ARYTHMYIA
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative textbooks plus the key diagram. Here is the full answer:
Arrhythmia: Mechanisms and Pathophysiology
Cardiac arrhythmias arise from abnormalities in the initiation and/or propagation of the cardiac electrical impulse. There are three core mechanisms: abnormal automaticity, triggered activity (afterdepolarizations), and reentry. - Harrison's Principles of Internal Medicine, 22E, p.1956
1. Normal Cardiac Impulse Propagation (Background)
The normal impulse originates in the sinoatrial (SA) node, travels across the atria via preferential pathways (including Bachmann's bundle), reaches the AV node - where conduction slows (reflected as the PR interval) - then propagates through the bundle of His, right and left bundle branches, and finally the Purkinje fiber network to activate the ventricular myocardium.
Key conduction velocities:
- Purkinje fibers: 2-3 m/s
- Ventricular myocardium: 0.3-0.4 m/s
Ionic basis of the action potential (AP):
-
Phase 0 (rapid upstroke): Na⁺ and Ca²⁺ inward currents
-
Phases 1-2 (plateau): K⁺ channels open slowly; Na/Ca channels inactivate
-
Phase 3 (repolarization): K⁺ outward currents dominate
-
Phase 4 (resting): quiet in atrial/ventricular myocytes; spontaneous depolarization ("funny current", I_f) in nodal tissues driven by a nonselective Na/Ca channel - the target of ivabradine
-
Harrison's Principles of Internal Medicine, 22E, p.1954-1956
2. Mechanism I: Abnormal Automaticity
Definition: Automaticity = spontaneous phase 4 depolarization. Normally this is a property of the SA node, AV node, and His-Purkinje system. When automaticity of a distal tissue exceeds the SA node rate, it takes over as pacemaker ("escape rhythm").
Pathologic enhanced automaticity occurs when:
- The rate of phase 4 depolarization accelerates beyond normal in conduction tissues (SA node, AV node, His-Purkinje)
- Non-nodal tissues acquire automaticity in disease states: border zones of infarcted myocardium, pulmonary veins (trigger for paroxysmal AF), coronary sinus, SVC, ventricular outflow tracts
- Ischemia, reperfusion, or injury alters membrane properties to create new automatic foci
Clinical examples:
- Accelerated junctional rhythm, accelerated idioventricular rhythm (AIVR)
- Premature ventricular contractions (PVCs) from ischemic border zones
- Atrial tachycardia (AT) from ectopic foci
- Pulmonary vein ectopy triggering paroxysmal AF
Autonomic regulation is key: increased adrenergic tone accelerates phase 4 depolarization; vagal tone slows it. - Harrison's Principles of Internal Medicine, 22E, p.1956
3. Mechanism II: Triggered Activity (Afterdepolarizations)
Definition: Abnormal depolarizations occurring in the late phases of the AP that are "triggered" by a preceding AP and can initiate sustained arrhythmias.
A. Early Afterdepolarizations (EADs)
- Occur during phases 2-3 of the AP
- Facilitated by intracellular Ca²⁺ loading and AP prolongation
- Heterogeneous QT prolongation across the ventricles allows EADs to trigger wavefronts
- Result in Torsades de Pointes (TdP) - a polymorphic VT that can degenerate into VF
Precipitants of EADs:
- QT-prolonging drugs (antiarrhythmics, antibiotics, antipsychotics)
- Hypokalemia, hypomagnesemia
- Bradycardia
- Electrical remodeling in cardiomyopathies
- Inherited Long QT syndrome (LQTS)
B. Delayed Afterdepolarizations (DADs)
- Occur during phase 4 of the AP (after full repolarization)
- Mechanism: excess intracellular Ca²⁺ drives repetitive spontaneous depolarizations via the Na/Ca exchanger
- Can produce sustained arrhythmia including bidirectional VT
Precipitants of DADs:
-
Digitalis glycoside toxicity (classic cause)
-
Catecholamine excess
-
Ischemia/reperfusion
-
Heart failure with Ca²⁺ overload
-
Harrison's Principles of Internal Medicine, 22E, p.1957
4. Mechanism III: Reentry (Most Common Tachyarrhythmia Mechanism)
Definition: Circus movement of an electrical wavefront that perpetually re-excites the same tissue. This is the most common mechanism of tachyarrhythmias. - Washington Manual of Medical Therapeutics, p.231
Requirements for reentry (all three must be present):
- An anatomic or functional circuit - a closed loop of conductive tissue
- Unidirectional block - the wavefront can propagate in only one direction at the site of block (the other direction is refractory or blocked)
- Slow conduction - within part of the circuit, conduction is slow enough that the rest of the circuit recovers excitability before the wavefront returns
Anatomic Reentry
- Fixed barrier (scar, annulus fibrosus, accessory pathway) defines the circuit
- Predictable, regular, and often terminable by pacing
- Examples: AVNRT (AV nodal reentry tachycardia), AVRT (accessory pathway), atrial flutter (cavotricuspid isthmus), scar-based VT post-MI
Functional Reentry
- No fixed anatomic barrier; instead, a region is functionally refractory
- Circuit varies in size and location; frequency of depolarization varies
- More complex; more difficult to terminate
- Likely mechanism for: atrial fibrillation (multiple wavelets) and some forms of VF
Premature beat as a trigger: A premature impulse may find one pathway refractory (unidirectional block) while conducting through the other - if that pathway conducts slowly enough, the originally blocked pathway recovers and the impulse re-enters, establishing the circus loop.
