Cerebellum
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Basal ganglia physiology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compose the full answer.
Basal Ganglia Physiology
Overview
The basal ganglia are a collection of gray matter nuclei deep within the cerebral hemispheres that play a central role in the planning, initiation, and regulation of voluntary movement. They also contribute to cognitive, affective, and motivational functions. Critically, the basal ganglia have no direct projections to the spinal cord - they exert their influence entirely through a loop back to the motor cortex via the thalamus.
Anatomical Components
The basal ganglia consist of five main structures (Ganong's):
| Structure | Division | Transmitter |
|---|---|---|
| Caudate nucleus | Striatum (input) | GABA (medium spiny neurons) |
| Putamen | Striatum (input) | GABA |
| Globus pallidus external (GPe) | Intrinsic nucleus | GABA |
| Globus pallidus internal (GPi) | Output nucleus | GABA |
| Subthalamic nucleus (STN) | Input/intrinsic | Glutamate |
| Substantia nigra pars compacta (SNpc) | Input/modulator | Dopamine |
| Substantia nigra pars reticulata (SNpr) | Output nucleus | GABA |
- The caudate + putamen = striatum (the main input structure)
- The putamen + globus pallidus = lenticular nucleus
- ~95% of striatal neurons are medium spiny neurons (GABAergic); the remainder are aspiny interneurons (cholinergic, somatostatinergic, GABAergic)
The Cortico-Basal Ganglia-Thalamo-Cortical Loop
The overall architecture is a re-entrant loop:
Cerebral Cortex → Striatum → GPi/SNpr → Thalamus (VL nucleus) → Motor Cortex
The cortex provides the main excitatory (glutamatergic) input to the striatum. The thalamus receives inhibitory output from GPi/SNpr (GABAergic) and projects back excitatorily to premotor and supplementary motor areas. The basal ganglia thus modulate cortical motor activity rather than commanding it directly. - Neuroanatomy through Clinical Cases 3rd Ed., p. 778
