomycin or linezolid) if: cavitary pneumonia, post-influenza, necrotizing pneumonia, gram-positive cocci on Gram stain
- Add P. aeruginosa coverage (anti-pseudomonal beta-lactam) if: structural lung disease (bronchiectasis), recent broad-spectrum antibiotics, prior Pseudomonas isolation
HAP/VAP Treatment
Empiric therapy based on local antibiogram. Core principles:
- Cover MSSA with: piperacillin-tazobactam, cefepime, meropenem, imipenem, or levofloxacin
- Add vancomycin or linezolid if MRSA rate >10-20% or risk factors present
- Use two antipseudomonal agents from different classes if MDR risk factors present or gram-negative resistance rates >10%
- De-escalate once culture/sensitivity results are available
Aspiration Pneumonia
- Routine anaerobic coverage is NOT necessary unless: poor dentition, lung abscess, or necrotizing pneumonia
- If community-acquired: amoxicillin-clavulanate or clindamycin
- If hospital-acquired: piperacillin-tazobactam or carbapenem
Duration of Therapy
- Minimum 5 days for CAP; continue at least 48-72 hours beyond clinical stability (afebrile, improved respiratory status)
- Atypical organisms (Legionella, Mycoplasma): typically 10-14 days (fluoroquinolone or macrolide)
- HAP/VAP: 7 days if clinically responding; shorter courses supported by evidence
9. Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion | Occurs in ~40% of bacterial pneumonias; if exudative (Light's criteria), requires drainage |
| Empyema | Pus in pleural space; requires chest tube drainage + antibiotics; especially common with S. pyogenes (30-40%) |
| Lung abscess | Cavitation with air-fluid level; anaerobes, CA-MRSA, Klebsiella; requires prolonged antibiotics |
| ARDS | Severe pneumonia can trigger diffuse alveolar damage |
| Septicemia/bacteremia | ~15-20% in pneumococcal CAP |
| Respiratory failure | Requires supplemental O₂, non-invasive ventilation, or intubation |
| Organizing pneumonia | If infiltrates fail to resolve, consider bronchiolitis obliterans organizing pneumonia (BOOP) |
10. Prevention
Vaccination (cornerstone of prevention)
Pneumococcal vaccines:
- PCV20 (20-valent pneumococcal conjugate vaccine) - recommended for all adults ≥65 and high-risk adults ≥19 years (immunocompromised, chronic lung/liver/kidney/heart disease, diabetes, CSF leak, cochlear implants, cigarette smokers)
- PCV15 + PPSV23 sequence is an alternative for adults ≥65
- Re-vaccination with PPSV23 after 10 years if first dose given before age 65
Influenza vaccine annually - reduces secondary bacterial pneumonia (a major complication of influenza)
General measures
- Smoking cessation (smoking is a major risk factor for pneumococcal pneumonia and impairs mucociliary clearance)
- Hand hygiene
- Avoid aspiration risk (upright positioning after meals, good oral hygiene)
- Appropriate infection control in hospitals (hand hygiene, care bundles for VAP prevention including head-of-bed elevation 30-45°, oral chlorhexidine, subglottic suctioning, daily sedation interruption)
11. Differential Diagnosis
Conditions that can mimic pneumonia on imaging:
- Pulmonary embolism (most common cause of "atypical pneumonia" - always consider)
- Congestive heart failure with pulmonary edema
- Hypersensitivity pneumonitis
- Bronchiolitis obliterans organizing pneumonia (BOOP/COP)
- Acute eosinophilic pneumonia
- Pulmonary hemorrhage (Goodpasture's syndrome, mitral stenosis)
- Foreign body aspiration
- Connective tissue diseases (lupus pneumonitis, RA-associated ILD)
- Lung malignancy
Recent Evidence (2025-2026)
A 2025 systematic review and meta-analysis (Nakagawa et al., Eur Respir Rev) identified risk factors for drug-resistant pathogens in CAP - emphasizing that prior antibiotic use remains the strongest predictor of resistant organisms. New 2026 ATS Clinical Practice Guidelines (Jones et al., Am J Respir Crit Care Med, Jan 2026) provide updated recommendations on CAP diagnosis and management - these represent the most current guidance and may update prior ATS/IDSA 2019 recommendations.
Sources: Harrison's Principles of Internal Medicine 22E, pp. 1068-1080 | Textbook of Family Medicine 9e, pp. 271-275, 321-322 | Current Surgical Therapy 14e (HAP/VAP section) | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.