- Harrison's Principles of Internal Medicine, 22E, p.1957
Summary Diagram
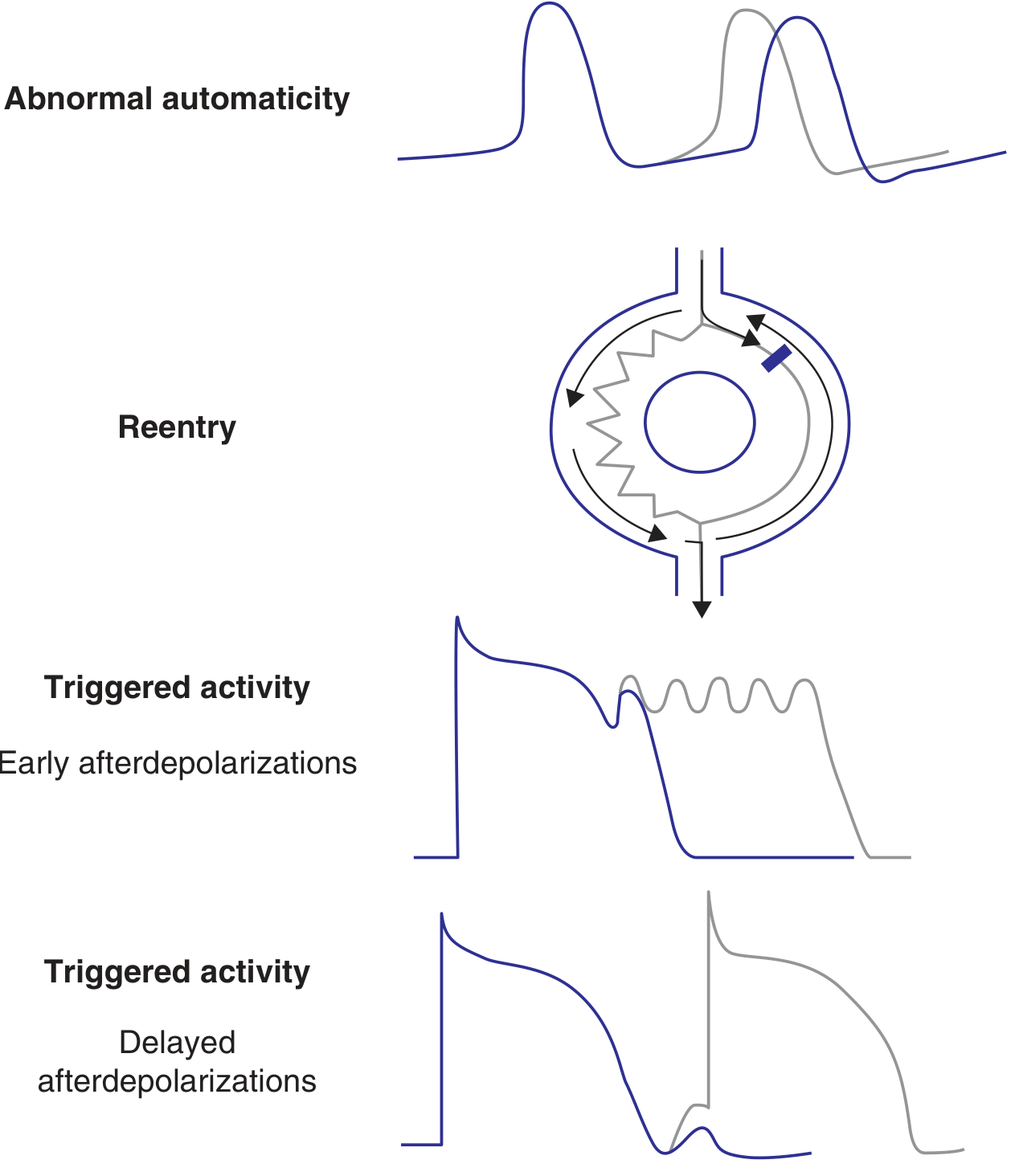
FIGURE 250-3 from Harrison's 22E: Schematic action potentials showing EADs, DADs, reentry circuit, and abnormal automaticity
Summary Table (Harrison's 22E, Table 250-1)
| Category | Mechanism | Prototypical Arrhythmia |
|---|---|---|
| Abnormal automaticity | Enhanced phase 4 depolarization | Idiopathic VT, atrial tachycardia, AIVR |
| Triggered activity - EADs | Phase 2-3 afterdepolarizations | TdP in long QT syndrome, PVCs |
| Triggered activity - DADs | Phase 4 afterdepolarizations (Ca²⁺ overload) | Digitalis-induced VT/AT, reperfusion PVCs |
| Reentry | Unidirectional block + slow conduction | AVNRT, AVRT, atrial flutter, scar-related VT |
Clinical Clues to Mechanism
| Feature | Likely Mechanism |
|---|---|
| Sudden onset and abrupt termination of palpitations | Reentry |
| Terminates with Valsalva / carotid sinus massage | AV nodal reentry (AVNRT) |
| Gradual warm-up and cool-down | Enhanced automaticity |
| Long QT on baseline ECG | EAD-triggered TdP |
| Digitalis toxicity | DADs |
| Post-MI sustained VT | Scar-based anatomic reentry |
| Paroxysmal AF | Pulmonary vein automaticity triggering functional reentry |
- Washington Manual of Medical Therapeutics, p.231; Fuster and Hurst's The Heart, 15th Edition, p.1061
This is a shared conversation. Sign in to Orris to start your own chat.