Direct and Indirect Pathways
This is the core physiological model. The two pathways have opposing net effects on the thalamus and therefore on movement:
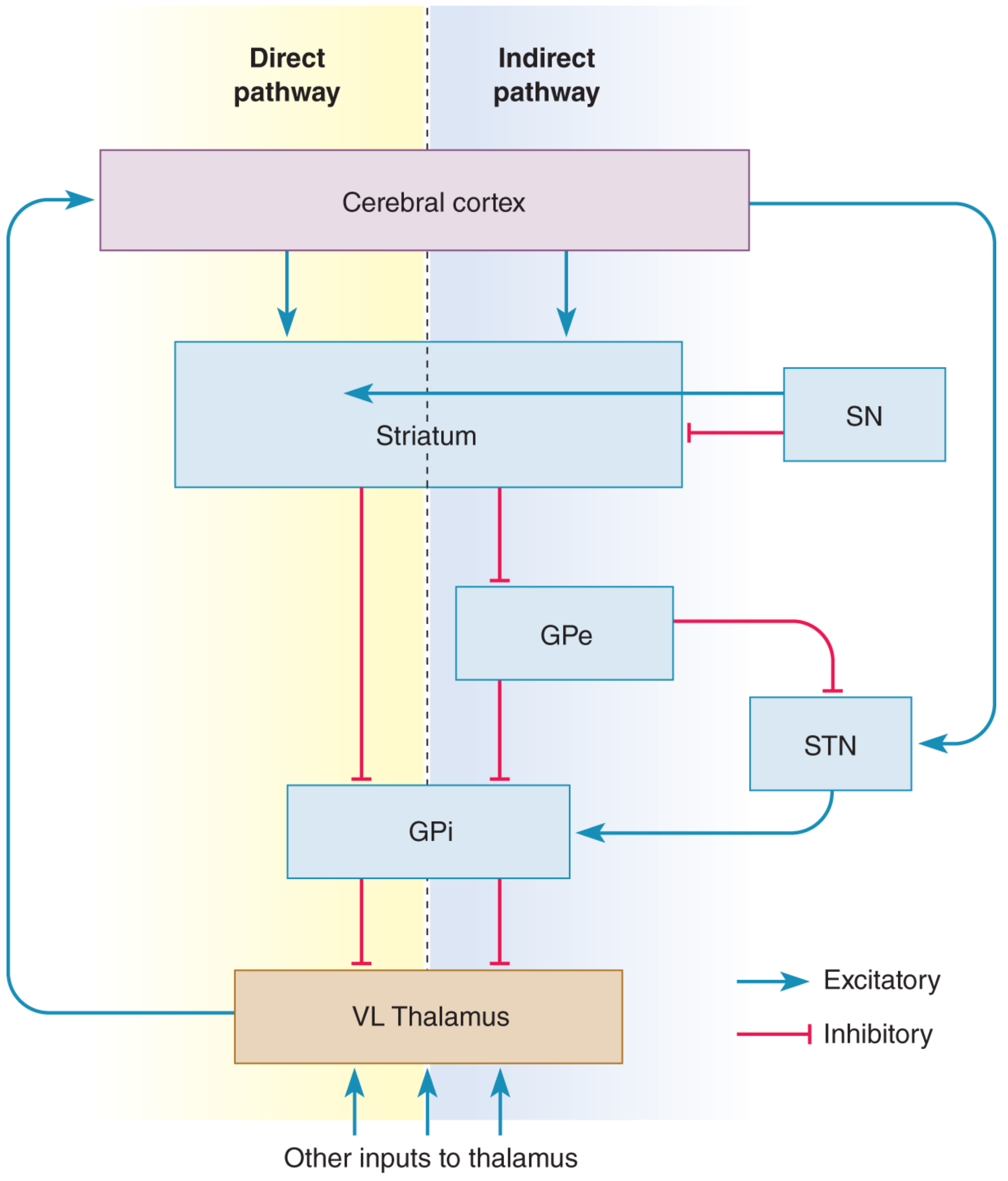
Direct Pathway (pro-kinetic - facilitates movement)
Cortex → Striatum → GPi/SNpr → Thalamus → Motor Cortex
Step-by-step:
- Cortex excites striatal neurons (glutamate)
- Striatum inhibits GPi (GABA)
- GPi tonically inhibits the thalamus - this inhibition is now released
- Thalamus becomes active, exciting motor cortex (SMA)
- Net result: movement facilitated
The key insight is that GPi neurons are spontaneously active at rest, so they tonically suppress thalamic activity. The direct pathway releases this brake. Using signed arithmetic: two inhibitions = net excitation (-1 × -1 = +1). - Neuroscience: Exploring the Brain, 5th Ed., p. 1353
Indirect Pathway (anti-kinetic - suppresses movement)
Cortex → Striatum → GPe → STN → GPi/SNpr → Thalamus → Motor Cortex
Step-by-step:
- Cortex excites striatum (glutamate)
- Striatum inhibits GPe (GABA)
- GPe normally inhibits STN - this inhibition is released, so STN becomes active
- STN excites GPi (glutamate)
- GPi inhibits thalamus more strongly (GABA)
- Motor cortex receives less excitation
- Net result: movement suppressed
Three inhibitions = net inhibition (-1 × -1 × -1 = -1). The cortex also provides a direct excitatory input to the STN (the "hyperdirect pathway"), which further drives GPi inhibition of the thalamus and acts as an emergency "stop" signal. - Costanzo Physiology 7th Ed., p. 3473
Neurotransmitter Summary
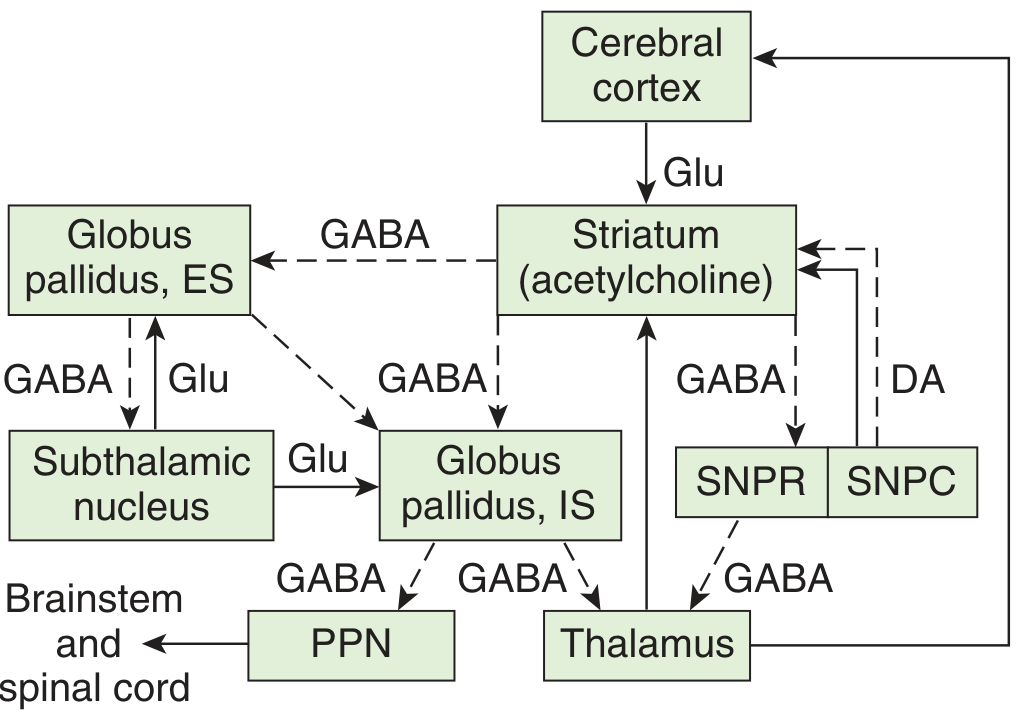
Inputs to the basal ganglia:
- Corticostriatal: Glutamate (excitatory)
- Thalamostriatal (intralaminar nuclei): Glutamate (excitatory)
Within the basal ganglia:
- Striatum → GPe and GPi: GABA (inhibitory)
- GPe → STN: GABA (inhibitory)
- STN → GPi and GPe: Glutamate (excitatory)
- SNpc → Striatum: Dopamine (D1 and D2 receptors, see below)
- Striatum → SNpr: GABA
- Striatal interneurons: Acetylcholine
Outputs from the basal ganglia:
- GPi → Thalamus: GABA (inhibitory)
- SNpr → Thalamus and brainstem: GABA (inhibitory)
Dopamine Modulation: D1 and D2 Receptors
Dopamine from the SNpc is the key modulator of basal ganglia balance:
| Receptor | Pathway | Effect on Striatum | Net Effect on Thalamus |
|---|---|---|---|
| D1 | Direct | Excitatory | More thalamic activation (facilitates movement) |
| D2 | Indirect | Inhibitory | Less thalamic inhibition (facilitates movement) |
Both D1 and D2 receptor activation ultimately favor movement:
- D1 boosts the direct (pro-kinetic) pathway
- D2 suppresses the indirect (anti-kinetic) pathway
Dopamine therefore acts as a "gain control" mechanism on the basal ganglia loop. Loss of dopamine (as in Parkinson's disease) simultaneously reduces direct pathway drive AND increases indirect pathway drive, causing net over-inhibition of the thalamus and therefore hypokinesia. - Neuroanatomy through Clinical Cases 3rd Ed., p. 778
Functional Loops
The basal ganglia are not a single circuit - they are organized into at least five parallel, functionally segregated loops (Kandel, Principles of Neural Science 6th Ed.):
| Loop | Input Region | Striatal Target | Function |
|---|---|---|---|
| Motor | Motor/premotor cortex | Putamen | Voluntary movement control |
| Oculomotor | Frontal eye field | Caudate (body) | Saccadic eye movements |
| Prefrontal (dorsolateral) | DLPFC | Caudate (head) | Working memory, cognition |
| Orbitofrontal | Orbitofrontal cortex | Caudate (ventromedial) | Impulse control, reward |
| Limbic | Anterior cingulate, amygdala | Nucleus accumbens (ventral striatum) | Motivation, emotion, reinforcement |
This explains why basal ganglia disorders can produce not only movement abnormalities but also cognitive deficits, psychiatric symptoms, and compulsive behaviors.
Role in Action Selection
A major functional concept from Kandel (6th Ed.) is that the basal ganglia serve as a selection mechanism - they help choose one behavior from several competing options. The GPi tonically suppresses all movements via its inhibitory output to the thalamus; when a specific movement is selected, focused striatal activity releases ("disinhibits") only the relevant thalamic neurons while keeping others suppressed. This focused disinhibition is the final functional expression of basal ganglia output.
Dopamine and Reinforcement Learning
The dopaminergic system encodes reward prediction errors (Kandel). Phasic dopamine release signals when an outcome is better than expected (positive prediction error), reinforcing the actions that led to the reward. This mechanism underlies habit formation and learning of motor skills, and is co-opted by addictive drugs that flood the dopamine system.
Diseases of the Basal Ganglia
Three pathways normally operate in balance: (1) nigrostriatal dopaminergic, (2) intrastriatal cholinergic, (3) striato-pallidal GABAergic. Disruption produces two classes of disorders: - Ganong's Review of Medical Physiology 26th Ed., p. 253
Hypokinetic Disorders
Parkinson's Disease:
- Degeneration of dopaminergic neurons in SNpc (mainly nigrostriatal fibers to putamen)
- Loss of D1 reduces direct pathway → thalamus under-activated
- Loss of D2 fails to suppress indirect pathway → thalamus over-inhibited
- Clinical: akinesia, bradykinesia, cogwheel rigidity, resting tremor (4-6 Hz)
- Rigidity differs from spasticity - affects both agonist and antagonist muscles ("lead pipe" quality)
- Treatment: L-DOPA + carbidopa, dopamine agonists (bromocriptine, pramipexole), anticholinergics
Hyperkinetic Disorders
Huntington's Disease:
- CAG trinucleotide repeat expansion → degeneration of striatal medium spiny neurons
- Early loss preferentially affects indirect pathway (enkephalin-containing neurons projecting to GPe)
- GPe disinhibited → inhibits STN → GPi under-active → thalamus disinhibited → excess movement
- Clinical: chorea (rapid, involuntary "dancing" movements), then dementia, then death within 10-15 years
- Later stages: both pathways degenerate → rigid hypokinetic state
Hemiballismus:
- Usually a lesion of the subthalamic nucleus (e.g., lacunar infarct)
- STN normally excites GPi; without it, GPi is less active → thalamus disinhibited
- Clinical: wild, flinging movements of the contralateral extremities
Athetosis: slow, writhing involuntary movements (often striatal lesions)
Chorea: rapid, involuntary, "dancing" semipurposeful movements
Key Principles Summary
- No direct spinal output - the basal ganglia work entirely through the cortex-thalamus-cortex loop
- Tonic inhibition - GPi/SNpr tonically suppress the thalamus; movement occurs via disinhibition
- Direct pathway = pro-kinetic (net: removes thalamic inhibition)
- Indirect pathway = anti-kinetic (net: increases thalamic inhibition)
- Dopamine facilitates movement via D1 (direct) and D2 (indirect) receptors
- Ipsilateral vs. contralateral: basal ganglia lesions affect the contralateral side of the body (unlike cerebellar lesions which are ipsilateral)
- Hyperkinetic = too much disinhibition of thalamus; hypokinetic = too much inhibition of thalamus
- Parallel loops - motor, cognitive, limbic circuits run in parallel through segregated parts of the BG
Sources: Ganong's Review of Medical Physiology 26th Ed. | Costanzo Physiology 7th Ed. | Neuroscience: Exploring the Brain 5th Ed. | Neuroanatomy through Clinical Cases 3rd Ed. | Kandel Principles of Neural Science 6th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.